IJCRR - 9(8), April, 2017
Pages: 21-29
Date of Publication: 01-May-2017
Print Article
Download XML Download PDF
Anatomical Study of the Ankle Joint in Relation to the Anterior, the Posterior and the (New) Medial Arthroscopic Portals: A Cadaveric Study
Author: Bharambe Vaishaly K., Shinde Amol A., Patel Dinesh K., Chaudhary Sumedha
Category: Healthcare
Abstract:Context: Several arthroscopic portals are used for arthroscopy for which understanding of anatomy of ankle and foot is very important. Aims: To study the anatomy of ankle joint in relation to the anterior, posterior and medial midline arthroscopic portals by dissection method. Methods and Material: The distance of the portals to the corresponding neurovascular structures was measured in 20 cadavers using a vernier caliper. Results: The mean distance between the anteromedial portal and the great saphenous vein and saphenous nerve was found to be 7.7 mm, that between the medial midline portal and the dorsalis pedis artery and deep peroneal nerve was found to be 1.7 mm. The mean distance between the anterocentral portal and the dorsalis pedis artery and deep peroneal nerve was found to be 1.4 mm, and that between the anterolateral portal and superficial peroneal nerve was found to be 2.5 mm. Absence of peroneus tertius was found in 2 out of 20 cases. The mean distance between posterolateral portal and sural nerve was found to be 15.9 mm.
Conclusions: The present study confirmed that use of anteromedial portal for ankle arthroscopy is comparatively safe while indicating high chances of injury to dorsalis pedis artery and deep peroneal nerve in both anterocentral and middle midline portals. In case of anterolateral portal the study found the mean distance to be 2.5mm but variations in distribution of superficial peroneal nerve and in tendons of this region have to be studied beforehand to avoid injury to the nerve.
Keywords: Ankle arthroscopy, Anteromedial portal, Anterolateral portal, Posteromedial portal, Posterolateral portal, Medial midline portal
Full Text:
Introduction
Symptoms and complaints related to ankle joint are very commonly encountered by orthopedicians. For this, ankle arthroscopy is a common, less invasive and valuable procedure for diagnosis and treatment of any ankle injuries.[1] It is generally performed as outpatient surgery. This is done either under general or regional anesthesia or under epidural anesthesia with the patient sedated. The space within the ankle joint can be temporarily enlarged, and the space can be observed using instruments and a special camera. For entry of the camera and related instruments, incisions are made in the ankle. These are referred to as portals i.e. they act as portals for entry of machine or instrument into the ankle joint. Through the camera, ankle arthroscopy helps in direct visualization of inside of ankle without large cosmetically unsightly scars. At the end of the procedure the incisions are closed by putting tiny sutures on the skin to close the portals and covered by a sterile dressing. Often patient can go home on the same day. [2]
Today arthroscopy is used not only as a tool for investigation, but also as an alternative to open ankle surgery. It has become popular surgical approach for addressing many ankle pathologies that are intra-articular. It is used for treatment of conditions like synovitis, osteochondral defect of talus (osteochondritis dessicans), arthrofibrosis, infection, tibiotalar arthritis, loose bodies, impingement, intra-articular fractures and osteochondral lesions. Patients may be able to begin rehabilitation sooner, and return to high level activities like sports.[3]
Several arthroscopic portals are utilized during ankle arthroscopy, like anteromedial and anterolateral which are most commonly used and allow access to all sides of the joint. [4] The anterocentral portal helps us to see both sides of the joint but is less used because of associated risk to dorsalis pedis artery and related nerve. Other portals are posteromedial, posterolateral, medial transmalleolar and through the Achilles tendon. New portal for ankle arthroscopy has been described called medial midline portal which approaches ankle joint through space between extensor hallucis longus and tibialis anterior.[4]
Variations are seen in terms of distances of portals to the neurovascular structures around the ankle joint. A variety of these neurovascular structures may be encountered during ankle arthroscopy through any of above portals and could be damaged. Same structures can also be damaged during open surgeries of the ankle, but chances of injuring them during mini open approaches or ankle arthroscopy are higher as in open surgery neurovascular structures are better visualized and thus iatrogenic injuries can be avoided.[5]
It is mandatory to have a thorough understanding about the anatomy of the ankle and foot to perform ankle arthroscopy. It becomes important to study the structures in vicinity of the above portals and to note any associated variations. Knowledge of such variations is important as these variant nerves and/ or blood vessels can be injured during the arthroscopic procedures and/or regional anaesthesia. It can explain some unusual clinical symptoms caused due to variations.[6]
The purpose of present study is to discuss the portals used for ankle arthroscopy and to discuss their surgically relevant anatomy and related variations.
Ferkel has described that ankle and foot injuries are frequent today. They are usually diagnosed clinically or using imaging techniques. But some are difficult to evaluate by these methods. Such cases are a diagnostic challenge. He says that though bony disorders are easy to diagnose radiologically, injuries to articular cartilages are best diagnosed arthroscopically. Thus arthroscopy has become very popular as a means to diagnose and treat various ankle disorders. Ferkel also described that arthroscopy can be done under general, spinal, epidural or local anaesthesia using an arthroscope with a diameter of 2.7 to 4 mm. He says that 3 portals have been established to routinely examine the ankle joint cavity. They provide complete access to the joint and also adequate flexibility of approach during examination and surgery. These are the anterolateral, anteromedial and posterolateral portals. He stressed that the placement of portals must be based on thorough knowledge of extra-articular anatomy of the ankle joint to avoid injury to the neurovascular structures as well as tendons around the ankle. He recommended two anterior portals, namely anteromedial and anterolateral, anteromedial being just medial to the tibialis anterior tendon and anterolateral being just lateral to the peroneus tertius tendon. He stated that posterior portals, also used for arthroscopy were posterolateral and posteromedial portals, lying lateral and medial to Achilles tendon respectively. The posteromedial portal is used popularly but should be used with great caution.[7]
Golano et al in their article for arthroscopists stress on the need for adequate knowledge of the anatomy of ankle joint, intra as well as extra articular, along with anatomic variations to avoid confusion and intraprocedure complications. They state that in arthroscopy a three dimensional picture of interior of ankle joint as seen by surgeon or anatomist by opening the ankle joint has been converted into a two dimensional picture seen through the arthroscope. The authors state that most important aspect of preventing injury to structures related to ankle joint is to make skin incisions parallel to the tendons and neurovascular structures running from leg distally to the foot and that it is necessary to carry out blunt dissection to prevent injury while reaching the joint capsule. Golano et al stressed on the necessity to identify tendons such as tibialis anterior, peroneus tertius and that of tendocalcaneus or Achilles tendon and neurovascular structures such as saphenous vein and superficial cutaneus nerve and its two branches i.e. medial and intermedial cutaneus nerves which can be easily identified in thin patients.[8]
Golano et al stated that in case of anteromedial portal which is made just medial to the tibialis anterior tendon there is a potential to damage the great saphenous vein as well as the saphenous nerve. In case of anterolateral portal, the structure likely to be damaged is the intermediate dorsal cutaneous nerve which is the lateral branch of superficial peroneal nerve. They also stated that it is essential for the arthroscopist to remember that the superficial peroneal nerve and its branches lie close to anterolateral portal and injury to them needs to be avoided. However he emphasized that since the nerve is subcutaneous and visible on clinical examination, injury to it can be avoided by careful inspection of the lateral ankle region after inversion of the foot. In case of anterocentral portal, there is potential to injury to the deep peroneal nerve and to dorsalis pedis artery. Due to these possibilities the use of anterocentral portal is discouraged. While discussing the posterior portals, Golano et al stated that the posterolateral portal is more popularly used compared to medial. It lies 1.2 to 2.5 cm proximal to the lateral malleolus and is in close proximity to the sural nerve and the short saphenous vein. The posteromedial portal has potential to damage the tibial nerve, posterior tibial artery and tendons of flexor hallucis and flexor digitorum longus muscles.[8]
Buckingham et al introduced the medial midline portal wherein the ankle joint was approached through a portal just lateral to the tibialis anterior tendon. This portal was said to have a lesser risk of injury to neurovascular structures of this region.[4]
Woo et al carried out a study wherein they investigated the anatomic variations of neurovascular structures in the ankle in relation to safety margins for arthroscopic portals. They studied 23 ankles by dissection method after marking the various portals namely anterolateral, anteromedial, posterolateral and posteromedial and measured the distances of each portal with related neurovascular structures. They found significant variations in the neurovascular structures and concluded that care must be taken to avoid inadvertent injury to the neurovascular structures during ankle arthroscopy.[9]
Sitler et al studied the safety of posterior portals by marking them and then studying their MRI images. The proximity of these portals to adjacent structures were measured on the images and also by dissection and these 2 distances were compared. They concluded that with patient in prone position, arthroscopy can be done using posterior portals without gross injury to the posterior neurovascular structures. The measurements of MRI images were used as additional measurements to confirm the dissection results. No significant differences were detected.[10]
Balci et al in a similar study involving the posterior ankle arthroscopic portals, studied the distance of important neurovascular structures from either of the posterior portals in different ankle positions namely neutral, plantar flexed and dorsiflexed. They concluded that the distance between the neurovascular structures and the portals was more in plantarflexed and dorsiflexed positions compared to that in neutral position.[11]
Scholten and C Niek van Dijk have described a anterior and posterior arthroscopy wherein first patient was in supine position for anterior approach and then in prone position for posterior approach through the portals.[12]
Zengerink M and C Niek van Dijk in a retrospective study involving 1305 patients who had undergone ankle arthroscopy, found the complication rate to be 3.5%. 1.9% were neurological problems and were found to be due to due to errors during placement of the portal.[13]
Materials
Materials used were:
Gloves, scalpel, blunt and tooth forceps, fine small scissors, 23 guage needle, vernier caliper and a 12 megapixel camera for photography.
Methods
Institutional Ethical Committee clearance was obtained before study was commenced. (Attached)
30 lower limbs were obtained from formalin fixed cadavers. Each limb was examined, rejecting five which were damaged. Once selected, each limb was labeled separately for identification.
The surface landmarks such as medial and lateral malleoli, borders of Achilles tendon and medial border of tibialis anterior muscle were identified. The different portals were marked using a 23 guage needle as follows:
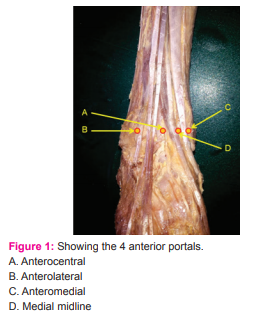
With the limb in supine position (Figure 1 depicts the positions of the 4 anterior portals):
- Medial to the tibialis anterior tendon and parallel to the joint line we marked the anteromedial portal.
- Lateral to the peroneus tertius tendon and parallel to the joint line we marked anterolateral portal.
- Between tibialis anterior and extensor hallucis longus we marked the medial midline portal
- Lateral to the extensor hallucis longus tendon we marked the anterocentral portal.
With the limb in the prone position
- The posterolateral portal was marked just lateral to the Achilles tendon and about half inch proximal to the distal tip of lateral malleolus
- The posteromedial portal, just medial to the Achilles tendon and 1.2 cm proximal to a horizontal line drawn from the tip of lateral malleolus.
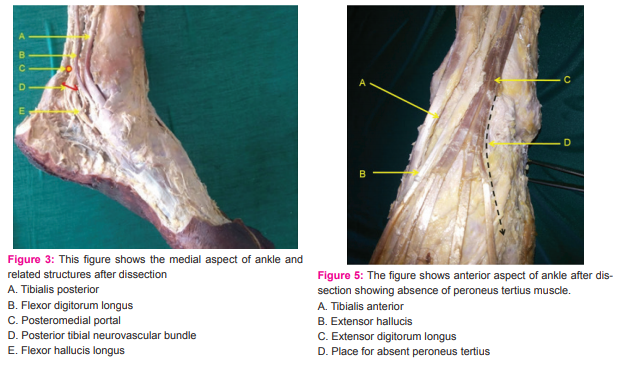
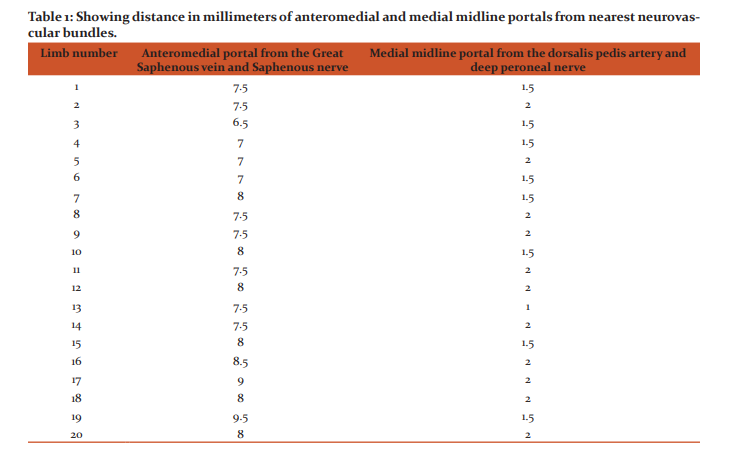
After the portals were marked the dissection was commenced. However the needles inserted were removed during dissection as they interfered with the finer dissection. The skin and subcutaneous fat was dissected from underlying fascia for visualization of the neurovascular structures below. Throughout the dissection care was taken not to disturb the dissected tendons, nerves or blood vessels. The distance of the portals to the corresponding neurovascular structures was measured using a vernier caliper. For each individual portal, care was specially taken for important structures. For the anteromedial portal, the great saphenous vein and saphenous nerve were dissected with care and their distance from the portal was measured. For the anterolateral portal the superficial peroneal nerve and its branches were dissected.
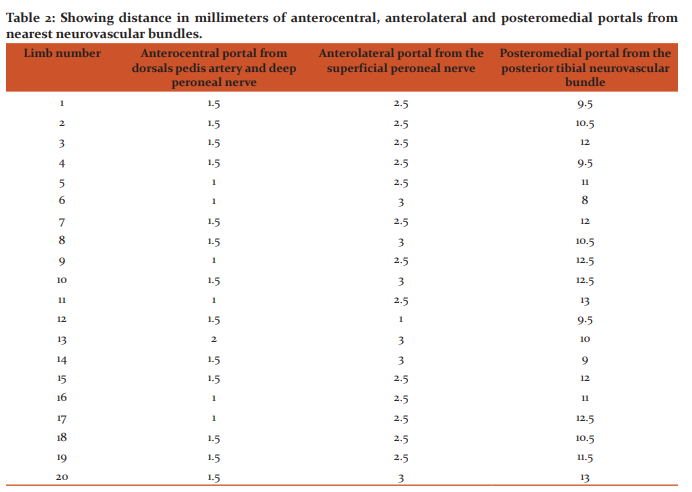
Any variation in branching mentioned. Distance between these nerves and the portal was noted. The area round the anterocentral portal was dissected carefully to note the dorsali pedis artery, deep peroneal nerve and its branches and distance between these and the portal was noted. The medial midline portal and its distance from deep peroneal nerve and dorsalis pedis artery was measured (Figure 2). Similarly the distance between the sural nerve and the posterolateral portal and between the posterior tibial neurovascular bundle and the posteromedial portal was measured taking care to note any variations in branching pattern of the nerves and vessels. All measurements were taken in millimeters. (Figures 3,4)
Observations and Results
The data presented here is for a total of 20 lower limbs. Five lower limbs were not suitable as parts of them were damaged and the other 5 lower limbs could not be dissected due to constraints of time. The distance between the anteromedial portal and the great saphenous vein and saphenous nerve is depicted in Table 1. The mean distance between the anteromedial portal and the great saphenous vein and saphenous nerve was found to be 7.7 mm, range being 6.5 to 9.5mm. The distance between the medial midline portal and the dorsalis pedis artery and deep peroneal nerve is depicted in Table 1. The mean distance between the medial midline portal and the dorsalis pedis artery and deep peroneal nerve was found to be 1.7 mm, range being 1 to 2 mm. The distance between the anterocentral portal and the dorsalis pedis artery and deep peroneal nerve is depicted in Table 2. The mean distance between the anterocentral portal and the dorsalis pedis artery and deep peroneal nerve was found to be 1.4 mm, range being 1 to 2 mm.
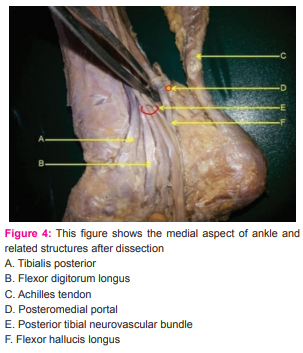
The distance between the anterolateral portal and the superficial peroneal nerve is depicted in Table 2. The mean distance between the anterolateral portal and superficial peroneal nerve was found to be 2.5 mm, range being 1 to 3 mm. Absence of peroneus tertius was found in 2 out of 20 cases i.e. an 10% incidence. (Figure 5) The distance between posteromedial portal and posterior tibial neurovascular bundle is depicted in Table 2. The mean distance between them was found to be 11 mm and the range found to be 8-13 mm. The distance between posterolateral portal and sural nerve was measured in 6 cases as in other cases the sural nerve was damaged during removal of skin. The mean distance between them was found to be 15.9 mm and the range found to be 9.5-19.5 mm.
During the measurement of all above distances wide variations were found in the distances measured between the portals and related neurovascular structures in cases of the posteromedial and posterolateral portals.
DISCUSSION

 \
\
Arthroscopy is increasingly being used for diagnosis and treatment of ankle related pathologies. The ankle arthroscopy is thus used for survey of ankle joint from within and for reparative ankle surgery. [14] Ankle arthroscopy was the first attempted in 1931 and fol lowing the attempt it was concluded that this joint was not suitable for arthroscopy due to its narrow joint cavity. Since then narrow small diameter arthroscopes have resulted in improved ability to perform diagnostic and operative arthroscopy. [14] However there are some possible complications with arthroscopy. To prevent them the surgeon must be well versed with anatomy of the ankle region. Ferkel described an complication rate of about 9%. 49% of these were neurological. The most commonly injured nerve was the superficial branch of common peroneal nerve. Lesser complications were due to injury to sural, deep peroneal and saphenous nerves. Ferkel also reported complications with anterocentral and posteromedial portals. It was concluded that thorough understanding of the extra-articular anatomy of the ankle region was mandatory to avoid complications. [7]. The present study was aimed at studying this extra-articular anatomy of the ankle region with respect to the anterior (anteromedial, anterocentral and anterolateral), posterior (posteromedial and posterolateral) and medial midline portals. The distances between each of the respective portals and the commonly injured neurovascular bundles near them was measured.
The Anteromedial portal
In the present study the mean distance between the anteromedial portal and the great saphenous vein and saphenous nerve was found to be 7.7 mm, range being 6.5 to 9.5mm.
Stetson and Ferkel state that the anteromedial portal is made first as it is easy to establish and the region where it is placed is devoid of any major neurological structures.[6] Woo et al reported the mean distance to be 10.2mm (range 1.1 to 20.2) in a study carried out on Chinese cadavers, which is more than the finding reported by present study. [9] Golano et al while describing ankle anatomy for the arthroscopists, report the mean safe distance between the portal and the great saphenous vein as 9mm (range 3-16mm) and for saphenous nerve as 7.4mm (range 0-17mm).[8] Though these structures are relatively risk-free, there are reports of a case of lesion of the great saphenous vein and 5 cases neurological complications during arthroscopy using the anteromedial portal. [7,15] The mean distance reported by present study is lesser than findings of all above authors and this could indicate higher possibility of damage to both great saphenous vein and saphenous nerve during use of anteromedial portal for arthroscopy in case of Indian population.
The medial midline portal
This portal was described by Buckingham et al as a new portal for ankle arthroscopy. [4] Here the arthroscope passes between the tendons of extensor hallucis longus and tibialis anterior. The authors reported a mean distance of 11 mm (range 5-15mm) from the dorsalis pedis artery. In the present study a mean distance between the medial midline portal and the dorsalis pedis artery and deep peroneal nerve was found to be 1.7 mm, range being 1 to 2 mm. This distance reported by present study is very much less compared to findings reported by Buckingham et al. Golano et al state that this portal gives an intra-aricular view similar to that by anterocentral portal but with lower chances of lesion to vital structures.[8]
The anterocentral portal
In the present study the mean distance between the anterocentral portal and the dorsalis pedis artery and deep peroneal nerve was found to be 1.4 mm, range being 1 to 2 mm. Buckingham et al reported the mean distance to be 0.7 (range 0-5) in case of dorsalis pedis artery and 1.1 (range 0-5) in case of deep peroneal nerve. The authors state that in 90% of the cases where this portal was used, the arthroscope touched the dorsalis pedis artery and in one case it lacerated the deep peroneal nerve. In all cases the arthroscope was in contact with the superficial peroneal nerve and in 3 cases this nerve too showed lacerations.[4] Feiwell and Frey found the average distance of this portal from the neurovascular bundle to be 3.3mm (range, 0-10mm).[16] In 1 case the arthroscope penetrated and in 4 cases was related to the neurovascular bundle. Golano et al state that use of this portal is discouraged due to high associated risk of injury to superficial peroneal nerve superficially and deep peroneal nerve and dorsalis pedis artery on the deeper plane.[8] The present study reports the distance of portal from close neurovascular structures to be 1.4 mm which is close to that reported by Buckingham (0.7 mm) but less than the 3.3 mm distance reported by Feiwell and Frey. Golano et al state that any associated variations of the artery may also lead to vascular lesions. [8] Basarir et al studied the lateral and medial malleolar arteries and their distances from the arthroscopic portals in plantar and dorsiflexion positions of foot. The authors go on to state that risk of vascular injury is quiet high in case of arthroscopy and advised position of plantar flexion during portal placement which increases the distance of the portal from the blood vessels.[17]
The anterolateral portal
In the present study the mean distance between the anterolateral portal and superficial peroneal nerve was found to be 2.5 mm, range being 1 to 3 mm. Buckingham et al reported a mean distance of 0.5 mm (range, 0-10 mm). They reported 2 cases of laceration to the nerve during arthroscopy using this portal. [4] Stetson and Ferkel state that this portal is made just lateral to the peroneus tertius tendon at the joint level.[6] The superficial peroneal nerve branches are at risk. [14] They report a mean distance of the portal from the superficial peroneal nerve branch to be 6.2 mm (range, 0-24mm). Woo et al found the mean distance between the portal and superficial peroneal nerve to be 5.5mm (range, 0.4 to 14.4). They state that the anterolateral portal should be placed as close to the fibulas as possible to avoid injury to the nerve. [9]The mean distance reported by present study is greater than that reported by Buckingham et al but less than that reported by Stetson and Ferkel and Woo et al. The present study reports absence of peroneus tertius muscle in 2 limbs. This could mislead the surgeon while placing the portal. Such absent peroneus tertius muscle was also reported by Das et al, though the study did not correlate the absence of the muscle with relation to the anterolateral arthroscopic portal. [18] C Niek van Dijk clearly states that in absence of peroneus tertius (which is present in 90%of the population), the anterolateral portal is placed adjacent to extensor digitorum longus tendon.[19]
The posteromedial portal
In the present study the mean distance between posteromedial portal and the posterior tibial neurovascular bundle was found to be 11mm and the range found to be 8-13 mm. Balci et al reported the mean distance to be 6mm (range, 3.9 to 9.5mm).[11] Woo et al found the mean to be 14.2mm (range, 5.2 to 22.1mm).[9] The distance reported by present study of 11mm is greater than that reported by Balci et al and less than the findings of Woo et al in their study on Chinese cadavers.
Frank et al state that the posterior tibial artery could be damaged during creation of the posteromedial portal.[5] Ilyas et al stated that this portal was contraindicated due to proximity to posterior tibial artery and nerve and also risk to flexor hallucis and flexor digitorum longus tendons.[19] Sitler et al in a study of posterior ankle arthroscopy state that though arthroscopy has generally been performed with the use of anterior portals with the patient in supine position, the authors advise that with the patient in prone position, posterior ankle arthroscopy can be performed without gross injury to the posterior neurovascular structures.[10]
The posterolateral portal
The distance between posterolateral portal and sural nerve was measured in 6 cases in the present study. The mean distance between them was found to be 15.9 mm and the range found to be 9.5-19.5 mm. Woo et al report a mean distance of 12.6mm (range, 7.0 to 23.0) and Feiwell and Frey reported it to be 6mm (range, 0-12mm). [9,16] Balci et al reported it to be 6mm (range, 2.7 to 14.5mm).[11] The distance reported by present study is found to be the highest among all reported. However considering that only 6 cases could be dissected successfully to demonstrate the sural nerve, this mean of 15.9 mm cannot be reliably used for comparison. Both the posterior distances measured in present study were found to be higher than those reported by other authors. Regarding the posterior ankle arthroscopic portals, Zengerink M and C Niek van Dijk state that posterior ankle arthroscopy using a 2 portal approach is a safe procedure with the rate of complication similar to anterior ankle arthroscopies. [13]
CONCLUSION
The mean distance between the anteromedial portal and the great saphenous vein and saphenous nerve is 7.7 mm as reported by present study which is lesser than findings of all above authors and this could indicate higher possibility of damage to both these structures during use of anteromedial portal for arthroscopy in case of Indian population. In case of the medial midline portal which is a new portal for ankle arthroscopy, the mean distance of the portal from the dorsalis pedis artery was found to be 1.7 mm. This distance reported by present study is very much less compared to findings reported by other authors and does not give much space for maneuvering of the arthroscope and likelihood of damage to the dorsalis pedis artery seems to be very likely. In the present study the mean distance between the anterocentral portal and the dorsalis pedis artery and deep peroneal nerve was found to be 1.4 mm. This finding is similar to findings of most other authors and indicates high chances of injury to the dorsalis pedis artery and deep peroneal nerve in case this portal is used for arthroscopy.
In the present study the mean distance between the anterolateral portal and superficial peroneal nerve was found to be 2.5 mm. An associated absence of peroneus tertius was noted in 2 limbs. The mean distance reported by present study is greater than that reported by Buckingham et al but less than that reported by Stetson and Ferkel and Woo et al.[4,6,9] Careful observation of the branches of superficial peroneal nerve and examination and palpation of the limb involved to note all related tendons can reduce chances of damage to underlying structures in case of use of this portal as well as in portal placement. In the present study the mean distance between posteromedial portal and the posterior tibial neurovascular bundle was found to be 11mm. The distance reported by present study of 11mm is greater than that reported by other authors. The mean distance between posterolateral portal and sural nerve measured in 6 cases in the present study was found to be 15.9 mm and was the highest reported by any author. However considering that only 6 cases could be dissected successfully to demonstrate the sural nerve, this mean of 15.9 mm cannot be reliably used for comparison.
The present study measures the distances of 4 anterior portals and 2 posterior portals used for arthroscopy at the ankle joint, from the closest neurovascular bundles. The study confirmed that use of anteromedial portal for ankle arthroscopy is comparatively safe due to the distance existing between the portal and the great saphenous vein and saphenous nerve. The study also indicated high chances of injury to dorsalis pedis artery and deep peroneal nerve in both anterocentral and middle midline portal. In case of anterolateral portal the study found the mean distance to be 2.5mm but variations in distribution of superficial peroneal nerve and in tendons of this region have to be studied beforehand to avoid injury to the nerve or wrongful placement of the portal. In case of the posterior portals, the mean distances measured for both medial and lateral portals were found to be more than the mean distances reported by other authors. In present study 20 limbs were dissected for 5 of the portals. For the posterolateral portal the sural nerve was dissected successfully in only 6 limbs and was damaged during dissection in others. Further study using more number of limbs would help bring more authenticity to the data and may also reveal further details of some of the variations encountered.
ACKNOWLEDGEMENT
The Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to the authors/editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of funding: As this study was carried out in the dissection hall of our Department, there was no separate financial aid provided for it. Conflict of interest: There is no conflict of interest
References:
1. Andrews JR, Previte WJ, Carson WG. Arthroscopy of the ankle: technique and normal anatomy. Foot Ankle 1985;6:29-33.
2. Amendola A, Petrik J, Webster-Bogaert S. Ankle arthroscopy: outcome in 79 consecutive patients. Arthroscopy. 1996 Oct;12(5):565-73.
3. Calder JD, Sexton SA, Pearce CJ. Return to Training and Playing After Posterior Ankle Arthroscopy for Posterior Impingement in Elite Professional Soccer. Am J Sports Med,38(1):120-4
4. Buckingham RA, Winson IG, Kelly AJ. An Anatomical Study Of a New Portal For Ankle Arthroscopy. J Bone Joint Surg Br.1997;79:650-2.
5. Frank RM, Hsu AR, Gross CE, Walton DM, Lee S. Open and Arthroscopic Surgical Anatomy of the Ankle. Hindawi Publishing Corporation Anatomy Research International Volume 2013, ArticleID 182650,9pages.
6. Stetson WB, Ferkel RD. Ankle arthroscopy I:Technique and Complications. J Am Acad Orthop Surg 1996;4:17-23.
7. Ferkel RD. Ankle and Foot Arthroscopy Contemporary Approach to Diagnosis and Treatment. (?)
8. Golano P, Vega J, Carro LP, Gotzens V. Ankle Anatomy for the Arthroscopist Part 1: The Portals. Foot Ankle Clin N Am 11 (2006) 253-273.
9. Woo SB, Wong TM, Chan WL, Yen CH, Wong WC, Mak KL. Anatomic variations of neurovascular structures of the ankle in relation to arthroscopic portals: a cadaveric study of Chinese subjects. Journal of Orthopaedic Surgery 2010.18(1):71-5
10. Sitler DF, Amendola A, Bailey CS, Thain LMF, Spouge A. Posterior Ankle Arthroscopy An Anatomic Study. JBJS.ORG 2002.84(5):763-769.
11. Balci HI, Polat G, Dikmen G, Atalar A, Kapicioglu M, Asik M. Safety of posterior ankle arthroscopy portals in different ankle positions: a cadaveric study. European Society of Sports Traumatology, Knee Surgery, Arthroscopy 2014.DOI 10.1007/s00167-014-3475-6
12. Scholten PE, Dijk CNV. Combined Posterior and Anterior Ankle Arthroscopy. Case Reports in Orthopedics 2012, Article ID 693124, 4 pages.
13. Zengerink M, Dijk CNV. Complications in ankle arthroscopy. Knee Surg Sports Traumatol Arthrosc (2012) 20:1420–1431.
14. Ilyas J. Ankle Arthroscopy. http://dx.doi.org/10.5772/54013.
15. Chen YC. Clinical and cadaver studies on the ankle joint arthroscopy. J Jpn Orthop Assoc 1976;50:631-51.
16. Feiwell LA, Frey Cankle 1993;14:142-147 :Anatomic study of arthroscopic portal sites of ankle. Foot
17. Basar'r K, Esmer AF, Tuccar E, Binnet M, Güçlü B. Medial and Lateral Malleolar Arteries in Ankle Arthroscopy: A Cadaver Study. The Journal of Foot and Ankle Surgery 2007.
18. Das S, Suhaimi FH, Latiff AA, Hlaing KPP, Ghafar NA, Othman F. Absence of the peroneus tertius muscle: cadaveric study with clinical considerations. Romanian Journal of Morphology and Embryology 2009, 50(3):509 - 511.
19. Dijk CNV. Ankle Arthroscopy: Techniques Developed by the Amsterdam Foot and Ankle School. 32-33.ISBN:978-3-642-35989-7(Online)
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





