IJCRR - 9(3), February, 2017
Pages: 24-27
Date of Publication: 10-Feb-2017
Print Article
Download XML Download PDF
Hematological and Bone Marrow Biopsy Evaluation in Non Hodgkin Lymphoma
Author: Kanwalpreet Kaur1, Nidhi Sharma2, Karuna Gupta3, Sandhya Gulati4, Prerana Choudhary5
Category: Healthcare
Abstract:Aim: Bone marrow evaluationis an integral part of staging workup in patients with Non-Hodgkin's lymphoma (NHL). Aim of this study is to analyze incidence and histological pattern of bone marrow involvement in diagnosed cases of NHL.
Methodology: This is a retrospective study on 85 patients diagnosed with NHL. Bone marrow biopsy was performed under local anesthesia as a part of staging workup in cases of NHL. Complete blood counts (CBC) were also noted in each case.
Results: In this study, NHL cases comprised of low grade NHL 68.2%, intermediate grade 28.2% and high grade 3.5%. The age ranged from 10 to 75 years and M: F ratio was 1.07:1. 38.8% (33/85) cases showed bone marrow involvement. Majority of bone marrow involvement was seen in indolent lymphomas (87.8%). Most common pattern of involvement was mixed (12/33) followed by diffuse (9/33), interstitial (8/33) and nodular (4/33). 87.9% cases showed increase in reticulin which included reticulin grade 1(9/33), grade 2(14/33) and grade 3(6/33). Only 48.5% cases of bone marrow involved cases had CBC abnormalities while 51.5% were completely normal. CBC abnormalities included anemia (5/16), leucopenia (3/16), leukocytosis (8/16) and thrombocytopenia (9/16).
Discussion: In the present study, bone marrow involvement by non-Hodgkin lymphoma was seen in 38.8% cases. Other studies also described the incidence of bone marrow involvement from 27.6% to 53%. Predominant involvement was observed in indolent cases which were similarly noted in other studies.
Conclusion: Bone marrow biopsy is an essential part of staging work up of NHL affecting the prognosis and treatment.
Keywords: Non Hodgkin lymphoma, Bone marrow infiltration, Hemogram
Full Text:
Introduction
Non Hodgkins lymphoma (NHL) includes heterogenous group of neoplasms each with distinct clinical, morphological, immunophenotypic, genetic features and different response to therapy. The incidence of NHL for India was estimated to be 2.2/100,000 with 23,801 new cases[1]. Bone marrow (BM) evaluation is an essential part of staging work up in NHL (modified Ann Arbor staging). The aim of this study was to analyze the incidence and histological pattern of bone marrow involvement in diagnosed cases of situs slot.
Material and methods
This was a retrospective study on 85 patients diagnosed with NHL. Bone marrow biopsy was performed as a part of routine staging workup. Informed consent was taken from each patient before the procedure and performa containing basic information of patient including age, sex and indication of procedure was filled. Bone marrow biopsy was performed under local anesthesia from posterior iliac spine using Jamshidi needle. It was fixed in Bouin’s solution, decalcified in 5% nitric acid for two hours followed by routine paraffin embedding and processing. Multiple serial sections stained with Hematoxylin and eosin and reticulin were examined for histological pattern of infiltration and fibrosis. Complete blood counts (CBC) were also noted in each case by a five part automated analyser.
Results
This study included 85 cases diagnosed with NHL who underwent BM evaluation as a part of staging work up over one year. International working formulation was followed to classify NHL as low, intermediate and high grade. In this study, NHL cases comprised of low grade NHL 68.2%, intermediate grade 28.2% and high grade 3.5%. The age ranged from 10 to 75 years and M: F ratio was 1.07:1.
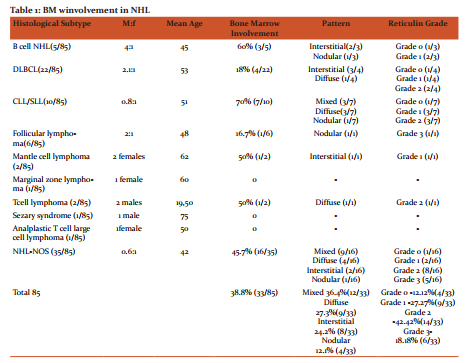
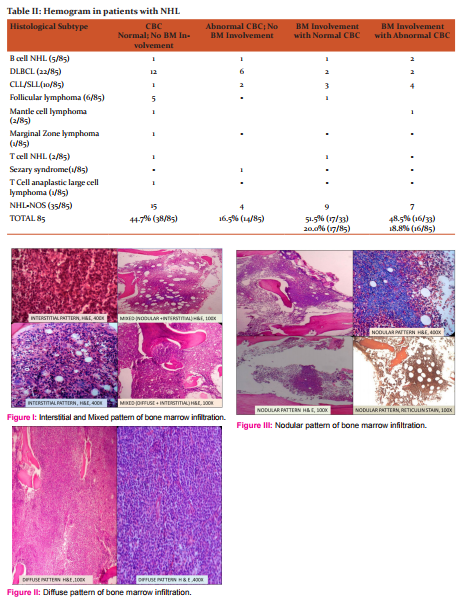
Bone marrow involvement was seen in 38.8% (33/85) cases. Majority of bone marrow involvement was seen in indolent lymphomas (87.8%) while 12.1% of aggressive lymphomas showed BM involement. None of the highly aggressive lymphoma showed infiltration in BM. Most common pattern of involvement was mixed (12/33) [figure1] followed by diffuse (9/33) [figure2], interstitial (8/33) [figure1] and nodular (4/33) [figure 3]. Increase in reticulin was noted in 34.1% cases which included reticulin grade 1(9/33), grade 2(14/33) and grade 3(6/33). (table 1)
CBC abnormalities were seen in 30 patients. NHL cases without BM involvement showed abnormalities in CBC in 16.5% cases while only 18.8% cases of NHL with BM infiltration showed abnormalities in CBC. Only 48.5% cases of bone marrow involved cases had CBC abnormalities while 51.5% were completely normal(table 2). There was no significant association between abnormal hemogram and BM involvement by NHL on applying Fisher Exact test (P value = 0.062).
CBC abnormalities included anemia(5/16), leukocytosis (8/16), leukopenia (3/16) and thrombocytopenia (9/16) in NHL cases with BM involvement while in NHL cases without BM infiltration showed CBC abnormalities as anemia (10/30), leukocytosis (8/30), leukopenia (2/30) and thrombocytopenia(14/30). Unilineagecytopenia was seen in 5cases, bilineagecytopenia in 10 cases while pancytopenia in 4 cases.
Discussion
In the present study, bone marrow involvement by non-Hodgkin lymphoma was seen in 38.8% cases. Other studies also described the incidence of bone marrow involvement from 27.6% to 53%[2-9]. The reason of difference in incidence of BM involvement is due to differences in histological subtypes in different studies and time elapsed between initial diagnosis of NHL and BM evaluation.
In the present study, majority of bone marrow involvement was seen in indolent lymphomas (87.8%). It was similar to studies of Tarek et al.[8] and Mokhtar et al.[10] which also showed the predominance of marrow involvement in indolent lymphomas.
Small lymphocytic lymphoma (SLL) showed highest incidence of marrow involvement (70%). It was in concordance with results of study of Suneet et al. [7] and Prateek et al. [11]. Diffuse large B cell Lymphoma (DLBCL) had relatively lower frequency of spread of lymphomas to BM (18%). However other studies showed involvement upto 33%[8].This was because most of the tumours in our study were not typed at the time of BM evaluation. They were diagnosed as NHL on fine needle aspiration.
Most common pattern of involvement was mixed (12/33) followed by diffuse (9/33), interstitial (8/33) and nodular (4/33) in this study. It was similar to findings of Arber et al [6] and Suneet et al. [7] however, Foucar et al. [3] found focal involvement to be the predominant pattern. It was because of the large sample size of study with most common lymphoma being follicular lymphoma. Lim et al [9] reported diffuse pattern as the most pattern of involvement.
In this study, 87.9% cases showed increase in reticulin which included reticulin grade 1(9/33), grade 2(14/33) and grade 3(6/33). Increased reticulin deposition is restricted to the areas of infiltration. Reticulin stain is useful in detecting scanty interstitial infiltrates which are not so evident on H&E stains. However, reticulin fibrosis did not correlate with NHL grade. This was similar to findings of study of Prateek et al.[11]
Only 48.5% cases of bone marrow involved cases had CBC abnormalities while 51.5% were completely situs judi slot online deposit pulsa tanpa potongan. This was similar to results of Prateek et al [11]in which 46.8% of NHL showed BM involvement with CBC abnormalities. Abnormal hemogram findings were not useful to predict BM infiltration in NHL. The same was concluded by studies of Hiorns et al12 and Prateek et. al[11].
Conclusion
Bone marrow biopsy is an essential part of staging work up of NHL affecting the prognosis and treatment. Indolent lymphomas showed higher rate of bone marrow involvement than highly aggressive lymphomas. Abnormal hemogram findings did not reveal any correlation with bone marrow infiltration.
References:
- Nair R. Arora N. Mallath M.K. Epidemiology of Non-Hodgkin's Lymphoma in India. Oncology 2016;91:18-25.
- Brunning RD, Bloomfield CD, McKenna RW, Peterson L. Bilateral trephine biopsies in lymphoma and other neoplastic conditions. Ann Intern Med 1975;82:365-6.
- Foucar K, McKenna RW, Frizzera G, Brunning RD. Bone marrow and blood involvement by lymphoma in relationship to the Luke-Collins classification. Cancer 1982;49:888-97
- Varma N, Dash S, Sarode R, Marwah N. Relative efficacy of bone marrow trephine biopsy sections as compared to trephine imprints and aspiration smears in routine hematological practice. Indian J Pathol Microbiol 1993;36:215-26
- Schmid C, Isaacson PG. Bone marrow trephine biopsy in lymphoproliferative diseases. J Clin Pathol 1992;45:745-50.
- Arber DA, George TI. Bone marrow biopsy involvement by non-?Hodgkin's lymphoma: frequency of lymphoma types, patterns, blood involvement, and discordance with other sites in 450 specimens. Am J Surg Pathol 2005;29:1549-57.
- Kumar S, Rau AR, Naik R, Kini H, Mathai AM, Pai MR, Khadilkar UN. Bone marrow biopsy in non-Hodgkin lymphoma: a morphological study. Indian J PatholMicrobiol. 2009 Jul-Sep;52(3):332-8.
- Tarek MN, Bolkainy E, Deif WSA, Gouda HM, Mokhtar NM. Evaluation of Bone marrow in 143 Lymphomas: the relative frequency and pattern of involvement, secondary myelopathies, pitfalls and diagnostic validity. Journal of the egyptian nat. cancer inst.2008;20:17-30
- Lim EJ, PehSC.Bone marrow and peripheral blood changes in non-Hodgkin's lymphoma. Singapore Med J. 2000 Jun;41(6):279-85.
- Mokhtar N, Khaled H (editors). Lymphoma, 1st edition, Cairo, Cairo University Press. 2002,23:0138-190.
- Bhatia P, Das R, Ahluwalia J, Malhotra P, Varma N, Varma S, Trehan A, and Marwaha RK. Hematological Evaluation of Primary Extra Nodal Versus Nodal NHL: A Study from North India. Indian J Hematol Blood Transfus. 2011 Jun; 27(2): 88–92.
- L. R. Hiorns, J. Nicholls, J. P. Sloane, A. Horwich, S. Ashley, and M. Brada. Peripheral blood involvement in non-Hodgkin's lymphoma detected by clonal gene rearrangement as a biological prognostic marker.Br J Cancer. 1994 Feb; 69(2): 347–351.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





