IJCRR - 7(13), July, 2015
Pages: 54-57
Print Article
Download XML Download PDF
INVESTIGATION OF AN OUTBREAK OF CHOLERA IN SANKHEDA VILLAGE OF CHHOTAUDEPUR DISTRICT, GUJARAT
Author: Nikhil Patel, Bhavesh Shroff, V.S. Mazumdar
Category: Healthcare
Abstract:Aim: Investigation of an outbreak of Cholera in Sankheda village of Chhotaudepur district, Gujarat Introduction: Diarrheal disease outbreaks are causes of major public health emergencies in India. We investigated such outbreak in Sankheda village of Chhotaudepur district, Gujarat to identify the etiological agent, source of transmission and propose control measures. Methodology: This study was conducted by a rapid response team as an investigation of outbreak to find out the root cause during the emergency response. The information was entered and analyzed anonymously. The study was implemented in collaboration with the district health officials Results and Conclusion: The outbreak was caused by Vibrio cholerae 01 Biotype Ogawa. Cases were localized to clusters of village depending on distribution of contaminated water.
Keywords: Cholera, Contaminated water
Full Text:
INTRODUCTION
Cholera is a waterborne disease characterized by acute severe watery diarrhea followed by vomiting, rapid dehydration, muscular cramps and suppression of urine. The organism which causes Cholera is labelled as V. cholera O1 (more recently also V.cholerae O139), which colonizes the small intestine and produces an enterotoxin responsible for a watery diarrhea. Person with cholera may die of dehydration in a matter of hours after infection without prompt treatment. Cholera outbreaks are generally associated to contaminated food and water supplies. Cholera was confined only to the Indian sub-continent until 19th century.1 In this region, Cholera outbreaks were seasonal with one or two peaks per year2 and from here, cholera was spread throughout the world seven times since 18173. The last pandemic began in 1961 in Indonesia, spread through the Asian continent during the 60’s, reached Africa in 19704and Latin America in 1991.
MATERIAL AND METHODS
This study was conducted by a rapid response team as an investigation of outbreak to find out the root cause during the emergency response and was designed to provide information, so ethical approval was not sought prior to the study. It was undertaken as a public health practice rather than a research5,6. All inquiry was administered informed consents, ensured confidentiality and anonymity during and after the study. At the same moment health education was carried out in each household regarding cholera transmission and prevention. The information was entered and analyzed anonymously. The survey was carried out after obtaining permission from the district health officials.
The outbreak
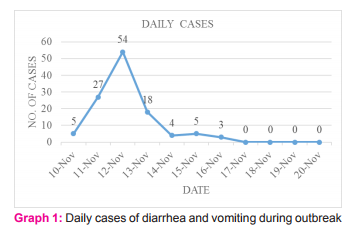
In November 2014, an outbreak of diarrhea and vomiting was reported from Sankheda village of Chhotaudepur district of Gujarat. Sankheda village having a population of 9406 with approximately 1800 Households (HH). People use tap water supplied by panchayat for drinking purpose. There were total two water tanks in village, which were supplied by 4 tube wells. As per the reports of Block Health Officer (BHO) affected population was 4318 and first case was reported on 9/11/2014. There were 2 deaths due to same outbreak,
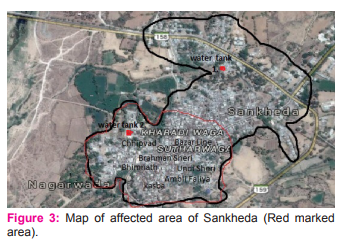
13 cases of diarrhea and vomiting were reported and hospitalized at CHC (Community Health Centre) Sankheda. So, surveillance to find other cases was started. The dean of Medical College, Baroda had constituted a Rapid Response Team (RRT) of Physician, Pediatrician, Microbiologist and Public health expert to investigate the reported outbreak on 12th of November. A map of location of water tank and tube well and the area supplied by them were made. Those who had complaints of diarrhea and vomiting were examined by the physician and pediatrician according to age and their stool samples were collected by microbiologist. The team then visited the families of those who had died due to diarrhea, elicited the history and then after the surrounding area was examined as well as water used for drinking purpose was checked. One significant finding in the history was that the both deceased had consumed water from same source, subsequently the water was found to be contaminated. The local people and the health personnel of the area suspected the quality of drinking water.
Microbiological aspects
Out of 73 stool samples sent for examination 14 samples were positive for V. cholera by the “hanging drop preparation” examination, colony and culture and sensitivity report. As reported by Public Health Laboratory, Baroda Medical College Vadodara, all three water sample sent from village were negative for chlorine and were not potable.
High risk geographical area
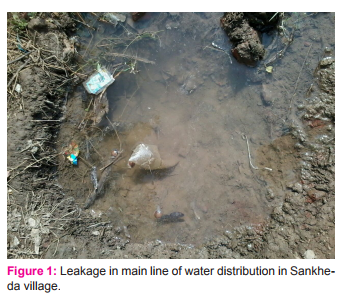
High risk geographical area was distribution area of 1 of the 2 drinking water supply tanks where leakages were found in distribution line. These areas were 10-12 clusters of total 18 clusters of Sankheda village. There were 13 leakages in water distribution pipes and out of them 3 were in direct contact of sewage.
RESULTS

DISCUSSION
An outbreak of cholera occurred in the Sankheda village of Chhotaudepur district in November 2014. After investigation, it was revealed that the outbreak occurred because of contaminated drinking water due to leakages found in the water pipes and bore-wells of Sankheda village. Contaminated water remains the prime vehicle for outbreaks of cholera in developing countries like India. Here at Sankheda, the affected areas have open sewage system. They have poor sanitation practices, lack of sewerage and toilets facility at residence and because of these, fecal contamination through leakages of water sources of households could be one of the possibilities. Hamne et al found same picture also in Varanasi, India and because of that hyper endemicity of water born diseases are present7 Almost 90% of patients had complaints of diarrhea, vomiting and other signs of dehydration on November 9,2014. A rapid response team was called on November 12,2014 from local authorities so there was three days of delay for initiation of epidemic investigation and man-agement. Similar to past studies of diarrheal disease outbreaks, there were certain limitation in the investigation. Secondly, we could only obtain laboratory confirmation from the limited numbers of indoor patients. Thus, we could not exclude other causes, which may be acting together or their own to cause this outbreak. However 14 positive patients out of 73 tested patients confirmed the outbreak of V. cholerae. So suspicion of V. cholerae was based on case definition compatible with V. cholerae definition of Integrated Disease Surveillance Project and Diagnosis of V.cholerae8 . Patients with complaints of diarrhea, vomiting and dehydration, irrespective of lab confirmation were also treated. The above limitations could have had an impact on the association of the outbreak and V. cholerae but main cause of outbreak was the contaminated drinking water.
Description of control measure taken
• Tap water supply was stopped and alternate supply by tanker was established.
• Repairing of 8 leakages in water supply line out of 13 leakages found was undertaken urgently.
• Chlorine tablets were distributed.
CONCLUSION
• It was concluded from the investigations that this outbreak of Cholera was caused by Vibrio Cholerae 01 Biotype Ogawa (Table-1) and the source of the infection was the consumption of contaminated water. Cases were not localized to any specific area but scattered in village depending on the consumption of the contaminated water.
Recommendation
• It is recommended in present situation that water supply should be safe and chlorinated. In affected area water supply by tanker should be continued till water quality is ensured
. • Repair of water distribution system, and if possible chlorination of water by chlorine gas as well as monitor chlorine level at source and end user.
• Chlorine tablet must be distribute and educate them how to use.
• Health education regarding water borne diseases, water safety and importance of personal hygiene should be taken up.
• Water supply system assessment is vital to look for leakages and blocked sewage lines should be cleared urgently.
ACKNOWLEDGEMENT
We would like to acknowledge contribution of the members of rapid response team of Medical College and S.S.G. Hospital, Baroda, which includes Dr. Jignesh Vasava (Assistant Professor, Dept. of Medicine) Dr. Tarun Parikh (Assistant Professor, Dept. of Pediatrics) Dr. Neelam Pandya (Assistant Professor, Dept. of Microbiology)for their valuable contribution during field visit. We are equally thankful to Dr. Vaishali, the Block Health Officer and Medical Officer and staff members of Gundiya PHC (Public Health Centre), for their co-operation during field survey. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript .The authors are also grateful to authors / editors /publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.

References:
1. Islam MS, Miah MA, Hasan MK, Albert MJ., Detection of non-culturable Vibrio cholera 01 associated with a cyanobacterium from an aquatic environment in Bangladesh. Transactions of the Royal Society of Tropical Medicine And Hygiene. 1994; 88:298-299.
2. Faruque SM, Albert MJ, Mekalanos JJ., Epidemiology, genetics and ecology of toxogenic Vibrio cholera.Microbiology and Molecular Biology Reviews.1998;62:1301-1314
3. Morillon M, De Pina JJ, Husser JA, Baundet JM, Bertherat E, Martet G., Djibouti, histoire de deuxepidemies de cholera:1993-1994. Bull Soc Path Ex.1998;91:407-411.
4. Islam MS, Drasar B, Bradley SR. Probable role of Bluegreen algae in maintaining endemicity and seasonality of cholera in Bangladesh: a hypothesis. J Diarrhoel Dis Res. 1994;12:245-256.
5. Washington State University institutional Review Board (IRB).Definitions, Washington State University, Pullman WA. (Internet) Available from : http:/www.irb.wsu.edu/ definitions.asp(updated May 2010), (Last cited on 2011 August 19).
6. Snider DE Jr, Stroup DF. Defining research when it comes to public health. Public Health Rep 1997;112;29-32 (PUBMED)(FULL TEXT).
7. Hamner S, Tripathi A, Mishra RK, Bouskill N, Broadway SC, Pyle BH, et al. The role of water use patterns and sewage pollution in incidence of water- borne/ enteric disease along the Ganges River in Varansi, India. Int J Environ Health Res 2006:16:113-32 (PUBMED)(FULL TEXT).
8. Integrated Disease Surveillance Project, India. Modified case definition for p-form(internet). Medical officers’ Manual, IDSP, 2006. Available from: http://www.idsp.nic.in/idsp/ IDSP/Case_Def_P_Form.pdf. (Updated 2008); (Last cited on 2011 June 21).
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





