IJCRR - 6(9), May, 2014
Pages: 37-40
Print Article
Download XML Download PDF
AN AUDIT OF APPROPRIATE USAGE OF BLOOD PRODUCTS IN BLOOD BANK IN A TERTIARY CARE HOSPITAL RAJKOT
Author: Ankita A. Katara , Amit H. Agravat, Gauravia Dhruva, Jagdish D. Dalsania, Rutvi G. Dave
Category: Healthcare
Abstract:Transfusion of blood and blood products such as Whole Blood, Red Cell Concentrate, Platelet Concentrate, and Fresh Frozen Plasma play an important role in treating hospitalised patients. The irrational use of medical technology is a major factor in increased healthcare expenses. We have done a crossectional studyto estimate the appropriate usage of blood and blood products transfusions in P.D.U. Medical College and Hospital, Rajkot,Gujarat,(India). Methodology: We analysed 1050 blood and blood products requests for transfusion. A total of 1078 blood and blood products transfusions were evaluated in these patients. A review of the patients medical record was done on each request for blood and blood products for examplediagnosis, indication for transfusion, number of units requested and the speciality prescribing it. Overall prevalence of appropriate use of blood and blood products was assessed according to NACO (National AIDS Control Organization) guidelines. Results: A total of 1050 requests were received for blood and blood products transfusion from various departments .These patients received 1078 transfusions.Maximum number of blood transfusion requests were received from Obstetrics and Gynecology department. Maximumnumber of transfusions were done in Medicine department. Out of these total transfusions, Red Cell Concentrates were maximum. According to our study maximum inappropriate transfusions were of Red Cell Concentrates.Total prevalence of appropriate use of blood and blood products was 81%. Conclusion: There is a need for continuous auditabout the use of blood and blood products as therapy. This helps in reduction of prevalence of inappropriate use of blood products, thus thereby reduces the expenditure on health care.
Keywords: whole blood, RCC (Red Cell Concentrate, PC(Platelet Concentrate), FFP(Fresh Frozen Plasma), Prevalenceof appropriate use
Full Text:
INTRODUCTION
Blood transfusion has become a very important part of modern health care. If used correctly, it can save life and improve health.However, like other therapeutic interventions, it may result in various types of complications. In addition, it carries the riskof transmission of infections like HIV (Human Immunodeficiency Virus), HBV (Hepatitis B Virus), HCV (Hepatitis C Virus), Syphilis etc. It is also expensive and uses a scarcehuman resource. Inappropriate use causes increase in health expenditure and also puts patients at higher risk in acquiring Transfusion Transmitted Infections.The risks associated with transfusion can only be decreased by collaboration between the blood transfusion service and clinicians in managing the blood components for transfusion, approach of both should be to provide an adequate supply of safe blood and blood products and the effective clinical use of blood and blood products There is no any absolute acceptable level for all patients exists. But the concept of transfusion is only indicated when Hemoglobin<7 g/dl. This concept has been accepted as general in most of the countries in the world1 .The blood component implies separation of whole blood into various potential components like packed red cells, platelet concentrate and fresh frozen plasma2-5 .To increase the efficacy, safety and utilizationof blood and blood components clinicians and hematologists should have knowledge regarding the potential risk associated with blood component therapy6 . Various strategies have been developed to reduce the inappropriate use of blood components. These includeguidelines and consensus conferences as well as monitoring of transfusion practice, educationand self-audit by clinicians5,7,8 .
MATERIALS AND METHODS
A crossectional study was done to estimate the appropriate use of blood and blood products transfusions in Blood Bank at P.D.U. Medical College and Hospital, Rajkot, Gujarat,(India). A review of the patients medical record was done on each request for blood and blood products for example diagnosis, indication for transfusion, number of units requested and the speciality prescribing it.
RESULTS
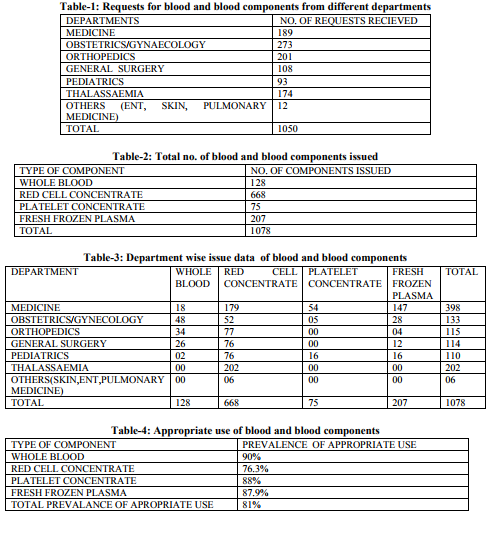
A total of 1050 requests were received. Out of which189 requests were from medicine, 273 from gynaecology, 201 from orthopaedics, 108 from general surgery, 93 from paediatrics, 174 from thalassaemia ward and 12 from others (skin, ENT, pulmonary medicine) [TABLE-1]. These patients received 1078 transfusions. Total number of transfusions done in medicine was 398, obstetrics and gynecology 133, orthopaedics 115, general surgery 114, paediatrics 110 ,thalassaemia 202 and others 06 respectively [TABLE-3]. Out of total 1078 transfusions Whole Blood were 128, Red Cell Concentrate were 668, Platelet Concentrate were 75 and Fresh Frozen Plasma were 207 [TABLE-2]. Prevalence of appropriate use of Whole Blood , Red Cell Concentrate, Platelet Concentrate and Fresh Frozen Plasma was 90%, 76.3%, 88% and 87.9% respectively [TABLE-4]. Prevalence for appropriate use of Blood and Blood components for all departments was 81% [TABLE-4].
DISCUSSION
Maximum number of blood transfusion requests were received from Obstetrics and Gynecology department. Maximum number of transfusions were done in Medicine department. Out of these total transfusions, Red Cell Concentrates were maximum. According to our study maximum inappropriate transfusions were of Red Cell Concentrates. Due to easy availability of blood and blood components, indiscriminate use of blood components is on arise. To reduce that internal audits should be regularly done as a part of the quality control programme in any blood bank9-10 . These Internal quality programs aims at proper selection of blood components and avoid their overuse11-12.The demand for blood and its components is increasing day by day,but the supply is limited. High rate of inappropriate use causes considerable impact on the health care cost, wastage of resourcesand increased risk of transmission transmitted infections. First reason for limited appropriate use of blood component is use of laboratory criteria alone to determine the request of transfusion. Ideally clinical status and laboratory reports should be considered. Second reason is, denial to issue blood can cause conflicts between clinician and laboratory personnels and may also lead to medicolegal issues, ultimately compromising patient care.Third reason is lack of any oversight program to monitor quality of transfusion practices.
CONCLUSION
Inappropriate use of blood and its products can be reduced effectively through various stratigies such as Medical audits, Continuing Medical Education and various educational stratigies including blood bank personnels and clinicians.In addition to their economic impact, these educational programs improve appropriate use of blood components and also have impact on the rate of transfusion transmitted diseases.
ACKNOWLEDGEMENT
I am highly indebted to my wonderful mentors, colleagues and last but not the least my Head of the Department for their guidance, constant supervision and immense support in completing the project. These are the persons who were always there for me in my all ups and downs. I would like to express my immense gratitude towards my parents, my mentors & members of my institute (P.D.U Medical College and Hospital, Rajkot, Gujarat, (INDIA) for their kind cooperation and encouragement which helped me in completion of this article successfully.
References:
REFERENCES
1. Hospital Transfusion Committee Centre Hospital Macao.Blood Transfusion A clinician’s reference. First Edition;2005.
2. Metz J, McGrath KM, Copperchini ML, Haeusler M, Haysom HE, et al. Appropriateness of transfusions of red cells, Platelets and fresh frozen plasma. An audit in a tertiary care teaching hospital.Med J Aust1995; 162: 572-573, 576-7.
3. Luk C, Eckert KM, Barr RM, Chin-Yee IH. Prospective audit of the use of fresh-frozen plasma, based on Canadian Medical Association transfusion guidelines.CMAJ 2002;166: 1539-1540.
4. Toy PT. Audit and education in transfusion medicine. Vox Sang 1996;70: 1-5.
5. Barnette RE, Fish DJ, Eisenstaedt RS. Modification of fresh-frozen plasma transfusion practices through educational intervention. Transfusion 1990;30: 253-257.
6. Vishwanathan C, Jain R, KamathM.Blood utilization review in a tertiary care hospital. Indian J Haematol Blood Transf1999;17: 26– 31.
7. Solomon RR, Clifford JS, GutmanSI.The use of laboratory intervention to stem the flow of fresh-frozen plasma. Am J ClinPathol1988;89: 518-521.
8. Brien WF, Butler RJ, InwoodMJ.An audit of blood component therapy in a Canadian general teaching hospital. CMAJ 1989;140: 812-815.
9. McCullough J, Steeper TA, Connelly DP, Jackson B, Huntington S, et al. Platelet utilization in a university hospital. JAMA 1988;259: 2414-2418.
10. Silver H, Tahhan HR, Anderson J, Lachman M. A non-computer dependent prospective review of blood and blood component utilization. Transfusion 1992;32: 260-265
11. Brandis K, Richards B, Ghent A, Weinstein S. A strategy to reduce inappropriate red blood cell transfusion.Med J Aust 1994;160: 721- 722.
12. Joshi GP, Landers DF.Audit in transfusion practice.J EvalClinPract1998;4: 141-146.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





