IJCRR - 7(18), September, 2015
Pages: 25-30
Date of Publication: 20-Sep-2015
Print Article
Download XML Download PDF
KNOWLEDGE, ATTITUDE AND PRACTICES OF PEOPLE TOWARDS MALARIA IN TRIBAL COMMUNITIES OF JAWHAR, MAHARASHTRA, INDIA
Author: Suhas Kadam, Ambadas Adhav, Balu Mote, Shrikant Kalaskar, Thirumugam M., Ravindra Kurbude, Sushil Patil
Category: Healthcare
Abstract:Background: Malaria continues to be one of the major public health concerns that India is facing since decades. Early identification and management of malaria prevents its complications and subsequent mortality due to it. Several studies across the globe showed that, misconception of malaria still exists and practices of controlling malaria have been unsatisfactory indicating further need of exploring the knowledge, attitude and practices of malaria among the people of high Annual Parasite Incidence (API) states, district and blocks. Aim: The aim of the study is to assess the levels of knowledge, attitude and practices for prevention of malaria in tribal of Jawhar, Maharashtra. Methodology: A cross sectional community based KAP sample survey was carried out with the help of structured questionnaire. Data was collected by face to face interview by using a structured questionnaire from 140 participants by Systematic Random Sampling. Results: The results show, 24 participants (17.1 %) have a low knowledge level and 94 (67.1%) obtained an average level and 22 (15.7 %) have high level of knowledge on components like symptoms, causes and transmission of malaria. 118 participants (84.3 %) have the average level score for attitude component. 88 (62.9 %) of the participants have an average level, while only 14 (10.0 %) found to have low level score on practices component while 38 (27.1 %) found high level practices score. Knowledge on etiology and symptoms of malaria is found to be optimum level, while knowledge regarding the complications and preventive methods were found low among the participants. Health care system is the major source of knowledge for the tribal community. Practices of sanitation and correct health seeking behavior were found to be optimum but the sampled tribal community were found to be not co-relating its importance of health as a whole.
Conclusion: Health education program directed towards community should be emphasized on a timely basis to improve the knowledge, attitude, and practice regarding malaria and its prevention in Tribal Communities of Jawhar. Capacity building among the government health workers on preventive part of malaria and complication management for malaria is the need of the hour time, as they are the major contact point for tribals.
Keywords: Knowledge, Attitude, Practices, Malaria, Tribal, Jawhar, Thane, Maharashtra, India
Full Text:
INTRODUCTION
India achieved growth in terms of economic development but on the contrary India is facing a challenge of ‘triple burden’ of diseases with 21.0% of world global burden of diseases. On one hand India is facing challenge of maternal and child health, communicable diseases (sometimes termed as “Diseases of Poverty”) while on the other hand Diabetes, Heart Diseases and Mental Health Diseases (sometimes termed as the “Diseases of Life Styles”). (1) The incidence of India accounted 58.0 % of cases in the South East Asia Region of World Health Organization (WHO). (2) The Lancet on 20 November 2010 reported 205000 malaria deaths per year in India before the age 70 years with cumulative probability of death 1.8%. The report also added that 90.0 % of deaths were occurred in rural area. In India the high risk fatality associated with the malaria were noted from Orissa, followed by Chhattisgarh, Jharkhand and Assam. (3)Rural and more specifically tribal parts of all the state is more affected as compared to the urban population. Annual Parasite Index (API) for the Maharashtra for year 2011 was 36 per 1000 person. Deaths associated with malaria were recorded as 200 (2010) and 118 (2011) deaths in Maharashtra.(National Vector Borne Disease Control Programme)According to the health status report of Government of Maharashtra 2010, the proportion of dangerous Plasmodium falciparum was 25.7% across the state. It was and is significantly higher in the tribal districts of Gadchiroli, Gondia and across the Vidarbha and North Maharashtra followed by the tribal of Thane (Western Maharashtra). (5) Knowledge is the important component in health seeking behavior. Ignorance, low awareness and not prioritizing health are some of the issues in early identification and prompt treatment of diseases. Studies focusing on knowledge, attitude and practices (KAP) showed that direct interaction with community plays an important role in circumventing malaria problem.(6,7)Researchers have included the direct or indirect measures of people’s knowledge of malaria in equations describing the risk of infection and suggest that health education would offer promise of influencing individuals to adopt better attitude and practices towards preventive measures.(8) A community profiling was done as a part of data collection among the medical practitioners of the Jawhar Block in which they reported malaria as a very prevalent illness in this community. This is complemented by the findings from the National Vector Borne Disease Control Programme (NVBDCP). To achieve the targets of reducing malaria prevalence and preventing malaria epidemic, it is imperative to have active community participation which in turn depends on people’s knowledge and attitude towards the disease. The major public health problems are the contaminated water supply which leads to the unhealthy surroundings paving was for vector breeding and other communicable diseases in these rural and tribal regions. In fact human behavior as a major contributing factor has been largely neglected in research all over the globe on vector borne diseases in part because of the long-standing separation of the behavioral disorder from the physical and biomedical disciplines. So this study was conceptualized to explore the levels of knowledge, attitude and practices towards malaria in tribal communities of Jawhar, Maharashtra, India.
Methodology:
A cross sectional community based KAP sample survey was carried out with the help of structured questionnaire. Multi stage sampling was used in this study. Sakur PHC was selected out of four PHCs of Jawhar block of Thane by Simple Random Sampling. Six villages under the Sakur PHC, Jawhar were then further selected by Simple Random Sampling. 20.0 % households from every village were selected by using Systematic Random Sampling to get desired sample of nearly 140 households. Every 5th household in the village was interviewed by administration of structured questionnaire. In case of unavailability of households, the next household was included in the study for data collection.
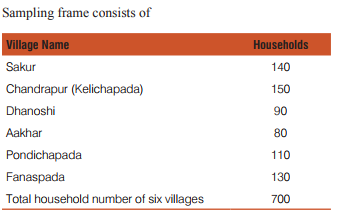
A total of 140 households (20.0 %) from these six villages were considered as samples in this study. Structured questionnaire was designed, pre-tested and standardized before the start of data collection.
Ethical Clearance: The permission from the institutional ethical committee was taken before starting the study. The purpose of the study was very carefully explained to study participants and informed consent was obtained. Confidentiality about the identity of the participant was maintained throughout the study. One individual per household (head of household) was interviewed face to face and responses were recorded in a structured close ended questionnaire. In case if head of the household was not present then other available member of the household of age > 15 years were interviewed. Gender equity during interview was considered throughout the data collection. Both sexes were given preferences for interview without any discrimination. Data was analyzed with the help of SPSS software version 20 package and Microsoft Office Excel. Descriptive statistics and cross tabs were carried out.
RESULTS
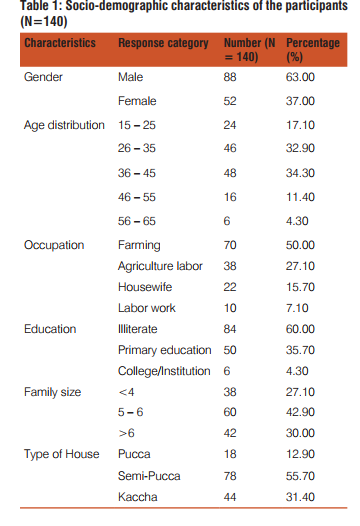
Findings from study are presented under the sections, sociodemographic profile, knowledge component, attitude component and practice component regarding malaria prevention. The table 1 indicates the socio-demographic characteristics of the participants. It was found that more than 50% of respondents were involved in farming and 27 % agricultural labour/ practices. Majority (68%) of the participants were in the age group of 26 to 45 years of age. Almost all (98%) of the population were found to be in with the education below primary level, of which illiterate were nearly 60%. Majority of the respondents were living in Semi-Pacca houses (56%) and Kaccha house (31%) with around 73 % of the families reported of having family size of 5 or more members. It was found that 63 % of respondent were male in this study.
Knowledge
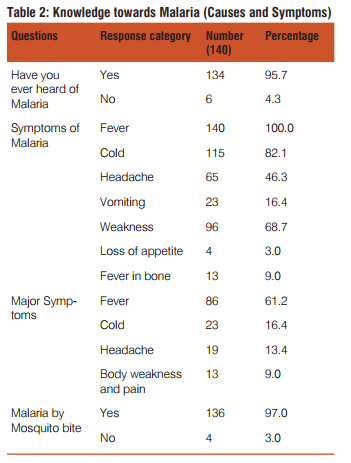
The majority sample correctly understood that malaria is transmitted by mosquitoes. Table 2 shows that 95.7 % of the population knows the correct cause of the malaria. As per the preventive perspective, community knowledge of malaria symptoms, such as fever accompanied by shivering, fever on alternating days, headaches, vomiting and rigors is very important for malarial control. Knowledge of the individual about the different symptoms described above is different for the different symptoms. Identification response was found 100% for fever and 83 % for feeling cold which are the basic symptoms for malaria. Among other symptoms only headache has been identified by the majority of the respondents and for the rest of the symptoms it was a low response. The knowledge level of individuals towards symptoms of malaria is low to average. Most of them could not identify other symptoms which are very important in the identification of fever related to malaria.
Attitude
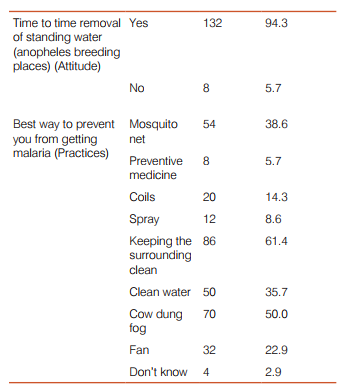
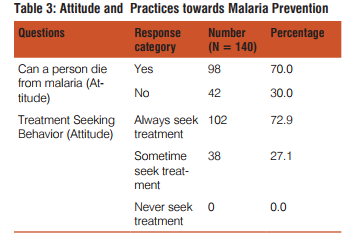
Table 3 indicates that of 30 % individuals perceived that malaria is a severe disease and person can die due to its serious consequences.73 % of the respondents reported to always seek care when they get these symptoms and remaining 27 % of the respondents reported to seek care only sometime, during the symptoms. About 95 percent of the participants reported removal of stagnant as a preventive measure for malaria.
Practices:
The percentage of population following important preventive practices to prevent malaria include, mosquito nets (39 %), indoor residual spraying (8 %), allowing the insecticidal fogging inside the house, cleaning the surroundings (62 %) as shown in table 3. In some practices, the percentage is very low, which is a cause of concern and should be addressed
KAP Scale scores: To assess the final level of knowledge, attitude, and practices we have developed a scale based on how many symptoms, attitude and practices the individual have and set the minimum (low) level of score, average level and maximum (high) level of score. (Table 4) This scale has been developed by adopting the KAP study of malaria in Myanmar. (9) The changes have been made according to the demand of the community setting. In the developed scale mean is about the scale only and not describing the mean of the score obtained. Mean is used only to divide the scale equally for the low, average, and high values. So according to these scale ratings the results for the total score for knowledge, attitude and practices have obtained.
One correct answer of respondent will get one mark. Score of each category again divided into three categories such as low, Average and high score viz. Knowledge and Practices score were low (1-3), Average (4-6) and high (7-9), while score for attitude was low (1-4) average (5-8) and high (9- 12), as the total questions for knowledge (9), attitude (12) and practices (9) were asked during the interviews of the participants.
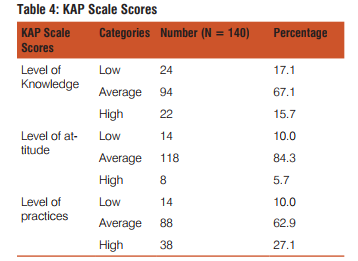
In the present study 67 % were found to be having an average knowledge on malaria 17.1 % have been found to have low knowledge level. Attitude was found at average level in 84 % of respondents and only 10 % reported low attitude levels. In the practices component, 63 % of the respondents were found to be of average level, while only 10 % found a low level score.
DISCUSSION
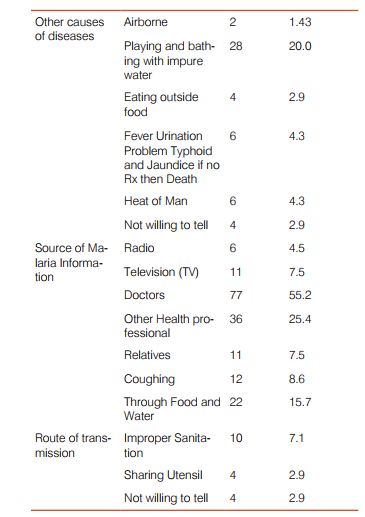
Health education is an important component in creating awareness and disseminating knowledge to the community. Slogans, IEC materials were available in Government of Maharashtra for increasing awareness of malaria health education in the community. The awareness regarding fever, cold, body ache and headache was found to be of optimal level from this study in tribal community of Jawhar indicating reach of Information Education and Communication (IEC) by the Government programme for prevention of communicable diseases under National Vector-Born Disease Control Programme (NVBDCP). Source of information of malaria mainly found as Government health care system and Doctors, this clearly depicts that Government is the major player of health care provision in the tribal areas. Tribals in Jawhar were found to be living in hilly and remote area where availability of infrastructures such as TV, radio etc. is less. Hence the tribal community is dependent mainly on Government healthcare system for the information, knowledge on disease transmission, prevention etc. Backwardness of tribal community as compared to other communities of rural and urban area is a known fact due to limited connectivity with external world like Television, Radio etc. Research regarding sanitation practices showed knowledge or awareness of sanitation helps indeed it is the good health seeking practices which are associated with the “odds” of communicable diseases. (10)Tribal people are aware or have the average knowledge of symptoms of malaria while they are not having high knowledge of prevention of malaria. This is an area which requires improvement as most of the respondents were found to be below the primary level of education. Further knowledge sharing on malaria through various health-education methods will help not only the tribal community to have strong healthy quality of life at the same time mortality due to malaria can be prevented. Though the respondents reported to be following good health seeking practices such as keeping surrounding clean, sanitation; indeed they fail to co-relate importance of these practices with their health status. So further upgrading their knowledge in area of sanitation, health hygiene and importance of behavioral change is needed. As knowledge and practices of the tribal people is a proxy indicator for the available social support or work done by the community health workers (CHWs) in area of health education, there is need of further capacity building among the health workers regarding the complications and treatment part of communicable diseases. (11) The respondent (more than 90%) had satisfactory knowledge regarding the aetiolgy, symptoms and treatment of malaria, majority of respondent (97%) understood that malaria is transmitted by mosquitoes. Studies that were conducted in other part of India in Rajasthan showed the same result and optimum knowledge of malaria in the community.(12)This could due to reach of IEC activities by Government or various organizations; also it could due to acquired knowledge from peers. Knowledge, attitude and practice study in India revels that there is discrepancy among the knowledge of Malaria associated with geography (hilly, tribal, urban, rural setting) and there is difference in different religions, because of their different health seeking behavior associated with their own cultural practices. (13) When we compared tribal community of Jawhar with other backward communities of tribal of India and Sub-Saharan countries then level of knowledge of Jawhar community is at average level.(14–17)
CONCLUSION
The knowledge level in the community was found to be average. Our findings suggest a need for a health education program aimed at the local community to increase knowledge level to high. Both attitude and practices were found to be average. Specific practices and attitudes changing trainings like use of mosquito nets, IRS spraying, standing water management through group discussion will help impart knowledge to curtail the spread of disease. An aware-ness programme about the common breeding sites (standing water) of Anopheles mosquitoes and ways to manage the complications is the need of an hour. This will improve attitude of the community to maintain their environment. It is recommended to conduct campaigns (IEC programs) for bringing in positive attitude towards Indoor insecticidal fogging in the community. Eventually, tribal of Jawhar needs health education on management of complications, prompt treatment and preventive part for control this communicable disease. Capacity building of the Community Health Workers (CHWs) is very much needed, as there were the main primary sources of knowledge and information dissemination at health care facilities.
ACKNOWLEDGMENTS
Authors duly thank School of Health System Studies, Tata Institute of Social Sciences, and Mumbai, India for providing the opportunity to conduct research and for permitting us to publish the contents of the research as an article in IJCRR and are also grateful to BAIF, Jawhar, and Maharashtra, India for field coordination. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of Funding: Nil
Conflict of interest: All author(s) declare(s) that there is no conflict of interest regarding the publication of this paper.
References:
1. Deaton A. The Great Escape: Health, Wealth, and the Origins of Inequality. 2013. 376 p.
2. World Health Organization. World Malaria Report. 2014. 228 p. 3. World Health Organization. Country Profiles. 2014.
4. National Vector Borne Disease Control Programme. Malaria in India [Internet]. Available from: http://www.malariasite.com/ malaria-india/
5. National Vector Borne Disease Control Programme. Annual Report [Internet]. 2012. Available from: http://www.nvbdcp.gov.in/ Doc/Annual-report-NVBDCP-2012.pdf
6. Ahorlu CK, Dunyo SK, Afari E a, Koram K a, Nkrumah FK. Malaria-related beliefs and behaviour in southern Ghana: implications for treatment, prevention and control. Trop Med Int Health. 1997;2(5):488–99.
7. Singh N, Singh MP, Saxena A, Sharma VP, Kalra NL. Knowledge, attitude, beliefs and practices (KABP) study related to malaria and intervention strategies in ethnic tribals of Mandla (Madhya Pradesh). Current Science. 1998.
8. Tyagi P, Roy A, Malhotra MS. Knowledge, awareness and practices towards malaria in communities of rural, semi-rural and bordering areas of east Delhi (India). J Vector Borne Dis. 2005;42(1):30–5.
9. Hla-Shein, Than-Tun-Sein, Soe-Soe, Tin-Aung, Ne-Win K-S-A. The level of knowledge, attitude and practice in relation to Malaria in O0-Do village, Myanmar. Southeast Asian J Trop Med Public Heal. 1998;29(3).
10. Sharma DC. India’s BJP Government and health: 1 year on. Lancet [Internet]. Elsevier Ltd; 2015;385(9982):2031–2. Available from: http://linkinghub.elsevier.com/retrieve/pii/ S0140673615609771
11. Perry HB, Zulliger R, Rogers MM. Community health workers in low-, middle-, and high-income countries: an overview of their history, recent evolution, and current effectiveness. Annu Rev Public Health [Internet]. 2014;35:399–421. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24387091
12. Yadav SP, Yadav S, Kuma P. Knowledge , treatment-seeking behaviour and socio-economic impact of malaria in the desert of Rajasthan, India. South African J Infect Dis [Internet]. 2013;28(1):41–7. Available from: http://www.sajei.co.za/index. php/SAJEI/article/view/399
13. Sharma AK, Bhasin S, Chaturvedi S. Predictors of knowledge about malaria in India. J Vector Borne Dis. 2007;44(3):189–97.
14. Forero D a, Chaparro PE, Vallejo AF, Benavides Y, Gutiérrez JB, Arévalo-Herrera M, et al. Knowledge, attitudes and practices of malaria in Colombia. Malar J [Internet]. 2014;13(1):165. Available from: http://www.malariajournal.com/content/13/1/165
15. Yadav SP, Tyagi BK, Ramnath T. Knowledge, attitude and practice towards malaria in rural communities of the epidemic-prone Thar Desert, Northwestern India. J Commun Dis. 1999;31(2):127–36.
16. Paulander J, Olsson H, Lemma H, Getachew A, San Sebastian M. Knowledge, attitudes and practice about malaria in rural Tigray, Ethiopia. Glob Health Action. 2009;2(1):1–7.
17. Aderaw Z, Gedefaw M. Knowledge, Attitude, and Practice of the Community towards Malaria Prevention and Control Options in Anti-Malaria Association Intervention Zones of Amahara National Regional State, Ethiopia. Glob J Med Res Dis. 2013;13(5).
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





