IJCRR - 7(14), July, 2015
Pages: 21-26
Print Article
Download XML Download PDF
EFFECTIVENESS OF END-RANGE MOBILIZATION AND INTERFERENTIAL CURRENT OR STRETCHING EXERCISE AND MOIST HEAT IN TREATMENT OF FROZEN SHOULDER- A RANDOMIZED CLINICAL TRIAL
Author: Dhara N. Panchal, Charu Eapen
Category: Healthcare
Abstract:Background: Frozen shoulder, one of the leading causes of shoulder pain with incidence of 2% in India is frequently treated by physiotherapist. Very few studies have emphasized combination of modalities or comparison of combined treatments for frozen shoulder till date. Thus, there is a need to evaluate the effectiveness of combined treatments for better implications in clinical practice. This study was aimed at comparing the efficacy of end range mobilization (ERM) and interferential current therapy (IFT) with moist heat and stretching on pain, range of motions and disability of shoulder in acute stage of frozen shoulder. Methodology: This clinical trial includes 43 subjects in the acute stage of frozen shoulder with SPADI score > 30. Group 1 (n=22) received treatment including moist heat application and shoulder stretching exercises whereas group 2 (n=21) received end range mobilisation with interferential current therapy. Follow up was taken at 6th day of treatment using SPADI, ROM and VAS for pain. Results: Between Group comparison showed no statistically significant improvement (p=0.41) on VAS Score. However, Abduction (p=0.006), Flexion (p=0.03), and Internal Rotation (p=0.03) were statistically and clinically significant in group 2. Improvement was not observed for external rotation (p=0.8) and SPADI scale (p=0.57). Conclusion: The results demonstrated that the end range mobilization can be used for better improvement in ROM in acute stage of frozen shoulder. Both the treatment strategies can be equally useful for pain management.
Keywords: Frozen shoulder, Rehabilitation, Mobilisation, End range stretch, IFT, Moist heat.
Full Text:
INTRODUCTION
Among different causes of musculoskeletal conditions, Shoulder pain is the third most commonly experienced condition exceeded only by low back and neck pain. 1-3 Shoulder pain is associated with significant impairment and disability which leads to the loss of mobility of this joint and significant morbidity.4,5 A number of causes for shoulder pain exist. Among them, frozen shoulder is the significant one with incidence of 2% in general population in India.6-8 Clinically, it progresses through four phases, acute-painful phase, freezing phase, frozen phase and thawing phase.9,10 The duration of acute phase comprises from 0 to 3 months along with pain and stiffness in more than two directions.9 Treatment of frozen shoulder in this stage can prevent the further progression to more disabling stage.10 The management with respect to physiotherapy consists of various methods to addresses pain and stiffness. For pain the different strategies used are heat11 or ice applications12, ultrasound13, interferential therapy14,15, transcutaneous electrical nerve stimulation16, and pulsed electromagnetic field therapy5 .To correct the stiffness active and passive range of motion exercises17, mobilization and manipulation techniques18-23 are used A recent systematic review concluded that interferential therapy is beneficial in reducing pain in musculoskeletal condition when used as an adjunct to other treatments.14Moist heat has been proven beneficial in the treatment of shoulder impingement and frozen shoulder.11,12 Studies regarding early implication of stretching exercises showed significant improvement in patients’ functional status.17,22Studies comparing the effects of various joint mobilization techniques for frozen shoulder suggested that end range mobilization and movement with mobilization are better for improving pain and function.18-23Thus modalities such as interferential therapy and manual therapy have been shown to be effective when used as an adjunct, the efficacy of other modalities has not been proven. Few studies on combination of modalities or comparison of combined treatments showed beneficial short-term effects.11, 16, 18,24Thus, there is a need to evaluate the effectiveness of combined treatments in better implications for clinical practice. There is a lack of randomized trials for strong evidence of treatment because of heterogeneity in inclusion criteria; inadequate treatment follow-up and variable methodology for specific clinical conditions like frozen shoulder. Therefore, there is a need recommended by Cochrane review to evaluate effectiveness of physiotherapy modalities used in combination. Hence, the aim of the study was to compare the efficacy of end range mobilization (ERM) and interferential current therapy (IFT) with moist heat and stretching on pain, range of motion and disability of shoulder in the acute stage of frozen shoulder.
MATERIAL AND METHODOLOGY
This study was a randomized clinical trial to compare efficacy of two different physiotherapy intervention strategies for frozen shoulder. The study was conducted at the Physiotherapy department, in a Tertiary care hospital. Total duration of the study was of nine months and each subject was treated for 6 daily sessions. The inclusion criteria was subjects between 40 to 65 years of age , with insidious onset of symptoms between last one to three months, significant night pain, significant limitations of shoulder motion in more than one plane with end ranges painful.9 and SPADI scores ≥30 points.25,26 Subjects who had pain due to acute severe trauma such as fractures, dislocation; cervical radiculopathy; subjects suffering from myocardial infarction, hyper and hypothyroidism; and subjects with hypermobility and instability were excluded.23 The study protocol was approved by the Scientific Committee and Time Bound Research Ethics Committee of the KMC, Manipal University. Subjects who were diagnosed for frozen shoulder referred by consultant to the physiotherapy were taken for the study. The total numbers of subject assessed were 59. Among them who fulfilled the inclusion criteria were taken for the study (N=43).The purpose of the study was explained to the subjects and an informed consent was obtained. The demographic information of the included subjects was taken. During the initial evaluation session, the patient was interviewed and an upper quarter screening examination was conducted to rule out cervical and elbow pathology. The baseline data of ROM with goniometer, VAS for pain and SPADI (shoulder pain and disability index) were taken by an observer who was blinded to the study. The same observer recorded the outcome measure after the completion of treatment session. After that, they were randomized into 2 groups, with block randomization.
In-Group 1, the intervention was given as follow.
1) Moist heat
Moist pack was wrapped in towel with three to four folds over the affected shoulder for 10 to 15 minutes. [Moist Heat Therapy Unit –MNE, India]
2) Stretching exercises
Shoulder stretching exercises include; Forward flexion, External rotation, Horizontal adduction, internal rotation.
In-Group 2, the intervention was given as follows,
1) End range Mobilization.-
At the start of each intervention session, the physical therapist examined the patient’s ROM in all directions to obtain information about the end-range position and the end-feel of the glenohumeral joint. Then, 10- 15 repetitions of intensive mobilization were given for flexion, abduction, internal rotation and external rotation Figures 1 and 2).18, 19
2) Interferential therapy
Interferential current therapy was given. [Current applied at 4000 Hz carrier frequency, Amplitude Modulated Frequency will be 0 to 250 Hz. Treatment time was 10 to 15 minutes].27 Patients were re-examined after 6 days of treatment for evaluation of outcomes, i.e. ROM, SPADI and VAS for pain.
 '
'

RESULTS
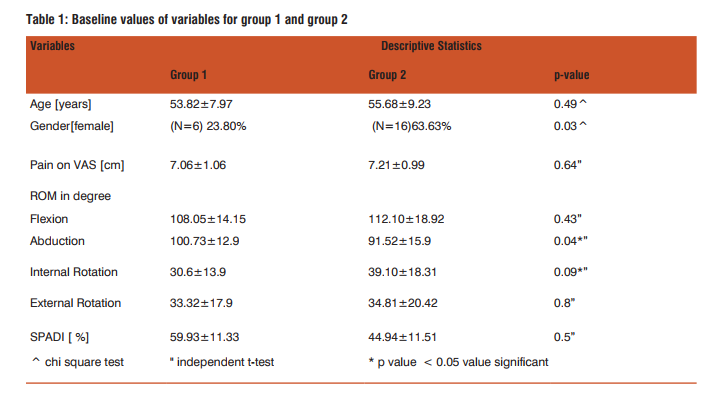
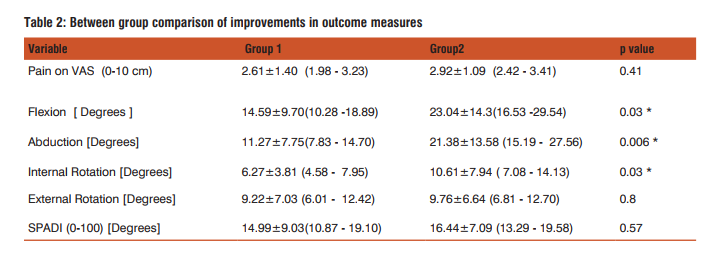
Table1 shows baseline value of variables in both the groups. Both the groups had similar baseline values of characteristics for pain and disability and no significant difference was seen between groups. Table 2 shows the comparison of improvements in outcome measures between group 1 and group 2.Pain on visual analogue scale was not statistically significant (p=0.41) between the two groups. Both the group showed similar improvement on VAS. There were significant changes seen in ROMs between the groups. Abduction was statistically highly significant (p=0.006), while flexion (p=0.03) and internal rotation (p=0.03) range were also significant for group 2. However no statistically significant difference was seen in external rotation (p=0.8) between the groups. There was also no significant difference in SPADI scale between groups (p=0.57), which indicates improvement in disability was similar for both the groups.
DISCUSSION
Present study compared two different treatment strategies in patients with acute stage of frozen shoulder. The result of the study was in agreement with hypothesis that combination of End range mobilization and IFT will produce better improvement. The reasons could be attributable to: end-range mobilization and its specific mechanical effects on connective tissue which might have increased ROM.22 This difference in therapeutic responses measured through changes of joint mobility compared to pain and disability were noted previously in other studies.15-18
Range of Motion
The between-group mean difference for ROM of flexion (group 1-14.59, group 2-23.04), and abduction (group1- 11.27, group 2-21.38) was greater than the MCID reported 7 degree for flexion and 16 degree for abduction. The between –group mean difference for ROM for internal rotation (group1-6.27.group2-10.61) and external rotation (group 1- 9.22, group 2- 9.76) was lesser than the MCID reported 11 degree for internal rotation and 14 degree for external rotation.28 The possible mechanism for increase in ROM as suggested by Kelley M et al9 that, specific joint mobilization techniques are believed to selectively stress certain parts of the joint capsule. Yang et al22 said that, this mobilization performed in specific plane close to end range improve the extensibility of periarticular structure. However, the results of the previous studies 18, 19, 29 also showed significant improvement in shoulder external range of motion, which was not statistically significant in the present study. The probable reason of this could be capsular pattern of shoulder joint described by Cyrix in which external rotation was the most limited and hence, difficult to treat and in order to improve external rotation of shoulder long time treatment protocol is mandatory. In-group 1with conventional therapy, the stretching exercises prescribed also did not address specific to rotator cuff interval. Therefore, in both the groups it was lacking .Few studies with follow-up of 12 and 15 years in frozen shoulder patients showed deficiency in external rotation range even after successful treatment.30,31 So, this is in agreement that it is difficult to gain improvement in external rotation in a short period of time.
Pain on VAS score: The MCID value of VAS score is 3 mm.5 In the present study, group 1 showed mean improvement of 2.61mm and group 2 showed 2.92mm. Therefore, none of group has reached at MCID, which give inferences that either IFT or moist heat can be used for pain relief.
SPADI score In the present study, we have used shoulder Pain and Disability Questionnaire in order to document the level of disability with frozen shoulder patient. This scale has been used in previous studies with various shoulder pathology.32, 33 The improvement noted in-group 1 was (14.99±9.03) and group 2 was (16.44±7.09) which was greater than the MCID of this scale. Here, both the group showed similar improvement. Tvieta et al26 had reported the responsiveness of SPADI scale in-patient with frozen shoulder. Point estimates (1.45) for between group changes in disability not exceeded the reported MCIDs. In addition, using MCID of 13 point for SPADI scale, NNT was calculated. The NNT (Number needed to treat) is 5. This means that 5 patients are required in order to say our intervention is effective.
CONCLUSION
The results of present study demonstrated that patients treated with end range mobilization showed greater improvement in range of motion when compared with the group treated with moist heat and stretching exercises. Improvement in pain severity and disability was similar with both the treatments. Therefore, end range mobilization can be used for better improvement in range of motion particularly in acute stage of frozen shoulder. Both the treatment strategies were equally effective for pain management.
ACKNOWLEDGEMENTS
The authors thank Dr Vivek Ramanandi for support in making manuscript. Special gratefulness are extended to Dr P. Senthil Kumar (PT) and Dr Prem Kotian (MS, Ortho) for their support and guidance throughout this study. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors /publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Bhargav D, Murrell G A. Stiffness of shoulder: diagnosis. Aust Fam Physician. 2004; 33:143-47.
2. Green S, Buchbinder R, Hetrick SE. Physiotherapy interventions for shoulder pain. Cochrane Database of Syst Rev. 2003;2:CD004258.
3. Evidence based management of acute musculoskeletal pain. 2003.p.119-130.
4. Manske RC, Prohaska D. Diagnosis and management of adhesive capsulitis. Curr Rev Musculoskeletal Med. 2008;1:180-9.
5. Thompson J, O’Brien T, Richardson C, Davison D, Watson H, Wragg M et al. (2011) Evidence-based clinical guidelines for the diagnosis, assessment and physiotherapy management of contracted (frozen) shoulder v.1.2, ‘standard’ physiotherapy. Endorsed by the Chartered Society of Physiotherapy.
6. Gupta S, Raja K, Manikanandan N. Impact of adhesive capsulitis on quality of life in elderly with diabetic. Int J Diabetes Dev Ctries. 2008;28:125-9.
7. Mathew AJ, Nair JB, PillaiS. Rheumatic musculoskeletal manifestation in type 2 diabetes mellitus patients in south India.Int J Rheum Dis. 2011;14:55-60.
8. Page P, Labbe A. Adhesive capsulitis: use the evidence to integrate your interventions. N Am J Sports Phys Ther. 2010;5:266- 73.
9. Kelley MJ, Mcclure PW, Leggin BG. Frozen shoulder: evidence and a proposed model guiding rehabilitation. J Orhtop Sports Phys Ther. 2009;39:135-48.
10. Donatelli R A. Physical therapy of the shoulder. 5thed. Elsevier; 2011.p.231-44.
11. Leung MS, Cheing GL. Effect of deep and superficial heating in the management of frozen shoulder. J Rehabil Med. 2008;40:145-50.
12. Calis HT, Berberoglu N, Calis M. Are ultrasound, laser and exercise superior to each other in the treatment of shoulder impingement syndrome? A randomized clinical trial. Eur J PhysRehabil Med. 2011;47:375-80.
13. Kurtais Y, Ulus Y, Bilgic A, Dincer G, Heijden VD. Adding ultrasound in the management of soft tissue disorders of the shoulder: a randomized placebo-controlled trial. Phys Ther. 2004;84:336- 43.
14. Fuentes J, Olivo S, Magee DJ, Gross D. Effectiveness of interferential current therapy in the management of musculoskeletal pain: systematic review and meta-analysis. Phys Ther. 2010;9:1219-38.
15. Cheing G L,So EM, Chao CY. Effectiveness of electroacupuncure and interferential electrotherapy in the management of frozen shoulder. J Rehabil Med. 2008;40:166-70.
16. Uysal F G, Kozanoglu E. Comparison of the early response to two methods of rehabilitation in adhesive capsulitis. Swiss Med Wkly. 2004;134:353-8.
17. Celik D. Comparisons of the outcomes of two different exercise programs on frozen shoulder. Acta Orthop TraumatolTurc. 2010;44:285-292.
18. Yang J, Chang C, Chen S, Wang S, Jenq J. Mobilization techniques in subjects with frozen shoulder syndrome: randomized multiple-treatment trial. PhysTher. 2007;87:1307-15.
19. Vermeulen HM, Obermann WR, Burger BJ, Kok GJ, Rozing PM, Ende CH. End-range mobilization techniques in adhesive capsulitis of the shoulder joint: a multiple-subject case report. PhysTher. 2000;80:1204-13.
20. Yang J L, Jan M H, Chang C W, Lin J J. Effectiveness of the end range mobilization and scapular mobilization approach in a subgroup of subjects with frozen shoulder syndrome: a randomizedcontrol trial. Man ther. 2012;17: 47-52.
21. Vermeulen HM, Rozing PM, Obermann WR, Cessie SL, Vlieland TP. Comparison of high grade and low grade mobilization techniques in the management of adhesive capsulitis of the shoulder: randomized controlled trial. PhysTher. 2006;86:355- 68.
22. Brudvig TJ, Kulkarni H, Shah S. The effect of the therapeutic exercises and mobilization on patients with shoulder dysfunction: A systematic review with meta-analysis. J orthop sport physther. 2011;41:734-48.
23. Chen JF, Ginn KA, Herbert RD. Passive mobilization of shoulder region joints plus advice and exercise does not reduce pain and disability more than advice and exercise alone: a randomized trial. Aust J Physiother. 2009;55:17-23.
24. .Jurgel J, Rannama L, Helena G, Ereline J, Kolts I, Paasuke M. Shoulder function in patients with frozen shoulder before and after 4-week rehabilitation. Medicina 2005;41:30-6.
25. Carette S, Helene M, Tardif J, Bessette L, Morin F, Fremont P et al. Intra articular corticosteroids, supervised physiotherapy, or a combination of the two in the treatment of adhesive capsulitis of the shoulder. Arthritis Rheum. 2003;48:829-38.
26. Tveita E K, Ekeberg O M, Juel N G, Holter E B. Responsiveness of the Shoulder Pain and Disability Index in patients with adhesive capsulitis. BMC Musculoskeletal Disord. 2008;9:161-65.
27. Kitchen S. Electrotherapy- Evidence based Practiced 11thedition. Melbourne. Harcourt Publishers Ltd; 2002.p.297-309.
28. Muir SW, Corea CL, Beaupre L. Evaluating changes in clinical status: reliability and measures of agreement for the assessment of glenohumeral range of motion.2010;5:98-111.
29. Johnson AJ, Godges JJ, Zimmerman GJ, Ounanian LL. The effect of anterior versus posterior glide joint mobilization on external rotation range of motion in patients with shoulder adhesive capsulitis. J Orthop Sports PhysTher. 2007;37:88-99.
30. Farrell C M, Sperling J W, Cofield R H. Manipulation for frozen shoulder: long- term results. J shoulder Elbow Surg. 2005;14:480-484.
31. Shaffer B, Tibone J E, Kerlan R K. Frozen shoulder: A long-term follow-up. J Bone Joint Surg Am. 1992;74:738-46.
32. Bennell K, Wee E, Coburn S, Green S, Staples M, Forbes A et al. Efficacy of standardized manual therapy and home exercise programme for chronic rotator cuff disease: randomized placebo controlled trial. BMJ. 2010;340:2756-65.
33. Dogan SK, Ay S, Evcik D. The effectiveness of low laser therapy in subacromial impingement syndrome: a randomized placebo controlled double-blind prospective study. Clinics.2010;65:1019-22.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





