IJCRR - 6(11), June, 2014
Pages: 71-78
Date of Publication: 13-Jun-2014
Print Article
Download XML Download PDF
STUDY OF LEFT VENTRICULAR MASS IN CHRONIC SEVERE ANEMIA
Author: Farquana Qushnood, Ruqia Asna, Salim A. Dhundasi, K. K. Das
Category: Healthcare
Abstract:Background and Objectives: In chronic anemia the heart has to entertain a hyperdynamic circulation in order to compensate for reduced oxygen carrying capacity of blood. Chronic alterations of cardiac workload results in changes of LV geometry. The diagnosis of left ventricular hypertrophy (LVH) based on LV mass has been incorporated in the clinical practice as an important marker of CVD. Hence, present study was undertaken with the objective of estimating the LV mass in pts with chronic severe anemia and comparing with controls. Methodology: Present study was conducted in Al-Ameen Medical College and District Hospital, Bijapur. 31 anemic patients (aged 18-40 yrs) with Hb ? 7 gm% and equal no. of age and gender matched normal subjects were selected. All anemic patients and controls were subjected for hemoglobin estimation and M mode 2D Echocardiography. Echocardiographic parameters IVSTd, LVPWd, LVIDd were studied, LVM and LVMI were derived. Statistics-by Student's unpaired't' test, correlation analysis. Results: Our study demonstrated increased LVM and LVMI in anemic patients compared to controls. Both correlated negatively with Hb levels. Interpretation and Conclusion: Left ventricular mass is an independent risk factor for prediction of cardiovascular events.Echocardiography is a simple, noninvasive imaging method in the evaluation of cardiac morphology and dynamics, hence can be used to evaluate LVM in chronic anemia. The findings of increased LVM and LVMI in anemic patients of our study are indicative of LV hypertrophy. Hypertrophy of cardiac myocytes occurs to meet the demand of increased rate of use of mechanical energy in response to sustained Hemodynamic overloading of the heart.
Keywords: Left ventricular Mass, Chronic anemia, LVH, Echocardiography.
Full Text:
INTRODUCTION
Chronic severe anemia is a common disease. Optimal tissue oxygenation requires the functional integrity of heart, lungs and blood. If one of this fails in joint task, the other has to carry extra load. In chronic anemia the heart has to entertain a hyper dynamic circulation in order to compensate for reduced oxygen carrying capacity of blood. Such profound and chronic alterations of cardiac workload results in changes of left ventricular geometry.1 Anemia significantly alters circulatory dynamics and so burdens circulatory system.Hemodynamic changes brought about by this condition have consequences that could both predispose and aggravate existing cardiac disease. One potential mechanism for the adverse health effects associated with chronic anemia may be an increased cardiac output, which may lead to the development of ventricular dilation, increased LV mass (LVM), and LV hypertrophy (LVH). In turn, LVM and LVH are well established predictors of cardiovascular morbidity and mortality. There is evidence to suggest that experimentally induced anemia causes myocardial hypertrophy in a rat model. The diagnosis of LVH has been incorporated in the clinical practice as an important marker of cardiovascular disease. Echocardiography has been clinically employed, becoming one of the most important noninvasive imaging methods in the evaluation of cardiac morphology and dynamics.2 Clinical studies suggest that correction of anemia causes regression of left ventricular hypertrophy.There are limited data,that have evaluated the relationship between chronic anemia with LVM or LVH. Hence the present study was undertaken with the objective of estimating the LV mass in patients with chronic severe anemia and comparing data with that of control group.
MATERIALS AND METHODS
The present study was undertaken in the department of physiology Al-Ameen Medical College, Bijapur. Thirty one (31) patients (20 females, 11 males) with severe anemia hemoglobin (Hb) ≤ 7gm%, between 18yrs to 40 yrs age visiting Al-Ameen medical college hospital and District Hospital Bijapur were selected. Equal number of age and gender matched individuals with normal Hb levels were controls. Patients presenting with acute blood loss, pregnancy, hypertension, any underlying heart disease, chronic obstructive pulmonary disease (COPD), patients with hyperdynamic circulatory states like hyperthyroidism, beriberi, AV fistulas were excluded from the study. All anemic patients underwent history taking and a thorough clinical examination. Physical parameters viz Height, Weight were recorded. Body surface area (BSA) in Sq. mts (m2 ) was calculated by Duboi’s nomogram. Their hemoglobin levels were estimated. Transthoracic Echocardiography was done using PHILIPS Envisor C (model no MCMD02AA) diagnostic Ultrasound System using 3.5 MHz transducer, probe (PA 4- 2) by physician experienced in Echocardiography. Measurements were made according to the recommendations of the American Society of Echocardiography (ASE) at end diastole and end systole.3 Echocardiographic parameters viz- LVPWd (Posterior wall thickness at end diastole), LVIDd (Left ventricular inner dimension at end diastole), IVSTd (septum thickness at end diastole)were recorded. Left ventricular mass was calculated in each case using Devereux formula.4 LV Mass= 1.04 [(LVIDD + PWTD +IVSTD)3 - (LVIDD)3 ]-13.6 gms Where 1.04 is the specific gravity of cardiac muscle. LV Mass index (LVMI) was calculated as LVM/Body surface area. LV Mass more than 131 gms in males and more than 90 gms in females were considered as abnormal and indicative of Left Ventricular Hypertrophy (LVH). Statistics: Student’s unpaired‘t’ test was performed (using Graph pad Prism 5 statistical software) to analyze the echocardiographic changes between anemic patients and control group. Pearsonscorrelation and regression analysis was applied to correlate Hb levels with LVM and LVMI in anemic pts. A ‘p’ value <0.05 was considered statistically significant. Percentage calculation was done with reference to values defining LVH in anemic pts.
RESULTS
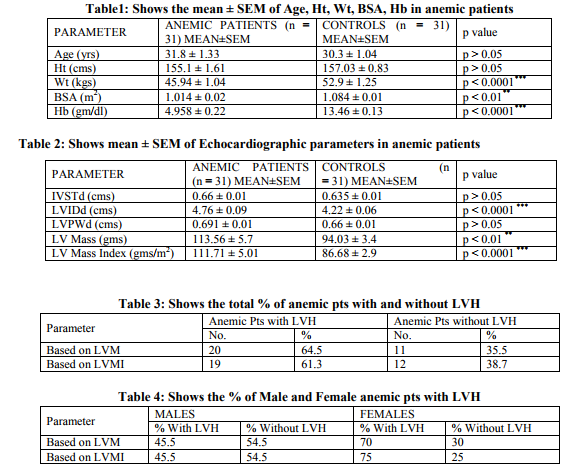
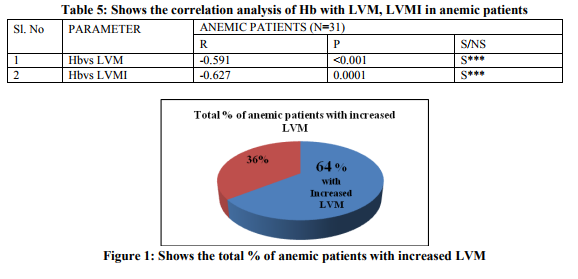
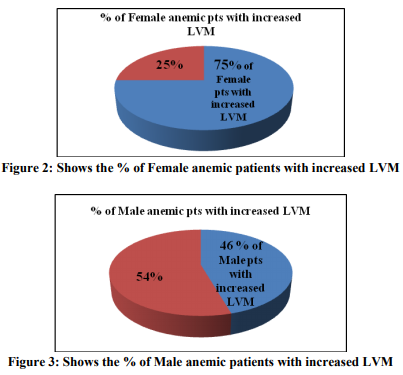
Thirty one patients with severe anemia having hemoglobin concentration less than 7 gm/dl, between 18 and 40 yrs of age were selected for this study. Equal no. of age and gender matched individuals with normal Hb levels were controls. Table No. 1 shows the mean ± SEM of age, Ht, Wt, BSA, Hb in anemic patients. The mean value of height was numerically more in controls than anemic pts which was not statistically significant; (t=1.07, p > 0.05). The mean weight of anemic patients was found to be less than that of controls, which was statistically significant; (t = 4.277, p < 0.0001). The mean value of BSA of anemic patients was more than that of controls, which was statistically significant; (t = 3.451, p < 0.01) and (t = 4.46, p < 0.0001) respectively. The mean ± SEM of hemoglobin in anemic patients was 4.958 ± 0.22 gm/dl; in controls 13.46 ± 0.13 gm/dl. Table No.2 shows mean ± SEM of Echocardiographic parameters in anemic patients. The mean value of IVSTd was numerically more in anemic patients as compared to the controls. But the difference was not statistically significant; (t = 1.692, p > 0.05).The mean value of LVIDd in anemic patients was 0.54 cms more as compared to that of controls. This difference was found to be highly statistically significant; (t = 5.064, p < 0.0001).The was no statistically significant between the mean value of LVPWd of anemic pts and controls; (t = 1.886, p > 0.05). Mean ± SEM of LVM in anemic pts was more 113.56 ± 5.7 gms, when compared to controls 94.03 ± 3.4 gms. This difference was statistically significant; (t = 2.94, p < 0.01). In anemic pts Mean ± SEM of LVMI was 111.71 ± 5.01 gms/m2 which was higher than that of controls 86.68 ± 2.9 gm/m2 , this difference turned out to be highly statistically significant; (t = 4.32, p < 0.0001). Table No.3 shows the total % of anemic pts with and without LVH. Based on the cutoff values of LV Mass of more than 131 gms in males and more than 90 gms in females, Left ventricular hypertrophy was found in 20 ptsi.e 64.5% of the total, where as 11 ptsi.e 35.5% of pts were without LVH. Fig 1 shows the same in pie chart form.However when corrected for body surface area, i.ebased on LVMI 19 pts (61.3%) showed LVH and 12 pts (38.7%) were found to be without LVH. Table No.4 shows the % of male and female anemic pts with LVH. 45.5% of male pts were found with LVH (Fig. 2). Based on LVM, 70% and based on LVMI 75% of female pts (Fig.3) were found to have LVH. Table No.5 shows the correlation analysis of Hb with LVM and LVMI in anemic patients.LVM showed statistically significant negative correlation with hemoglobin levels (r = -0.591, p < 0.001). Similar result was obtained when LVMI was correlated with Hb levels (r = -0.627, p < 0.0001).
DISCUSSION
Anemia is a common cause of morbidity in India especially in low socioeconomic group and is a serious health problem. It affects an estimated 50% of the population. According to NFHS (National Family Health Survey) II, 52% of women have some degree of anemia, 35% of women are mildly anemic, 15% are moderately anemic, and 2% are severely anemic.5 Takahashi M et.al 1990, conducted a study on 28 patients with iron deficiency anemia in which changes in hemodynamic parameters were observed before and after treatment in 14 subjects with moderate to severe anemia and then were compared with those of normal subjects. The LV diastolic diameter (LVIDd) as measured by Mmode echocardiography decreased after treatment in anemic patients. When compared with controls the values were higher in anemic patients.6 Patients with anemia had significantly larger left ventricles compared with control subjects as shown by the M mode left ventricular end diastolic dimensions (Bahl VK et al, 1992).7Our finding of an increased LVIDs is similar to other studies mentioned above. Probably this is due to the result of increased volume overload which in the long term causes hemodynamic alterations leading to gradual development of cardiac enlargement and LV hypertrophy. This LVH is eccentric, characterized by increased LV internal dimensions.8The transition from a high-output (compensated) cardiac state to a state of LV dysfunction (decompensated) appears to begin at a hemoglobin level of approximately 7 g/dL in anemic patient. As the hemoglobin level drops further, so does the LV function.9 Several factors have been shown repeatedly in epidemiologic studies to associate with LVH. Factors such as hematocrit have been implicated but with some inconsistency among different studies. Clinical validity and impact of such factors is controversial, but it may be important to consider them as relevant potential confounders in epidemiological studies investigating the role of novel risk factors in LVH and the role of LVH in disease prediction.4 Left ventricular mass (LVM) is an independent risk factor for prediction of cardio vascular events. Increased LVM in chronic anemia is well documented in animal models. Denis M. Medeirosand John L. Beard in their study reported the presence of eccentric cardiac hypertrophy in rats made anemic by feeding an iron-deficient diet.10In a cross sectional study of 175 patients attending a kidney disease clinic, the relationship of hemoglobin levels to echocardiographic findings was evaluated. The authors found that anemia and systolic blood pressure were the most modifiable risk factors associated with the presence of LV hypertrophy. In multiple logistic regression analysis, each 1g/ dL decrease in hemoglobin was associated with a 6% increase in risk of LV hypertrophy.11The physiologic response to anemia is a compensatory increase in cardiac output in order to maintain adequate oxygen delivery. Exercise capacity falls in correlation to the degree of anemia.12 In a study by Manish G. Amin et.al 2004, 1376 men and 1769 women who were anemic were studied. The mean hematocrit (Hct) and LVMI were 46.5% and 41.9%, and 127.3 and 95.8 g/m, respectively, in men and women. After adjustment for confounders, each 3% lower Hct was associated with a 2.6 g/m higher mean LVMI in men, and a 1.8 g/m higher mean LVMI in postmenopausal women (p ≤0.05). There was a significant quadratic relationship between Hct and LVMI in premenopausal women (p ≤ 0.01).2 Left ventricular mass was significantly increased in thalassemic patients as compared to controls in a study on 20 thalassemic pts and 20 controls done to investigate the echocardiographic features in β thalassemia patients(Taksande A et.al, 2005).13Levin A et al. 1996, demonstrated in their study the high prevalence of LVH in patients with renal insufficiency and identified two modifiable factors as important predictors of LVH, of which anemia was one factor. For each 10 g/L decrease in hemoglobin, the risk of LVH increased by 6% (P = 0.0062).11 The findings of our study are in agreement with other studies mentioned above. We demonstrated an increased LVM and LVMI in anemic patients as compared to controls. Left ventricular hypertrophy was found in 64.5% of pts based on LVM and 61.5% pts based on LVMI. 75% of female and 45.5% of male anemic patients were found with left ventricular hypertrophy. Differences in LV mass due to gender, independent of questions related to body size, may have pathophysiological implications. Women have been shown to have an increased parietal hypertrophic response to overload even after body size correction.4 Our study demonstrated 75% of female anemic pts were found with increased LVM after correction for BSA. Left ventricular mass (LVM) is an independent risk factor for prediction of cardiovascular events. Increase in LVM, as related to cardiac remodeling, can be consequent to both an adaptive and a maladaptive process.Severe anemia is known to cause reduced oxygen carrying capacity of blood. Non hemodynamic and hemodynamic mechanisms operate to compensate for anemia. Increased CO is the main hemodynamic factor mediated by lower afterload, increased preload, positive chronotrophic and inotrophic effects. With decreased afterload, the venous return and LV filling increases leading to increased LVIDd as evidenced in our study. In the long term, these hemodynamic alterations lead to gradual development of cardiac enlargement and LV hypertrophy. This LVH is eccentric, characterized by increased LV internal dimensions.8 Pathologic hypertrophy serves as an important adaptive response to regional or global increases in systolic and/or diastolic wall stress. Initially, the increase in cardiac mass serves to normalize wall stress and permit normal cardio vascular function at rest and during exercise. Nevertheless, during the compensated phase of pathologic hypertrophy, distinct alterations in myocardial gene expression occur; and these changes may serve to maintain function in the context of increased wall stress. This results in eccentric left ventricular hypertrophy. Eccentric hypertrophy results in an overall increase in myocyte length without a substantial increase in myocyte cross-sectional area and is caused by the addition of new sarcomeres in series. Volume overload leads to new sarcomeres both in parallel and in series. Hypertrophy of myocardial myocytes occurs to meet the demand of increased rate of use of mechanical energy as a response to sustained hemodynamic overloading of the heart. 14Up to a point, the increased mass of cardiac muscle is beneficial in terms of normalizing wall stress and providing for a larger number of contractile elements. However, the capacity for new cardiac myocytes to form is limited.14 Chronic anemia leads to work hypertrophy of the heart and finally to its dilatation and cardiac failure. However none of our patients were in heart failure.When anemia related LVH develops in otherwise healthy individuals without cardiovascular risk, the lesions are reversible. Continuation of this study after correction of anemia would have been of interest.
CONCLUSION
Chronic anemia leads to work hypertrophy of the heart. Left ventricular mass is an independent risk factor for prediction of cardiovascular events. Echocardiography is a simple, noninvasive imaging method in the evaluation of cardiac morphology and dynamics, hence can be used to evaluate LVmass in chronic anemia. The findings of increased LVM and LVMI in anemic patients of our study are indicative of LV hypertrophy. Hypertrophy of myocardial myocytes occurs to meet the demand of increased rate of use of mechanical energy as a response to sustained hemodynamic overloading of the heart. There is limited data on LV mass in chronic anemia; hence further studies are required in this regard. Also continuation of this study after correction of anemia would have been of interest.
ACKNOWLEDGEMENT
Authors would like to thank all the participants of the study. Authors acknowledge the immense help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Heribert Schunkert, Hans W Hense. A heart price to pay for anemia.Nephrol Dial Transpalant 2001; 16: 445-448.
2. Manish G. Amin, HocineTighiouart, Daniel E. Weiner, Paul C. Stark, John L. Griffith, Bonnie MacLeod et.al. Hematocrit and Left Ventricular Mass:The Framingham Heart Study. J. Am. Coll. Cardiol. 2004; 43: 1276- 1282.
3. Stritzke J, Mayer B, Lieb W, Luchner A, Döring A, Hense HW, Schunkert H. Haematocrit levels and left ventricular geometry: Results of the MONICA Augsburg Echocardiographic Substudy. J Hpertens 2007 Jun; 25 (6):1301-9.
4. MuriloFoppa, Bruce B Duncan and Luis EP Rohde.Echocardiography based left ventricular mass estimation. How should we define hypertrophy.Cardiovascular Ultrasound 2005; 3(17): 1-13.
5. National Family Health Survey NFHS 2 India 1998- International Institute for Population Sciences, Mumbai, MEASURE DHS + ORC and MACRO.
6. Takahashi M, Kurokawa S, Tsuyusaki T, Kikawada R. Studies of hyperkinetic circulatory state in chronic anemia. J Cardiol 1990; 20 (2):331-9.
7. Bahl VK, Malhotra OP, Kumar D, Agarwal R, Goswami KC, Bajaj R, et al. Non-invasive assessment of systolic and diastolic left ventricular function in patients with chronic severe anemia: A combined M-mode, twodimensional, and Doppler echocardiographic study. Am Heart J 1992; 124: 1516-23.
8. Metivier F, Marchais SJ, Guerin AP, Pannier B, London GM. Pathophysiology of anaemia: Focus on the heart and blood vessels. Nephrol Dial Transplant 2000;15Suppl 3: 14-8.
9. Alvares JF, Oak JL, Pathare AV. Evaluation of cardiac function in iron deficiency anemia before and after total dose iron therapy. J Assoc Physicians India 2000; 48: 204-6.
10. Denis M. Medeirosand John L. Beard.Dietary Iron Deficiency Results in Cardiac Eccentric Hypertrophy in Rats. ProcSocExpBiol Med. 1998 Sep; 218(4): 370-5.
11. Levin A, Singer J, Thompson CR, Ross H, Lewis M. Prevalent left ventricular hypertrophy in the predialysis population: Identifying opportunities for intervention. Am J Kidney Dis. 1996 Mar; 27(3): 347-54.
12. Varat MA, Adolph RJ, Fowler NO. Cardiovascular effects of anemia.Am Heart J 1972; 83: 415-26.
13. Taksande A, Vilhekar K, Jain M, Ganvir B. Left ventricular systolic and diastolic functions in patients with sickle cell anemia. Indian Heart J 2005 Nov-Dec; 57(6): 694-7.
14. ValentinFuster, R. Wayne Alexander, Robert A.O Rourke, Robert Roberts, Spencer B. King III, Ira S. Nash et al. Hurst’s THE HEART. 11thed. New York: McGraw Hill companies; 2004.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





