IJCRR - 14(4), February, 2022
Pages: 91-97
Date of Publication: 15-Feb-2022
Print Article
Download XML Download PDF
Assessing the Impact of Educational Interventions on Quality of Life: Measuring by Minnesota Living with Heart Failure Questionnaire
Author: Shaheen Nazakat, Kabir Ozigi Abdullahi, Asif Haneef, Adnan Yaqoob, Syed Amir Gillani, Muhammad Afzal, Umm-E-Habiba, Muhammad Sajid
Category: Healthcare
Abstract:Introduction: Heart failure is one of the most common cardiovascular diseases which decrease the quality of life. Most of the factors influencing the quality of life can be modified with educational interventions. Therefore, this study examined the impact of educational program on quality of life of congestive heart failure patients. Aims: The aim of the study was to access the impact of educational intervention on quality of life among congestive heart failure patients. Methodology: The study was conducted at Faisalabad Institute of Cardiology, Faisalabad Pakistan. Quasi-experimental design was used concerned study. The study participants were recruited through the process of convenient sampling. The sample consisted of men and women admitted to cardiac units, the researcher took data from patient's file for primary and secondary diagnosis of heart failure and was obtain consent from those participants, who fulfill the eligibility criteria. Results: The intervention showed significant (p
Keywords: Educational interventions, Heart Failure, Quality of Life, Minnesota living with heart failure, Impact, Questionnaire
Full Text:
Introduction
Heart failure is a prevalent cardiovascular condition that has a negative impact on one's quality of life. The heart is unable to properly pump enough blood throughout the body, resulting in a deficiency of blood flow supply throughout the body away from the heart.1 As a result, the oxygen delivery to human organs and tissues is insufficient.2 When heart failure strikes, the right ventricle frequently collapses as a result of the left ventricle's failing. The right ventricle, on the other hand, might sometimes fail on its own. Acute heart failure and chronic heart failure are the two types of heart failure. Acute heart failure manifests itself as the fast onset of symptoms and rapid worsening of heart failure symptoms.3
Heart failure has been one of the major clinical and economic burdens in the United States. On average, each patient's total annual medical costs amount to $6,199, with 95% of hospitalization costs.4 The high hospitalization and medical care costs have often prevented many patients from accessing high-quality medical care. As a result, most of them have succumbed to illnesses. While several patients have had insurance covers, many have had to spend their financial resources to cater to their medication.5
The educational program has played a pivotal role in improving the patient's knowledge about the disease process, self-care, and cost-effectiveness which in turn reduced the hospitalization stay of the patients.6 Moreover, this program has helped improve adherence to treatment. For instance, the improvement of self-care has promoted a healthy lifestyle among patients suffering from heart failure disease. Knowing the signs and symptoms of the disease, the process of treatments, and the appropriate actions required in the management of the disease has helped prevent the disease from worsening and hence reduce hospitalization stay for the patients. It is therefore essential for all healthcare directors to initiate such programs in their healthcare facilities to enhance disease awareness, self-care, and cost-effectiveness for the sake of patients suffering from heart failure.7
Quality of life explains the extent to which a person is comfortable, healthy, and in a position to enjoy or take part in life events. The concept of quality of life is seen as multifaceted in care delivery, incorporating social, material, physical and emotional well-being.8 The concept of quality of life can be explored in the case of congestive cardiac failure patients. There are various consequences of poor quality of life for congestive heart failure patients. Congestive heart failure (CHF) involves a chronic and progressive disorder that mainly affects the heart muscle pumping power in an individual. Whereas the condition is frequently known as heart failure, congestive heart failure includes the phase in which there is an accumulation of fluid inside the heart, resulting in inefficient pumping power.9
Hospital discharge education for patients with congestive heart failure (CHF) is important since it will help patients how to prevent future re-admission, improves self-care, and assists patients in determining problems early; hence it will increase the chances for improved patients results and adoption of best health interventions1.10 The Center for Medicare and Medicaid Service (CMS) reviewed how to reduce reimbursement by adding penalties for a patient with CHF (Congestive Heart Failure) for those who are re-admitted after hospital discharge within 30 days of their earlier heart failure admission. Re-admission of patients with CHF occurs due to inadequate planning discharge teaching from the patient's non-adherence to guidelines are illustrated as factor that lead to re-hospitalization, hence discharge teaching for patients with CHF is important since it improves the quality of life for patients and also improves patient outcomes.11
Multiple factors influence self-care behavior. To begin with, experience and skills become the first factor. The experience becomes an influential contributor to skill development in self-care. Therefore, patients must have sufficient knowledge and skills, to enable them to take the physician's advice to the latter.13 The study is necessary to ensure that more people acquire the appropriate knowledge needed to improve their general health. The importance of developing education programs is to ensure that there is adequate adherence to the medical recommendations during the treatment that eliminates any medical errors that may lead to ultimate readmissions.12 This way, the treatment of congestive heart failure is made more effective. When there is the presence of therapeutic interventions and educational sessions, it can lead to the improvement of a patient’s self-care, increase their awareness, and lead to positive health outcomes. When a patient lacks basic knowledge on their issues, it leads to low rates of compliance, and it is a great contributor to poor quality of life and readmissions in the hospital.14
The rationale of this study is to determine the effectiveness of educational programs in improving their quality of life through conducting a literature review on various articles related to educational programs and the quality of life of congestive heart failure patients. The general aim of the study is to throw light on the educational program on quality of life, whether the patient is faced with heart problems. According to the literature review many researchers conducted about the impact of educational programs on the quality of life of congestive heart failure patients. On each variable define separately, in many different countries and continents on different populations but no anyone try to find out collectively the above-mentioned variables among the married male and female patients with an educational program on quality of life. There is a very scarce research literature found with relevance to Pakistan. In the previous studies on the educational programs on quality of life in congestive heart failure patients, there was lack of a control group and sample size that does not permit the meaningful evaluation of the large numbers of variables that can influence the quality of life. In the previous studies of the relationship of educational program on quality of life of congestive heart failure patients with mortality different tools were used in each study caused a lack of correlation between mortality and all domains of educational program.
Objective:
So, the hypothesis generated are as follows:
H0 : The intervention has no significant effect on the quality of life in heart failure patients
Ha : The intervention has a significant effect on the quality of life in heart failure patients.
Significance of the Study
This study aims to provide a better understanding of the quality of life lived by HF patients and how educational programs can be used to improve the quality of life of such patients. The findings of this study will not only benefit the HF patients themselves by helping to improve their quality of life but will also benefit nurses and healthcare practitioners in general to improve the outcome of their patients. Further, this study will significantly help the educational program develops better programs that would enhance HF patients' life quality even better.
Operational Definitions
Independent Variable
Educational Program/ Discharge Teaching: A health education program is a planning and treatment process that will help the patient to enhance quality of life to reduce the re-hospitalization of heart failure patients.
Dependent Variable
A Quality of Life is the ability to perform physica1 and socia1 activities, maintaining happiness, and relationships. Quantity of 1ife wi11 be measured through MLHFQ.
MLHFQ Sca1e scores represent the average of 21 items in the sca1e that the respondent answered MLHFQ total scoring 0-105:
-
A score 0f 1ess than 24 (good qua1ity of 1ife),
-
A score 0f 24 t0 45 (average qua1ity of 1ife),
-
A score greater than 45 were determined as the cutting points for the (poor quality of 1ife) questionnaire.
-
Study Designs
This study used a quasi-experimental design concerned with quantitative statistics investigation and was explanatory in character. A quasi-experiment is a type of research design that attempts to establish a cause-and-effect relationship. The main difference with a true experiment is that the groups are not randomly assigned.
Setting
The study was conducted at the Faisalabad Institute of Cardiology, Faisalabad Pakistan.
Duration of Study
The duration of the study was 9 months after the approval of IRB.
Sampling Technique
A convenient sample was used in this study to collect data from the Faisalabad Institute of Cardiology (FIC).
Sample Size
The total calculated sample size is 36.
The calculated sample size is 1. This sample size is small to perform the statistical test with good efficiency. So, 30 participants will be taken after adding 20% dropout rate final. Sample size n=36
The sample size is calculated by using the following formula: -
.png)
Sample Selection
The study participants were recruited through the process of convenient sampling. The sample consisted of men and women admitted to cardiac units, the researcher took data from patient's file for primary and secondary diagnoses of heart failure and was obtain consent from those participants, who fulfill the eligibility criteria. The majority of patients in this sample were in NYHA classes II and III (New York Heart Association Classification) with scores of having an ejection fraction of less than 40 %.
Inclusion Criteria
The following inclusion criteria was followed for this study.
-
All heart failure patients admitted to the cardiac units with ECHO report indicating Congestive heart failure (CHF)
-
Both genders will be included equally.
-
Patients age 18 to 70 years old.
-
EF< 40 % and > 20%
-
Dyspnea
-
The patients were discharged to home and have cell phone/landline no.
-
Patients are able to give written or verbal consent for themselves.
Exclusion Criteria
The following exclusion criteria will be followed for this study.
-
Already taken any educational sessions or counseling regarding disease
-
Severe neuropsychiatric condition
-
Planned major surgery/intervention as a treatment of congestive heart failure.
-
Cerebrovascular accident, end-stage kidney disease, malignancy end stage
-
Patient with congenital heart disease
-
Bedridden
Data Collection Procedure
The data was collected after approval of the synopsis. The researcher checked the record for diagnosis of heart failure and eligibility. After receiving the verbal or written consent for enrollment, the researcher will contact the eligible patients. Before signing written informed consent, participants were briefed with a complete introduction to the research, its objective and its process. And researcher was also brief the risks and benefits and confidentiality of the data. The demographic data of the participants were collected through one-to-one interviews and medical records. MLHFQ was given to the respondents to fill out on the second day at hospital admission with the guidance of the researcher/facilitator. After taking the appointment from the participants, the researcher approached the patient at their bedside and educate the participants through a booklet which is an evidence-based comprehensive heart failure patient education booklet for four consecutive day for 15 mints. Booklet and Visual color-coded (Green, Yellow, and Red) guide for patients to monitor the symptoms at home according to the color zoon participants contacted the related nurse or Doctor.
-
Post-test 1 was conducted 30 days after completion of the intervention with a filling of questionnaires collected by the researcher/ facilitator on a one-month clinical follow-up visit.
-
Post test 2 was conducted at 90 days after intervention at each participant on a three-month follow-up visit.
Before the patient education, a one-hour training session for three consecutive days will be provided to facilitator/nurses in the cardiac units. The nurses' training sessions will be held over six days. Nurses will be asked to recapitulate the material in their own words and use the Robert Woods Johnson Foundation (RWJF) Live with Heart Failure guidance to facilitate comprehension and continuity.
An Instructional Guide for patients. Content for the standardized RWJF patient information materials for heart failure is based on the ACCF/AHA recommendations on nutrition, exercise, weight monitoring, avoidance of smoking, limiting of fluids, adherence to drugs, and follow-up appointments. The researcher will take advance permission from hospital administration for any adjustment regarding early patient visits or any investigation.
The researcher/ facilitator took the baseline data during hospital admission before discharge. The researcher will adjust the time participants to visit the hospital at the 30th day and the 90th day before discharge accordingly with the help of the hospital cardiologist.
Study Variables
Independent Variable: -The independent variable will be:
The Educational intervention/tech back technique is the independent variable.
Dependent Variable: -The dependent variable will be:
Quality of life will be measured by, MLHFQ
RESULTS
.png)
.png)
Table 1 shows the background detail of heart failure patients with regard to age, gender, qualification, work experience, and work setting. The sample consisted of 36 heart failure patients from the Faisalabad Institute of Cardiology. The findings of this study show that the majority 27.8% of participants are 61-65 years old. Also, a good majority 72.2% male participants and 55.6% of participants were literate. A huge majority 91.7% of participants are married. The participant's occupations were 44.4% employees, 47.2% unemployed and 8.3% retired. The BMI of the participants 22.3% were 31-39 category and 2nd highest fall four values 25, 27, 28 and 30 were 4 (11.1%). The total cholesterol of the participants 22.2% 300 cholesterol and 19.4% were 250 cholesterol. The Ejection friction status of the participants 13.3% 35 friction ejection and were 17 (19.4%), 30 were 7 (19.4%) and 40 were 5 (13.9%). The Classification NYHA status 72.2% were class and 19.4% NYHA class 2. The smoking status of the participant 61.1% were smokers and 38.9% were non-smoker. The residency status 50.0% were rural areas and 50.0% belong urban areas.
Distribution of respondents on the basis of cholesterol level:
The incidence of heart failure (HF) is constantly increasing in the Western world. Treatment with statins is well established for the primary and secondary prevention of cardiac events by lowering low-density lipoprotein (LDL) cholesterol levels. There are conflicting reports on the role of LDL cholesterol as an adverse prognostic predictor in patients with advanced HF. So the cholesterol level of respondents was measured.
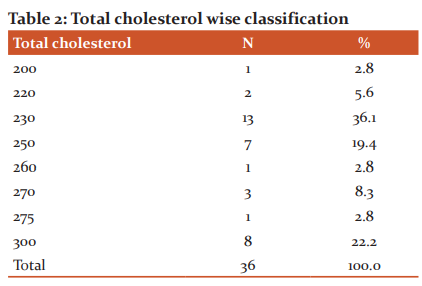
The total cholesterol of the participants 230 were 13(36.1%), 250 were (19.4%) and 300 were 8 (22.2%).
Ejection friction-wise distribution of the respondents:
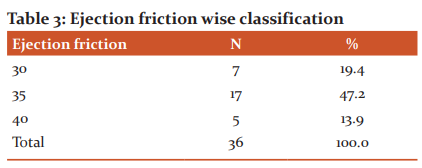
The Ejection friction wise classification of the participants depicted that 17 participants have 30 points Ejection friction, 7 participants having ejection friction of 30 points and least i-e 5 respondents have ejection friction up to 40 points.
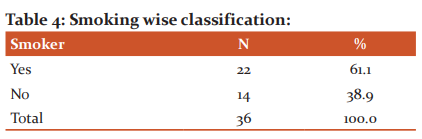
The smoking status of the participant were smoker 22 (61.1%) and non-smoker were 14 (38.9%).
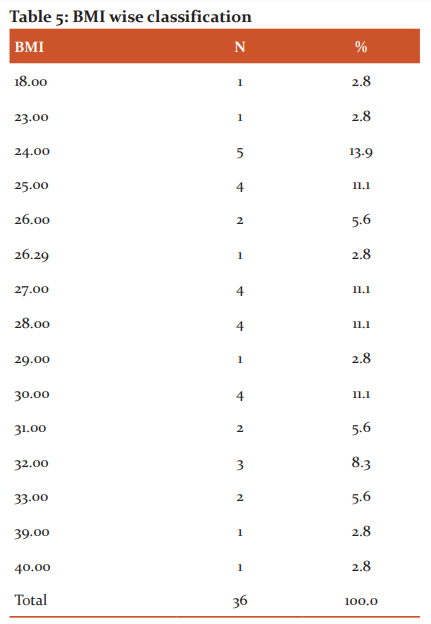
The BMI of the participants under 20 value were only 1 (2.8%), 24 value were maximum 5(13.9%), 2nd highest fall four values 25, 27, 28 and 30 were 4 (11.1%) and 31-39 category fall were 8 (22.3%).
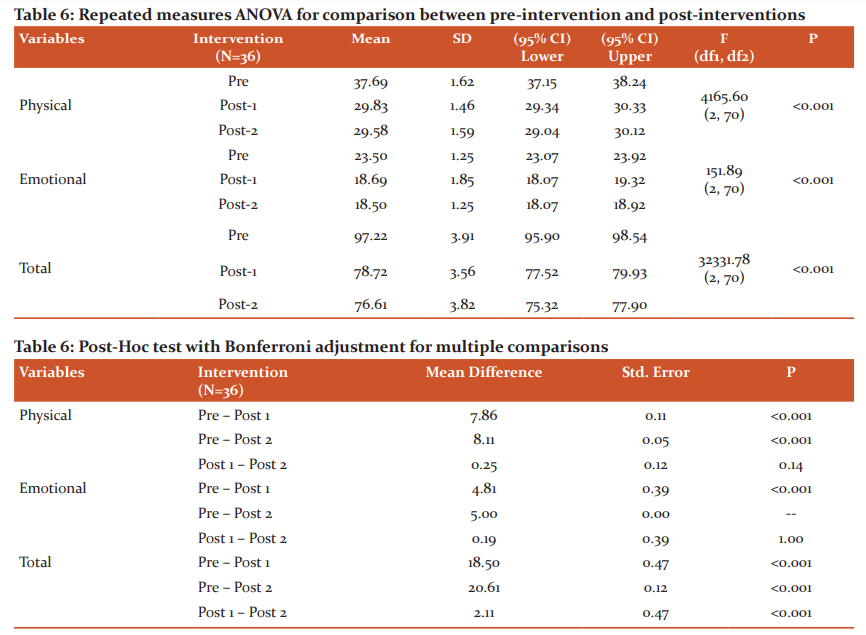
Physical: Based on the results of ANOVA (repeated measure analysis of variance), there was a significant difference found in Baseline Data, (M=37.69, SD=1.62). After 30 days’ educational intervention were found significant differences (M=29.58, SD=1.46) based on Teck Back techniques on quality of life in heart failure patients and After 90 days’ educational intervention were found significant differences (M=29.83, SD=1.59) based on Teck Back techniques on quality of life in heart failure patients.
Emotional: Further results show that there was a significant difference found between baseline Data and 30 days’ educational intervention (Mean Difference =4.81, Std. Error =0.39, P= <0.001). Results show that there was a significant difference found between baseline Data and after 90 days' of educational intervention (Mean Difference =5.00, Std. Error =0.00, P= <0.001).
Total: Results show that there was a non-significant difference found between 30 days' educational intervention and after 90 days' educational intervention (Mean Difference =0.19, Std. Error =0.39, P= 1.00).
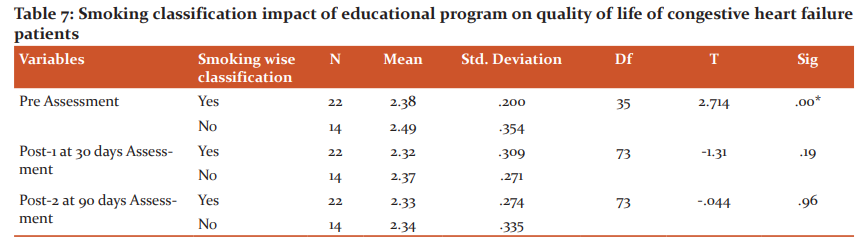
Clears that an independent sample t-test was applied to find out the mean comparisons in between the smoking responses on the impact of educational programs on the quality of life of congestive heart failure patients and the result shows that the smoker and nonsmoker patient mean scores. Therefore, it has been analyzed from the above pre-assessment results that mean for the response "yes” was M=2.38, (SD=.200) and responses in “No” was having mean M=2.49 and SD=.354. The result further shows that the pre-assessment p-value shows that, the impact of educational programs on the quality of life of congestive heart failure is relatively high in smoker patients than nonsmoker.
Post-1 at 30 days assessment Class2 were (M=2.32), (SD=.309) and Class3 (M=2.37), (SD=.271). Result further shows that the Post-1 30 days assessment p-value shows that, impact of educational program on quality of life of congestive heart failure is relatively high in smoker patients than nonsmoker.
Post-2 at 90 days assessment depicted that “yes” response was drop having mean M=2.33and SD=.274 and response for “No” (M=2.34), (SD=.335). The result further shows that the post-2 90 days assessment p-value shows that, the impact of educational programs on the quality of life of congestive heart failure is relatively high in smoker patients than nonsmokers.
Conclusion:
Our study outcomes demonstrated the importance of persistent educational interventions in improving quality of life in heart failure patients. In these patients, ongoing education enhanced their physical and emotional elements of QOL, as well as their overall QOL. In order to consistently promote self-care practices, regulate symptoms, and prevent consequences, continual training programs are required when it comes to the influence of chronic diseases on social health. As a result, with the rising prevalence of heart failure, persistent regimens are required.
Acknowledgment:
This article was written from the data derived from MSN thesis of Shaheen Nazakat a student of Department of Allied Health Sciences (LSN), University of Lahore Punjab, Pakistan. Special thanks to Dr. Asif Haneef, Syed Raza Gillani, Mrs. Um-E-Habiba and Muhammad Sajif for their cooperation in data collection, editing and proof-reading of the paper.
Conflict of Interest:
NIL.
Source of Funding:
NIL.
Ethical Clearance Number:
IRB-UOL-FAHS/830-II/2021.
Contribution of Each Author:
References:
-
Rokia1, Ali, Hassan, Hazem, Kali, Fadi. Evaluation of the Efficacy of Injection Platelet-Rich fibrin (I-PRF) in Accelerate Alignment and Levelling in an Adult Sample, IJCRR, 2021; Vol 13, Issue 23, Page no. 1-7.
-
Ponikowski, P,. Heart failure: preventing disease and death worldwide. ESC Heart Failure, 2014; 1(1), 4-25.
-
Mebazaa, A., Acute heart failure and cardiogenic shock: multidisciplinary practical guidance. Intensive care medicine, 2016; 42(2), 147-163.
-
Kim, E., Medical costs in patients with heart failure after acute heart failure events: a one-year follow-up study. J. Med. Econ, 2018; 21(3), 288-293.
-
Owenga, J. A, Nyambedha, E. O. Perception of cervical cancer patients on their financial challenges in Western Kenya. BMC Health Services Research, 2018; 18(1), 1-8.
-
Loving an, S. F., M. A cost-effectiveness analysis of a multimedia learning education program for stoma patients. J. Clin. Nurs, 2010; 19(13?14), 1844-1854.
-
Clari, M., Matarese, M., Ivziku, D., De Marinis, M. G. Self-care of people with chronic obstructive pulmonary disease: A meta-synthesis. The Patient-Centered Outcomes Research, 2017; 10(4), 407-427.
-
Arieh, A., Casas, F., Frønes, I., Korbin, J. E. Multifaceted concept of child well-being. Handbook of child well-being, 2014; 1, 1-27.
-
Katz, A. M., Konstam, M. A. Heart failure: pathophysiology, molecular biology, and clinical management. 2012; Lippincott Williams & Wilkins.
-
Adams, R. J. Improving health outcomes with better patient understanding and education. Risk management and healthcare policy, 2010; 3, 61.
-
Suksatan, W., Tankumpuan, T. Depression and rehospitalization in patients with heart failure after discharge from hospital to home: an integrative review. Home Health Care Management & Practice, 2021; 10(4), 27-47.
-
Awoke, M. S., Baptiste, D. L., Davidson, P., Roberts, A., Dennison-Himmelfarb, C. A quasi-experimental study examining a nurse-led education program to improve knowledge, self-care, and reduce readmission for individuals with heart failure. Contemporary nurse, 2019; 55(1), 15-26.
-
Hartgerink, J. M., Cramm, J. M., Bakker, T. J., Mackenbach, J. P., Nieboer, A. P. The importance of older patients’ experiences with care delivery for their quality of life after hospitalization. BMC Health Services Research, 2015; 15(1), 1-7.
-
Agrawal RK, Noor, Sofia, A Cross-Sectional Study on Violence Against Doctors and Associated Risk Factors in Raigarh, Chhattisgarh. IJCRR, 2021; 13(23). 32-36.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





