IJCRR - 7(16), August, 2015
Pages: 34-48
Date of Publication: 21-Aug-2015
Print Article
Download XML Download PDF
EVALUATION OF ADOLESCENT FRIENDLY HEALTH SERVICES (AFHS): CLIENTS' PERSPECTIVES
Author: Dinesh Kumar, R.J. Yadav, Arvind Pandey
Category: Healthcare
Abstract:Context: Adolescent period is hazardous for adolescent health due to absence of proper guidance and counseling, which have not received proper attention and guidance because of which the need of Adolescent Friendly Health Services (AFHS) is emphasized. Continuous monitoring and evaluation of established Adolescent Friendly Health Clinics (AFHC) is desirable. Aim: Evaluation of selected Adolescent Friendly Health Services (AFHS) with clients' perspectives. Methods: Evaluation study was conducted at two health facilities during November 2012 to February, 2013. Existing patterns of Adolescent Friendly Health Services (AFHS) were evaluated based on clients' exit interviews in selected health facilities. Exit interviews of adolescents (clients) from selected AFHC and other OPD were conducted. Evaluation of AFHC was done based on its desired characteristics of availability, accessibility, and acceptability. Results: Majority of respondents were self motivated to attend these clinics. Maximum number of clients took 30-60 min to approach the health facility. The physical environment in terms of waiting area was reportedly good by 21.7% clients of AFHC. Reading material was available as reported by 56.5% AFHC clients and 43.4% found the material interesting. Friendly behavior of doctors was reported by 100% clients but only by 90.9% respondents attending other OPDs. Confidentiality was maintained in most of cases. Overall satisfaction rates were 78.0% for AFHC clients and 73.0% for other respondents and about 65.0% AFHC clients were encouraged to recommend these services to their friend also. Suggestions regarding free services to be provided were given by 52.1% clients whereas 34.7% AFHC clients reported long waiting time. Majority of clients attending AFHC were in favor of separate discussion with doctors.
Conclusions: Study concludes that Adolescent Friendly Health Services (AYFHS) need some improvements to provide appropriate services to them to make them available, accessible, and acceptable. Existing services were found to be lacking in terms of maintaining privacy of clients. Adolescent Friendly Health Initiatives (AFHI) should be developed and monitored at different levels as ongoing efforts using newer methodology and evaluation techniques.
Keywords: Adolescent friendly health services (AFHS), Adolescent friendly health initiatives (AFHI); Adolescent reproductive and sexual health (ARSH)
Full Text:
INTRODUCTION
Adolescents are the most dynamic, creative, productive and enthusiastic group of population but also the most neglected groups by our society and policy makers. The World Health Organization (WHO) promotes Adolescent Friendly Health Services to address these issues and make it easier for adolescents to obtain the required services. Viewing adolescents as a specific group with their own needs is a relatively recent practice, especially in the developing world; India has identified adolescent reproductive and sexual health (ARSH) as a key strategy under the Reproductive and Child Health Programme Phase II (RCH-II) and the National Rural Health Mission (NRHM). Strategy for ARSH has been approved as part of the RCH-II. There are various programs available for adolescents and youths in different states. Initiative like “Adolescent Friendly Health Services (AFHS)” introduced in the schools is one of important efforts in this direction. Ministry of Health and Family Welfare (MoHFW) has de veloped guidelines and training package for operationalizing AFHS. Haryana is one of the first states in the country to have launched a distinct Adolescent Reproductive and Sexual Health (ARSH) program providing AFHS at government health facilities. The National Program Implementation plan of the RCH II has proposed to expand this program to 75 districts in the country. The AFHS project under RCH II in Haryana employs an “Adolescent Action Group” (AAG) to plan interventions with clear targets and roles and responsibilities. ARSH was implemented in Haryana in 2008 in nine districts with the objective of providing adolescent friendly health services through the existing public sector health facilities. Reproductive Health Services under the public sector are more oriented towards adult married women, while unmarried adolescents hesitate to seek health services due to the fear that these services are not confidential, inability to pay, requirement of parents’ approval and negative or insensitive attitude of health providers1 . For many adolescents who need sexual and reproductive health services, such as appropriate information, contraception and treatment for sexually transmitted infections, these are either not available or are provided in a way that makes adolescents feel unwelcome and embarrassed. Even married adolescent girls shy away from seeking healthcare due to sheer embarrassment and the taboo associated with reproductive and sexual health problems2 . This creates an “unmet need” for reproductive and sexual healthcare. This unmet need varies among married and unmarried adolescents Actions taken during adolescence can affect a person’s life opportunities, behavioral patterns and health. Adolescent period is hazardous for adolescent health due to absence of proper guidance and counseling, which have not received proper attention and guidance because of which the need of Adolescent Friendly Health Services (AFHS) is emphasized. AFHS provides a broad range of preventive, promotive and curative services under one roof can help to ensure improved availability, accessibility and utilization of health services. According to WHO3 , Adolescent-Friendly Health Services (AFHS) are accessible, acceptable and appropriate in terms of right place, at the right time, and affordable. WHO promotes Adolescent Friendly Health Services to address these issues. There are several AFHI’s undertaken by some NGOs in India such as Mamta, Nehru Yuva Kendra etc. MAMTA, an NGO to establish a model of AFHS through the public health system in villages of Delhi, runs the clinic, called Friends’ Clinic focusing the needs of the local youth population providing clinical and counseling services4 . Nehru Yuva Kendra acts as an health awareness unit through active participation of the young; Kishori Shakti Yojana is to improve the health and nutritional status of the girls; Balika Samridhi Yojana is to delay the age of marriage; Mahila Samakhya Programme - stresses on equal access to education facility for adolescent girls and young women; school age education. Yadav et al (2009)5 observed that proportion of adolescent girls visiting the AFHCs in Delhi and Kolkata was higher whereas the situation was reverse in Chandigarh. Present study was undertaken with an objective of evaluating selected Adolescent Friendly Health Clinics (AFHC) with clients’ perspectives.
MATERIAL AND METHODS
This study was undertaken during November 2012 to February, 2013 at two health facilities: Kamla Nehru Memorial Hospital Allahabad, Uttar Pradesh, India, Sarojini Naidu Children Hospital Allahabad, Uttar Pradesh, India attached with M.L.N. Medical College Allahabad and GMCH Chandigarh (UT) India. Existing patterns of Adolescent Friendly Health Services (AFHS) were evaluated based on clients’ exit interviews in selected health facilities. . Exit interviews of adolescents (clients) from selected AFHC and other OPD were conducted regarding their problems, services offered and satisfaction thereof. Evaluation of AFHC was done based on its desired characteristics of availability, accessibility, and acceptability. Prior permissions from concerned authorities were taken for conducting the study. Exist interviews were taken only of clients willing of participating in the study and confidentiality of their responses was ensured following Ethical Guidelines of ICMR. Because of some time, financial and other constraints, study could not be extended further in terms of inclusion of more AFHC’s in other cities.
RESULTS
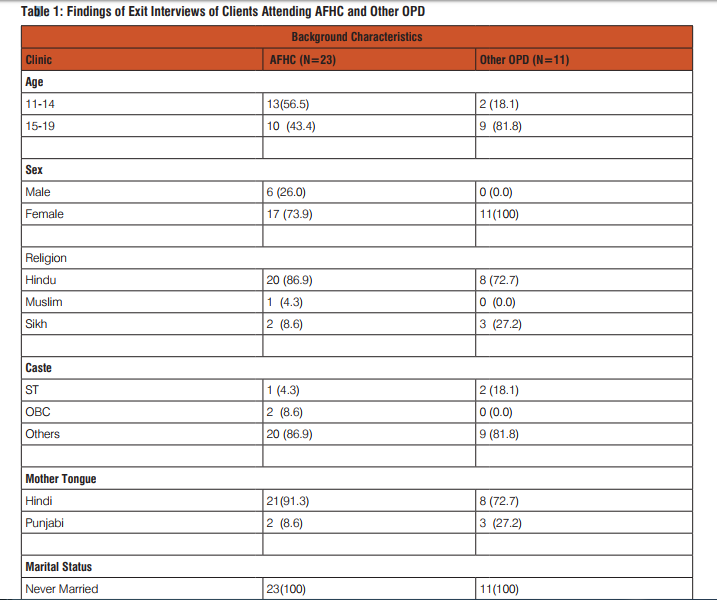
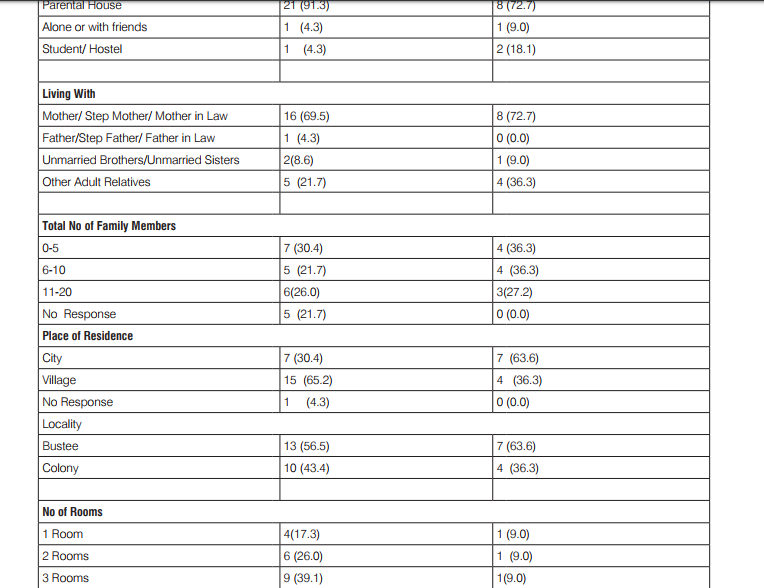
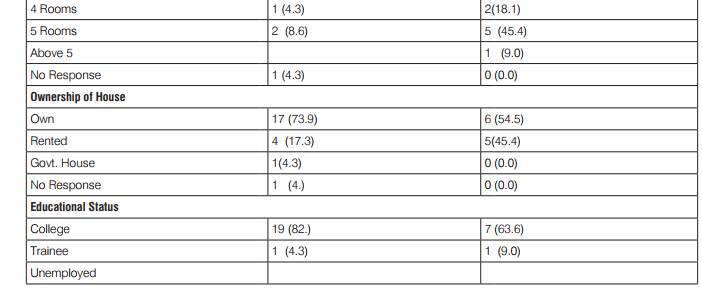
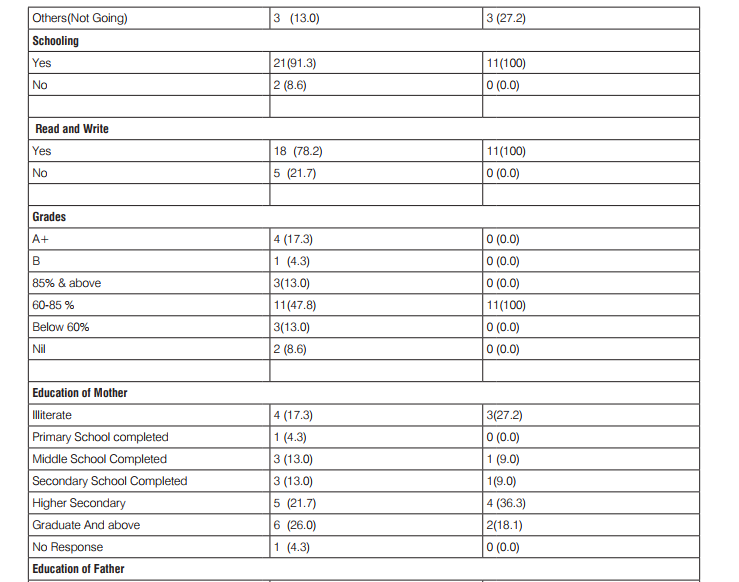
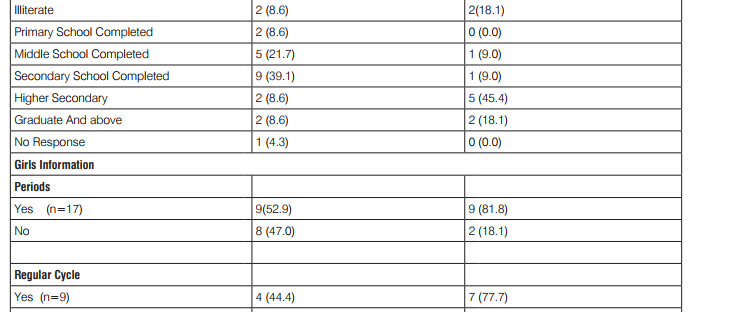
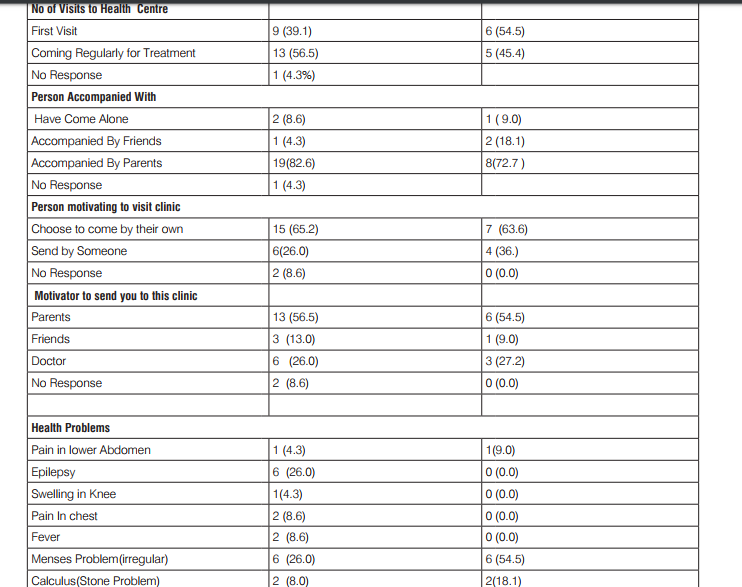
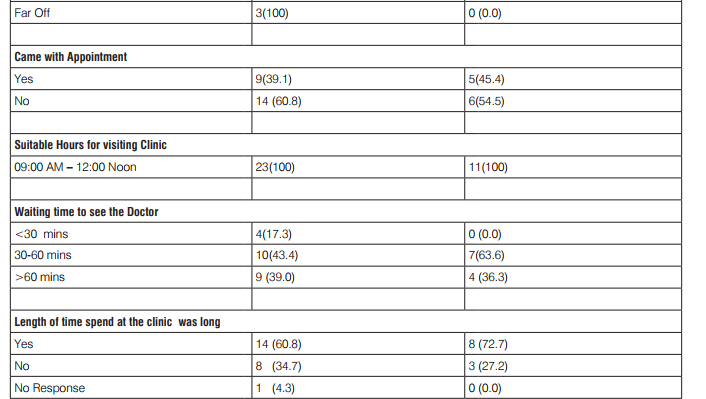
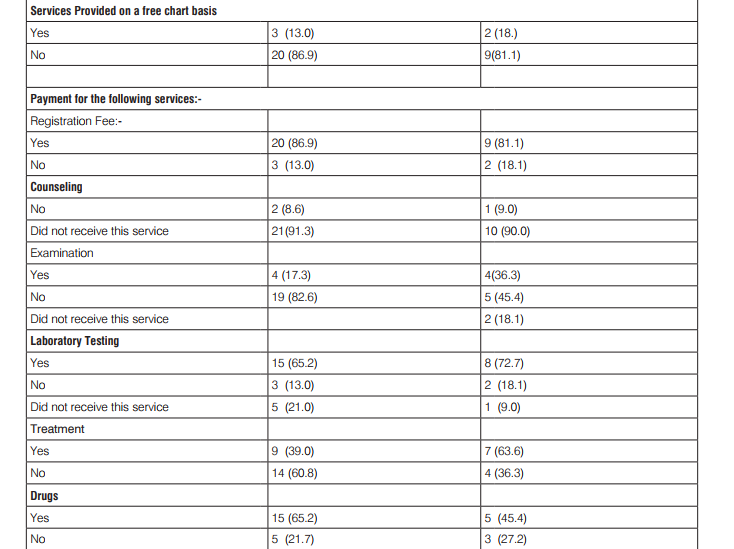
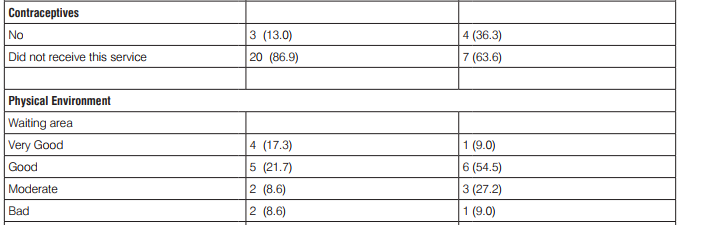
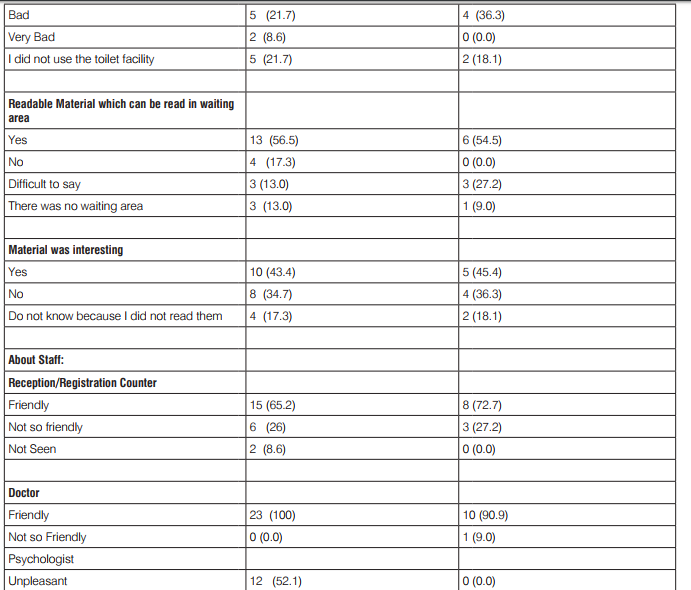
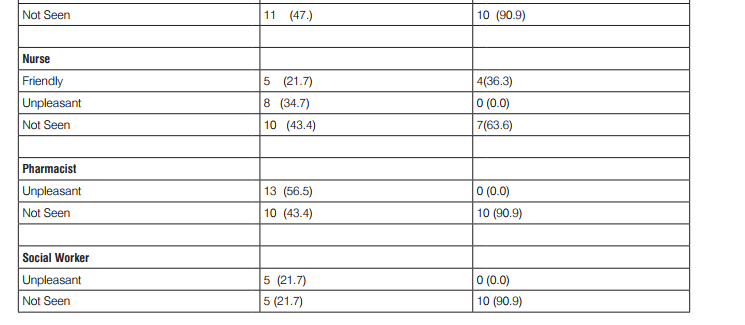
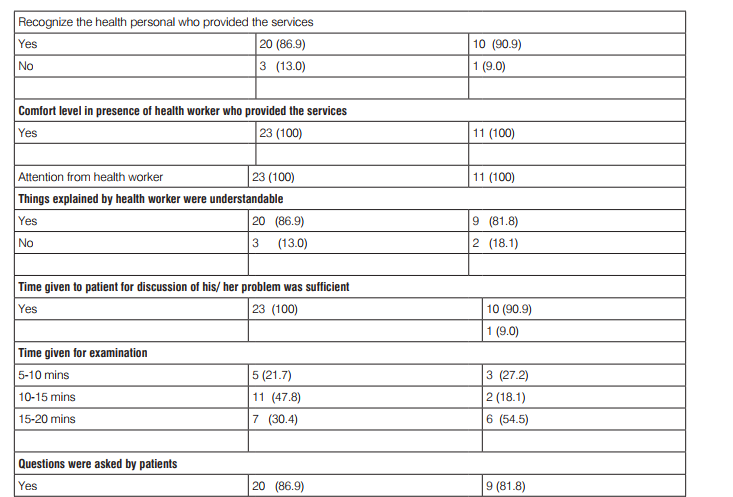
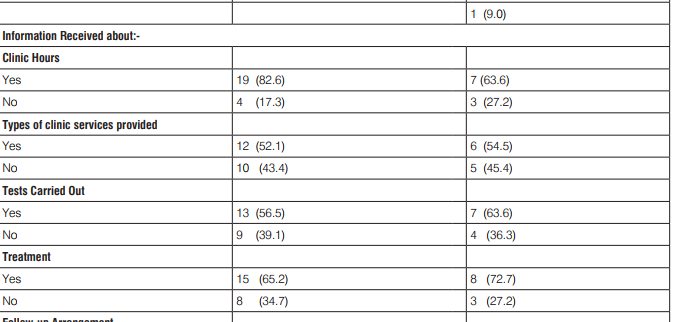
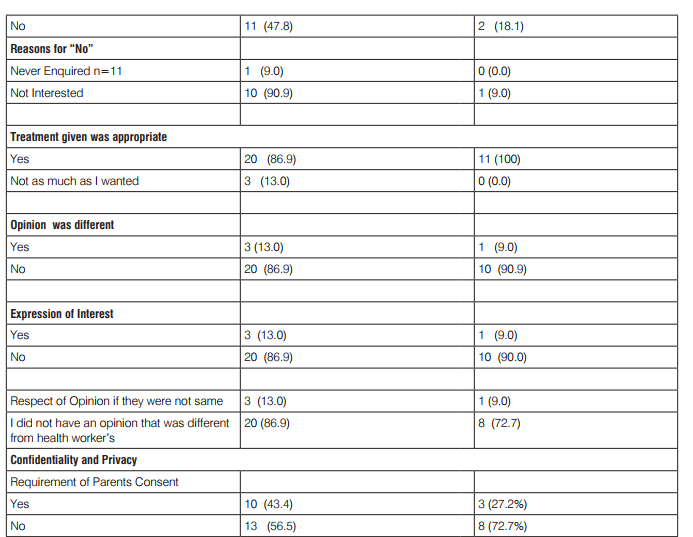
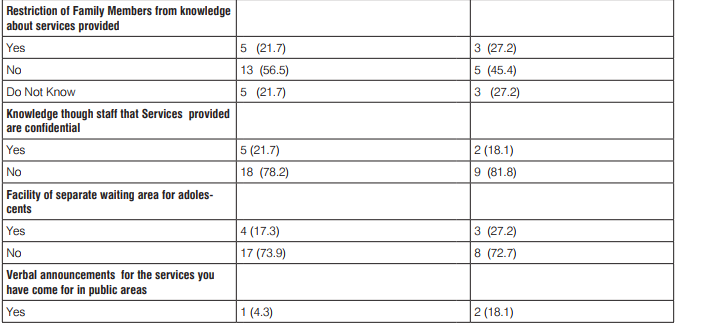
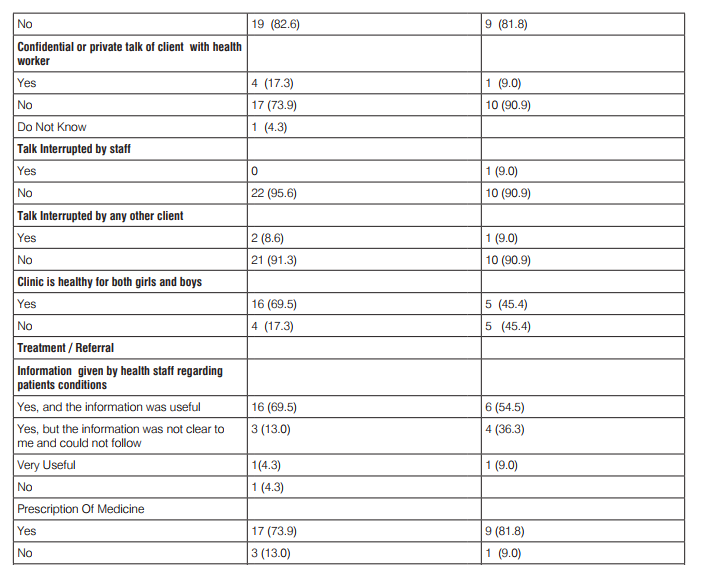
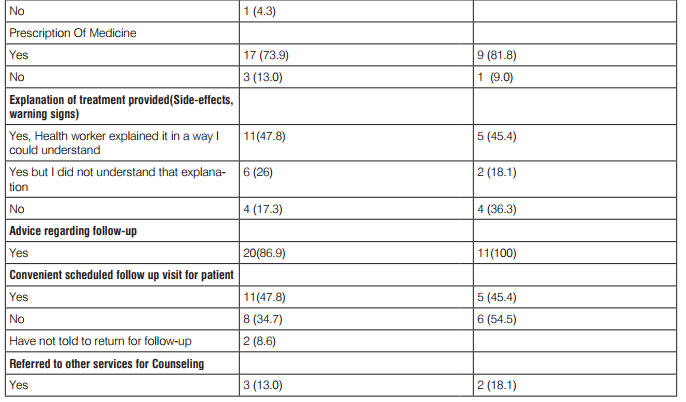
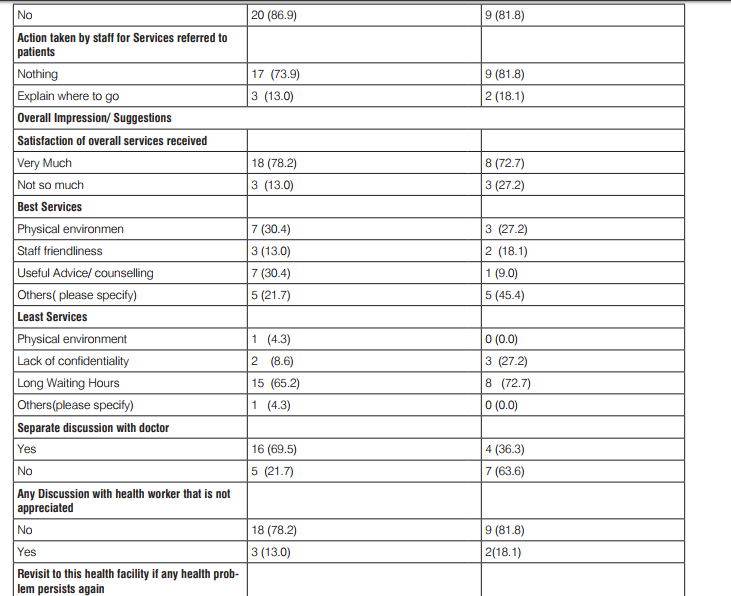
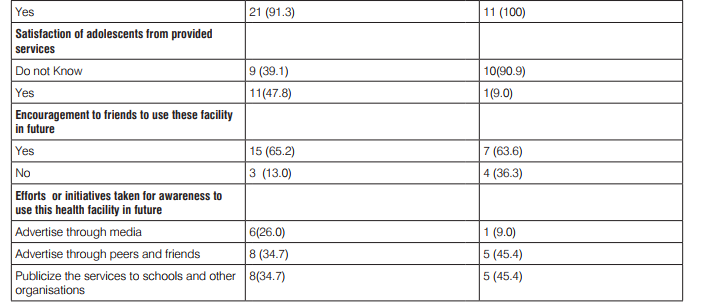
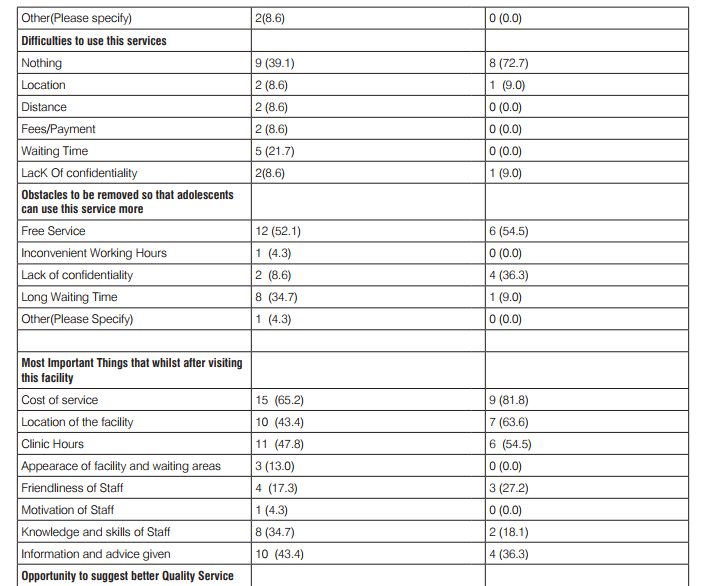
A total of 23 adolescents attending AFHC and other OPD were studied. Some important findings are presented in Table-1. There were 13 (56.5%) boys and 10(43.4%) girls in the age group 11-19 years. There were 26.1% male clients 73.9% female clients in AFHC clients from while other OPD’s were only females as they were mainly selected from Gynecology OPD. Respondents were mostly Hindus belonging to general category all were unmarried mostly living with parents. There were 91.3 % clients studying while all respondents attending other OPD’s were studying. Out of all AFHC girl clients 9(52.9%) and out of all girls attending other OPD, 9 (81.1%) have attends menarche. Among these girls 44.4% AFHC client and 77.7% other attendees reported regular cycle. Majority of respondents were self motivated to attend these clinics. They attended the clinic with several health problems listed maximum number of clients took 30-60 min to approach the health facility. No prior appointments was found in most of the cases and mostly had to wait 30-60 min to consult the doctor. No counseling was done in the most of the cases and most of them were not availing contraceptive service. The physical environment in terms of waiting area was reportedly good by 21.7% and 54.5% respondents. Reading material was available as reported by 56.5% AFHC clients and 43.4% found the material interesting. Friendly behavior of doctors was reported by 100% clients but only by 90.9% respondents attending other OPDs. Doctors took about 10-15 min as reported by 47.8% AHFC clients and 18.1% other respondents. Confidentiality was maintained. They received all relevant information up to a satisfaction level. About 78.0% AFHC clients 73.0% other respondents were satisfied with overall services whereas 34.7% AFHC clients reported long waiting time. About 65.0% AFHC clients were encouraged to recommend these services to their friend also. Suggestions regarding free services to be provided were given by 52.1% clients. About 69.0% AFHC clients were of the opinion in favor of availing opportunities of separate discussions with doctors in privacy.
DISCUSSION
Addressing adolescents provide not only health benefits in terms of delaying age at marriage, reducing incidence of teenage pregnancy, prevention and management of obstetric complications including access to early and safe abortion services and reduction of unsafe sexual behavior etc. but also economic and other benefits due to improved productivity and will help in protection of human rights. Health services have to be sensitive to the needs and developmental attributes of adolescents to be able to attract them6 . More young people now need reproductive health care, especially prevention services. These arguments strongly advocate the need of establishing AFHC. It is a known fact that adolescents first approach their peers for advice on sexual or reproductive issues. In the present study, majority of respondents were self motivated to attend these clinics mostly without any prior appointment and mostly had to wait 30-60 min to consult the doctor. There may be several reasons why the present health services are not accepted well by adolescents such as lack of knowledge regarding availability and accessibility of services, cultural reasons, lack of confidentiality, long way away or expensive services, lack of friendliness services, poorly trained staff, physical or logistical restrictions, gender barriers, and peer pressure etc. as observed in the present study also. Seventy two percent girls and 56% boys reported health problems during survey. only 43% girls and 35% boys reported to the clinic voluntarily to seek help and only one fifth the amount of problems were reported at the clinic in comparison to the quantum of problems reported in survey, which probably reflects a poor health seeking behavior by Joshi et al (2006)7 . No counseling was done in the most of the cases and most of them were not availing contraceptive service as observed in the present evaluation. The physical environment in terms of waiting area was reportedly good only by 21.7% AFHC clients and 54.5% other OPD clients. They received all relevant information up to a satisfaction level. Confidentiality and the quality of care are major concerns among adolescents. Present study reported that confidentiality was also maintained in most of the cases. Utilization of AFHC could be improved by intensive information, education and communication (IEC) strategies raising awareness on reproductive health and gender related issues. Reading material was available as reported by 56.5% AFHC clients and only 43.4% found the material interesting. Overall satisfaction rates were found to be about 78.0% among AFHC clients and 73.0% among other respondents whereas 34.7% AFHC clients reported long waiting time. About 65.0% AFHC clients were encouraged to recommend these services to their friends also. About 52.0% AHHC clients desired free services to be provided which needs further considerations. Existing services were found to be lacking in terms of confidentiality/privacy as about 69.0% AFHC clients were of the opinion that there should be opportunity of separate discussions with doctors in privacy. No earlier study is available on evaluation of AFHC in Indian set-up5 .
Conclusions and Suggestions
Existing services were found to be lacking in terms of maintaining privacy of clients. Adolescents felt need some improvements in AFHC. More users friendly AFHS need to be established and extended with desired characteristics of availability, accessibility, and acceptability. Further insight should be given to understand problems of adolescents attending AFHC and for evaluation of AFHS in a better way. Adolescent Friendly Health Initiatives (AFHI) should be developed and monitored at different levels as ongoing efforts.
ACKNOWLEDGEMENTS
The present paper is based upon some work conducted during Short Term Fellowship/Training in Indian Institute under HRD Scheme of Department of Health Research (DHR), Ministry of Health and Family Welfare, Govt. of India. I owe my sincere thanks to the Department of Health Research, Ministry of Health and Family Welfare, Govt. of India for award of this Short Term Fellowship/Training. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are also grateful to Reviewers for their valuable comments and improvements suggested.



References:
1. Mamdani M. Adolsecent reproductive health: Experience of community based programmes. In: Pachauri S, editor. Implementing a reproductive health agenda in India: The Beginning. New York: Population Council; 1999.
2. Bang R, Bang A. A community Study of Gynaecological Diseases in Indian Villages. In Zeidenstein and Moore, editors. Learning about sexuality: A practical beginning. New York: The Population Council; 1989
3. Peter McIntyre. Adolescent Friendly Health Services —An Agenda for Change WHO, Oxford, UK 2002.
4. Agrawal D, Mehra S, Mishra RK, Pandey SP. Road Map for implementing youth friendly services in Indian public health system. Paper presented at International conference on “Investing in young people′s health and development: Research that improves policies and programs” held at Abuja, Nigeria from April 27-29, 2008.
5. R.J. Yadav, Rajesh Mehta, Arvind Pandey and Tulsi Adhikari. Evaluation Of Adolescent-Friendly Health Services In India.. Health and Population: Perspectives and Issues Vol. 32 (2), 96- 104, 2009.
6.http://www.searo.who.int/entity/child_adolescent/topics/adolescent_health/adolescent_sexual_reproductive/en/assessed on 26.07.2015.
7. B. N. Joshi, S.L. Chauhan, U.M. Donde, V.H. Tryambake, N.S. Gaikwad, V. Bhadoria Reproductive Health Problems and Help Seeking Behavior Among Adolescents in Urban India, Indian J Pediatr 2006; 73 (6) : 509-513.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





