IJCRR - 7(11), June, 2015
Pages: 01-04
Print Article
Download XML Download PDF
A STUDY ON POSTKERATOPLASTY ASTIGMATISM AND CO- RELATION
Author: Sohan Lohiya, Ruchita Lohiya
Category: Healthcare
Abstract:Introduction: Post-operative visual status after successful penetrating keratoplasty depends mainly on the clarity of the graft and the refractive error, particularly the astigmatic component. Severe irregular astigmatism is often seen after keratoplasty which can delay visual rehabilitation, even with a clear graft. Aim: The aim of this study was to co-relate post- keratoplasty astigmatism by using different number of sutures and different donor graft sizes. Material and Method: In this prospective study, 80 eyes of patients underwent penetrating keratoplasty with interuppted suturing techniques with different numbers of sutures and by using different size of donor graft size. Conclusion: Post operative corneal irregular astigmatism was noted to be more common with increased number of sutures and large donor graft size.
Keywords: Penetrating keratoplasty, Astigmatism
Full Text:
INTRODUCTION
Penetrating keratoplasty (PK) has emerged as a relatively safe means of restoring vision in corneal opacities and irregularities. Astigmatism is the most common cause of suboptimal vision after corneal transplantation despite a clear corneal graft [1, 2]. A clear corneal graft may be an optical failure if high astigmatism limits visual acuity. Intraoperative measures to reduce postkeratoplasty astigmatism include round and central trephination of cornea with an adequate size, appropriate sutures with evenly distributed tension, and perfect graft-host apposition. Suture manipulation has been described for minimising early postoperative astigmatism. In addition, we investigated the final astigmatic outcome after suture removal. Based on several studies, 15–31% of patients undergoing PK may develop postoperative astigmatism greater than 5 diopters (D) [3–5]. The astigmatism can be irregular with associated higher-order aberrations that can ultimately limit the vision obtained and add to patient’s inability to wear standard optical correction [6]. This explains why visual acuity in 10–20% of PK cases cannot be corrected satisfactorily by spectacles or contact lenses [7–9].
AIMS AND OBJECTIVES
We studied the cases with penetrating keratoplasty,
1. To compare the amount of astigmatism after the operation with different number of sutures using interrupted suture techniques
2. To compare the amount of astigmatism by using different donor graft sizes
3. To study the post-keratoplasty visual status
MATERIAL AND METHOD
This prospective study was performed on patients who underwent penetrating keratoplasty between January 2008 and Dec 2012 by one surgeon. Informed consent was obtained from the included subjects. During investigations, the subjects who showed delayed wound healing more than 3 weeks, graft rejection, newly developed intractable glaucoma, or with wound problems such as dehiscence and those with combined cataract or glaucoma surgery were excluded. The patients were followed up for at least18 months. In all cases, interrupted suturing with 10/0 nylon was done. Routine follow-up schedule every weekly for first month, biweekly for second month, monthly for 3 to 6 months, and every three months for one year was followed. Patients compliant with this schedule were called “Regular Follow Ups.” Selective suture removal was started from third month onward, after assessing tightness of sutures on slit lamp examination, and calculating astigmatism by Retinoscopy.
OBSERVATIONS AND RESULTS
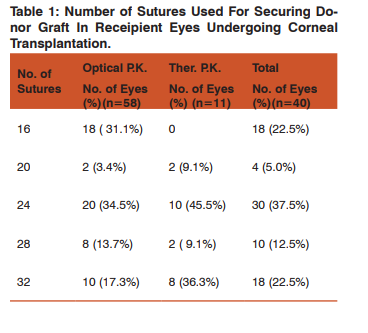
In this study interrupted 10 O Nylon suture were used in all the cases undergoing penetrating keratoplasty, for securing donor graft in recipient’s eyes. Number of sutures was 16-24 in 52 (65%) eyes whereas 28-32 sutures were used in 28 (35%) eyes. (Table 1)
ASTIGMATISM AND NUMBER OF SUTURE
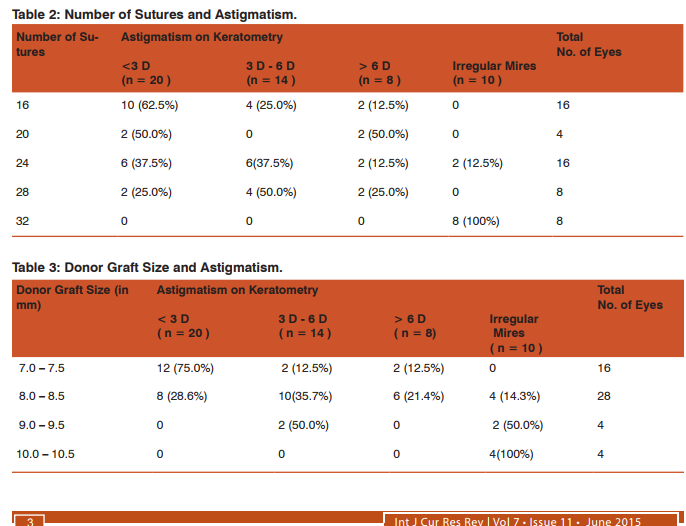
On post operative keratometry corneal astigmatism more than 3 D was noted to be more with increase in number of sutures used to secure donor graft. Irregular astigmatism was noted to be more common with increased number of sutures. (Table 2 ) ASTIGMATISM AND GRAFT SIZE Post operative corneal astigmatism on keratometry was noted to increase with increased size of donor graft. Irregular astigmatism was noted to be more common with large donor graft size. (Table 3 )
POST-OPERATIVE VISUAL STATUS
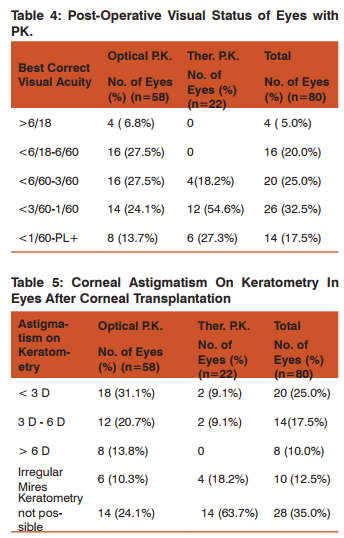
Out of 80 eyes included in this study in whom penetrating keratoplasty was performed post operative visual acuity in the operated eye was found to be >6/60 in 20 (25.0%) eyes and 20 (25.0%) eyes had visual acuity 6/60 in 20 (25.0%) eyes and 20(25.0%) eyes had visual acuity <6/60-3/60. In 26 (32.5%) eyes post operative visual acuity was <3/60- 1/60 and 14(17.5%) eyes had post operative visual acuity <1/60 to Perception of light. Vanathi et al (2005) reported that of the 53 eyes with repeat penetrating keratoplasty the best corrected visual acuity of the 28 clear grafts ranged from 4/60 to 6/9, only 5 eyes (9.4%) achieved best corrected visual acuity of 6/18 or better at the end of 1 year after re-grafting[10]. Valery et al (2001) reported that 44 of the 86 eyes (51%) had clear grafts, but only 39.5% had good visual outcome. Visual acuity also decreased with time. Final visual acuity was 20/20 to 20/40 in 13 of the 86 eyes (15%), 20/80 to 20/200 in 23 eyes (27%), and less than 20/200 in 50 eyes (58%). [11] Claesson et al (2002) reported that visual acuity improvement in patients, with keratoconus and Fuch’s dystrophy was 86% and 54% respectively compared with only 31% of bullous keratopathy and 35% in the “other diagnosis” group. In the present study post operative corneal astigmatism on keratometry was recorded 8-12 weeks after corneal transplantation. Astigmatism less than 3 D was noted in 20(25.0%) eyes, 14 (17. 5%) had astigmatism between 3 D – 6 D and astigmatism more than 6 D was noted in 8 (10.0%) eyes. Irregular mires were noted in 10 (12.5%) eyes. Carmen et al (2002) reported in his study on 30 eyes (28 patients) who underwent keratoplasty for keratoconus that all the patients had a continuous myopic shift to – 1.02 + 2.65 diopters 2 years postoperatively. This was associated with significant increase in the mean keratometry levels from + 41.72 + 2.96 diopters at 1 month postoperatively to + 43.77 + 2.29 diopters 2 years postoperatively. Soong et al (2000) reported that following tectonic keratoplasty the mean + SD change in keratometric astigmatism in the parent penetrating keratoplasty was 1.75 + 1.50 diopters. The astigmatism increased in 10 cases (60.6%), decreased in three (20%), and remained unchanged in two (13.3%). [12] Claesson et al (2002) reported that Postoperative astigmatism was higher in the bullous keratopathy group (4.7D).
CONCLUSION
On post operative keratometry corneal astigmatism more than 3 D was noted to be more with increase in number of sutures used to secure donor graft and was noted to be directly related with size of donor graft and number of sutures. Post operative visual acuity in the operated eye was noted to be >6/60 in 25.0%, <6/60-3/60 in 25.0% . In 32.5% eyes post operative visual acuity was <3/60-1/60 and 17.5% eyes had post operative visual acuity <1/60 to Perception of light. Hence, Corneal surgeons should tailor a specific plan, on the basis of patient’s needs and clinical situations, to score advantages of each intervention.
ACKNOWLEDGEMENT
We acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. K. A. Williams, N. B. Hornsby, C. M. Bartlett, et al., “Report from the Australian corneal graft registry,” Tech. Rep., Snap Printing, Adelaide, Australia, 2004.
2. N. C. Price and A. D. Steele, “The correction of post-keratoplasty astigmatism.,” Eye, vol. 1, part 5, pp. 562–566, 1987. View at Scopus
3. R. C. Troutman and M. A. Lawless, “Penetrating keratoplasty for keratoconus,” Cornea, vol. 6, no. 4, pp. 298–305, 1987. View at Scopus
4. K. A. Williams, D. Roder, A. Esterman, S. M. Muehlberg, and D. J. Coster, “Factors predictive of corneal graft survival: report from the Australian corneal graft registry,” Ophthalmology, vol. 99, no. 3, pp. 403–414, 1992. View at Scopus
5. R. J. Olson, M. Pingree, R. Ridges, M. L. Lundergan, C. Alldredge Jr., and T. E. Clinch, “Penetrating keratoplasty for keratoconus: a long-term review of results and complications,” Journal of Cataract and Refractive Surgery, vol. 26, no. 7, pp. 987–991, 2000. View at Publisher · View at Google Scholar · View at Scopus
6. M. S. Rajan, D. P. S. O’Brart, P. Patel, M. G. Falcon, and J. Marshall, “Topography-guided customized laser-assisted subepithelial keratectomy for the treatment of postkeratoplasty astigmatism,” Journal of Cataract and Refractive Surgery, vol. 32, no. 6, pp. 949–957, 2006. View at Publisher· View at Google Scholar · View at PubMed· View at Scopus
7. R. C. Troutman and C. Swinger, “Relaxing incision for control of postoperative astigmatism following keratoplasty,” Ophthalmic Surgery, vol. 11, no. 2, pp. 117–120, 1980. View at Scopus
8. J. H. Krachmer and R. E. Fenzl, “Surgical correction of high postkeratoplasty astigmatism. Relaxing incisions vs wedge resection,” Archives of Ophthalmology, vol. 98, no. 8, pp. 1400–1402, 1980. View at Scopus
9. G. W. Lavery, R. L. Lindstrom, L. A. Hofer, and D. J. Doughman, “The surgical management of corneal astigmatism after penetrating keratoplasty,” Ophthalmic Surgery, vol. 16, no. 3, pp. 165–169, 1985. View at Scopus
10. Vanathi et al. Indications and outcome of repeat penetrating keratoplasty in India, BMC, Ophthalmology,5:26,2005
11. Valery et al. The Profile of Repeated Corneal Transplantation, Ophthalmology 108:461-469, 2001.
12. Soong et al. Small, Overlapping Tectonic Keratoplasty Involving Graft-Host Junction of Penetraing Keratoplasty, American J Ophthalmol 129:465-467, 2000.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





