Introduction: Preterm infants (born with a low birth weight) represent major social and economic public health problems in developing/developed nations. The World Health Organization (W.H.O.) has suggested that gestational age <37 weeks and babies weighing <2500gm is considered preterm low birth weight and it leads to higher infancy sickness and neonatal mortality rates.1,2 The risk factors for PLBW include older (> 34 years) and younger (<17 years) maternal age; African-American ancestry; low socioeconomic status; inadequate prenatal care; drug, alcohol and tobacco abuse; hypertension; genitourinary tract infection; diabetes mellitus; multiple pregnancies and smoking.3
Some adverse pregnancy outcomes are thought to be associated with subclinical infections including periodontitis. Interventional studies of Lopezet al. in 2002,4 concluded that periodontal treatment reduces significantly the incidence of LBW (low birth weight) in women with periodontitis, whereas Michalowiczet al.,5 found no statistically significant difference and periodontal treatment did not significantly alter the rates of PB. Offenbacher et al. showed significant differences and they concluded that periodontal treatment reduces the incidence of PB.6,7
Animal studies have supported the hypothesis of a significant relationship between an increase in serum PGE2 induced by experimental Porphyromonasgingivalis and Escherichia coli infections in pregnant hamsters resulting in growth deficit and fetal mortality.8 Many instances of histologically proven chorioamnionitis are not linked with ongoing genitourinary tract infection, and culture findings are negative, suggesting that local infection is not the exclusive source of this disease.9,10 Hematogenous spread of infection from the oral cavity to amniotic fluid was suggested by Hill.11 Placenta is the only source of nutrition from the mother to the fetus, but can also act as the source of infection in the same way.
Using immunocytochemistry, the presence of Porphyromonasgingivalis antigens in placental tissues can be detected.12 The biological effects of P. Gingivalis on intrauterine tissues remain unclear. It can be detected in chorionic tissues of hospitalized high-risk pregnant women and may induce interleukin-6 and interleukin-8 production via TLR-2 in chorion-derived cells causing preterm rupture of the membrane.13
Patients with preterm delivery and generalized periodontal disease had a higher frequency of chorioamnionitis and funisitis.14 Although some recent studies failed to demonstrate an association,15 other reports—including animal, and human epidemiological and interventional studies—have suggested that poor periodontal status may result in preterm delivery and low birthweight.16 The presence of periodontal pathogens in placenta/placental extract has never been elucidated. So the purpose of the present study was to evaluate the possible correlation between microorganisms present in the placental extract and subgingival plaque and calculus, with the pregnancy outcomes.
Material and Method: The study included 30 pregnant females (15 each in study and control group), aged 18 -35 years who had given birth at Surendera Dental College and Hospital, Sriganganagar, Rajasthan, India, between May 2018 and December 2019. The consent form was signed by all the participants. The study group included women who had delivered preterm low birth weight babies (pregnancy< 37 weeks and weight < 2500gm), and females who had delivered at normal term and normal-weight babies were included in the control group. The study was approved by the ethical committee of the Institute of Dental Sciences, Bareilly, Uttar Pradesh, India.
Inclusion Criteria: All women who had ≥20 teeth; had periodontitis defined as the presence of at least 4 teeth with probing depth ≥4mm and clinical attachment loss ≥ 2mm, and had bleeding on probing at ≥35% of tooth sites, were included in the study group. And women with healthy periodontium were included in the control group.
Exclusion criteria: Patients having severe infection of the genital or urinary system (including bacterial vaginosis), pre-eclampsia, prophylactic antibiotics for invasive procedures, obstetric abnormalities (including placenta previa, hydramnios, gestosis or deformities of the uterus), systemic problems such as diabetes, hypertension and hypothyroidism, history of smoking, drinking and other tobacco-related habit and history of drug abuse were excluded from the study.
Clinical examination: Within two days postpartum, detailed medical history was taken with the help of a preformed questionnaire. A full mouth periodontal examination was carried out for every subject and the data was recorded for no of teeth present, bleeding on probing, probing depth and clinical attachment loss by a William graduated probe at four sites per tooth according to WHO Oral health surveys; 2013.17
Placental extract samples: Placental extract samples were collected at the time of delivery by the Obstetrician performing the procedure. Samples were transferred into the vial containing transport media (Robertson’s cooked meat broth) and stored at 4?C before transferring to the laboratory for processing.18
Plaque and calculus sample: In each subject, 2 periodontal sites with the deepest periodontal pockets were selected for microbial sampling. The supragingival plaque was removed and the sample sites were isolated from saliva. All the samples were obtained employing sterile Gracey curettes. The curette was inserted into the pocket and subgingival plaque and calculus were collected by a single scaling stroke. The collected plaque and calculus mass was immediately transferred into vials with transport media (Robertson’s cooked meat broth). All samples were thereafter transported to the laboratory of the division of Microbiology and kept at 4?C. Routine anaerobic bacteriological cultures were studied from placental extract & periodontal plaque and calculus samples. Processing was completed within 4 weeks from sample collection.19
Statistical analysis: The descriptive and inferential analysis of the data was done by using IBM SPSS. Statistics Windows, Version 20.0. (Armonk, NY: IBM Corp). The Chi-square test was used for intergroup comparison. Spearman Rank Correlation test was used for seeing the correlation between plaque and placental microbial count.
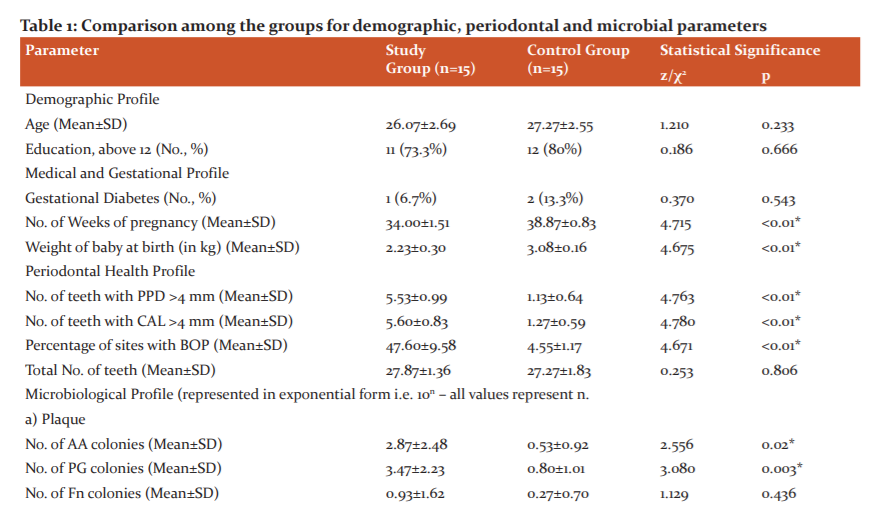
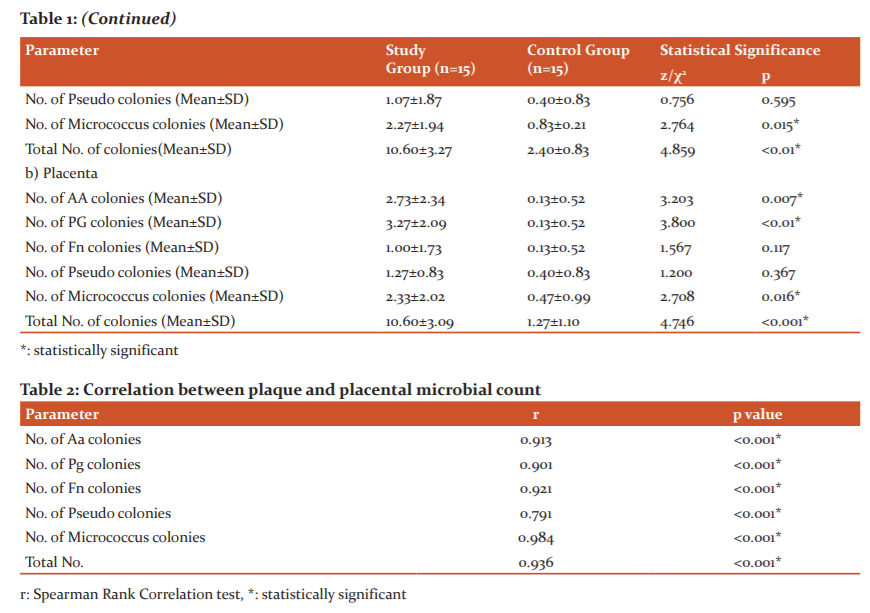
Results: Table 1 shows the comparison among the groups for demographic, periodontal and microbial parameters. By applying the chi-square test no significant difference was found between age and the total no. of teeth between study and control groups (p<0.05). A significant difference was found between no. of weeks of pregnancy, the weight of baby at birth, no. of teeth with probing depth (PD) ≥4mm, no. of teeth with clinical attachment loss (CAL) ≥4mm, percentage (%) of sites with bleeding on probing (BOP), between study and control groups. In microbiological profiles a significant difference was present between study and control groups for no. of A. actinomycetecomitans(Aa), P. gingivalis (Pg) and micrococcus colonies in both plaque and placenta samples. A significant difference was also present between study and control groups for the total no. of colonies in plaque and placenta samples. Some of the placenta extract samples were found to be sterile in the control group.
In table 2 reveals the Correlation between plaque and placental microbial count. Plaque and placenta microbial count were found to be correlated for all 5 groups of microorganisms (p<0.01).So, results of our study clearly indicate that in the study group females, Aa, Pg and micrococcus have a high count in both plaque and placenta samples, which were not seen in the control group.
Discussion: Placenta is the only source of nutrition to the fetus but at the same time can also act as a source of infection. In this study, we examined the correlation between plaque and placental microorganisms as related to pregnancy outcomes. In this study, all the confounding factors which may be responsible for preterm low birth weight babies were ruled out with detailed medical and personal history taken with help of a performed questionnaire.
A significant difference was found for probing depth, clinical attachment loss and bleeding on probing between case and control group, showing that case group females had periodontitis, while the control group had healthy periodontium. Maternal age, the total number of teeth, education level and gestational diabetes status were controlled factors. The above results were in comparison with the Moreu G et al.20
A significant difference was present between the number of colony-forming units per millimetre in preterm and term groups in plaque and placental samples. P. gingivalis, A. actinomycetecomitans and micrococcus were the most commonly encountered microorganisms in the case of the group for both plaque and placental extract samples. This shows that periodontal pathogens can affect the placenta and can later affect pregnancy outcomes. The spread of infection may have a hematogenous route from the oral site to the placenta, this has been supported by findings of Bearfield et al., who have found that bacteria from infected gums may spread to the uterus and fetus.21 Ebersole et al., found that women who delivered preterm had significantly lower antibody levels of P. gingivalis during the second trimester than women who delivered at term.22
Engebretson et al. in 2000 determined from a study of 164 women, mothers of preterm had significantly higher levels of periodontal pathogens. Furthermore, they suggested that periodontal treatment in pregnant women may substantially reduce the risk of having premature babies with LBW (low birth weight).23
Limitation of the present study was its small sample size, nutritional level, socioeconomic status, oral hygiene practices of patients not evaluated and the culture technique used because of the limited resources available. So, further studies with a large sample size and better microbiological analysis are required to draw a definite conclusion.
Conclusion: It can be concluded that a positive correlation was seen in our study between placental and plaque microorganisms in the preterm group (study group). This may be indicative of periodontitis being a potential causative factor for preterm low birth weight babies. Furthermore, studies are required with better microbiological analysis techniques and a larger sample size to validate the same.
-
World Health Organization. International Classification of Diseases. 1975 revision (1). Geneva: WHO, 1977.
-
World Health Organization. The incidence of low birth weight: an update. Weekly Epidemiol Rec 1984;59:205–211.
-
Committee to study the prevention of low birth weight, division of health promotion and disease prevention, institute of medicine. Preventing Low Birthweight. Washington, DC: National Academy Press: 1985.
-
Lopez NJ, Smith PC, Gutierrez J. Periodontal therapy may reduce the risk of preterm low birth weight in women with periodontal disease: A randomized controlled trial. J Periodontol. 2002;73:911–924.
-
Michalowicz BS, Hodges JS, Diangelis AJ, Lupo VR, Novak MJ, Ferguson JE, et al. Treatment of periodontal disease and the risk of preterm birth. N Engl J Med. 2006;355:1885–1894.
-
Offenbacher S, Lin D, Strauss R, McKaig R, Irving J, Barros SP, et al. Effects of periodontal therapy during pregnancy on periodontal status, biologic parameters, and pregnancy outcomes: A pilot study. J Periodontol. 2006;77:2011–2024.
-
Offenbacher S, Jarad HL, ?Reilly PG. Potential pathogenic mechanisms of periodontitis associated pregnancy complications. Ann Periodontol 1998;3:233.
-
Collins JG, Smith MA, Arnold RR, Offenbacher S. Effects of Escherichia coli and Porphyromonas gingivalis lipopolysaccharide on pregnancy outcomes in the golden hamster. Infect Immun 1994;62:4652-4655.
-
Hillier SL, Martius J, Krohn M, Kiviat N, Holmes KK, Eschenbach DA. A case-control study of chorioamnionitis infection and histologic chorioamnionitis in prematurity. N Engl J Med 1988; 319:972-978.
-
Mueller-Heubach E, Rubinstein DN, Schwarz SS. Histologic chorioamnionitis and preterm delivery in different patient populations. Obstet Gynecol1990; 75:622-626.
-
Hill GB. Preterm birth: association with genital and possibly oral microflora. Ann Periodontol 1998;3:222-232.
-
Katz J, Chegini N, Shiverick KT, Lamont RJ. Localization of P. gingivalis in Preterm Delivery Placenta. J Dent Res. 2009; 88: 575–578.
-
Nakamura K H, Tateishi F, Nakamura T, Nakajima Y, Kawamata K, Douchi T, et al. The possible mechanism of preterm birth associated with periodontopathic Porphyromonas gingivalis. J Periodontal Res. 2011;46:497-504.
-
Ovalle A, Gamonal J, Martínez MA, Silva N, Kakarieka E, Fuentes A, et al. Relationship between periodontal diseases and ascending bacterial infection with preterm delivery. Rev Med Chil. 2009;137:504-514.
-
Michalowicz BS, Hodges JS, DiAngelis AJ, Lupo VR, Novak MJ, Ferguson JE, et al. Treatment of periodontal disease and the risk of preterm birth. N Engl J Med 2006;355:1885-1894.
-
Goldenberg RL, Culhane JF, Iams JD, Romero R. Epidemiology and causes of preterm birth. Lancet 2008;371:75-84.
-
World Health Organization. Oral health surveys: basic methods. World Health Organization; 2013.
-
Burton GJ, Sebire NJ, Myatt L, Tannetta D, Wang YL, Sadovsky Y, et al. Optimising sample collection for placental research. Placenta. 2014;35(1):9-22.
-
Moolya NN, Thakur S, Ravindra S, Setty SB, Kulkarni R, Hallikeri K. Viability of bacteria in dental calculus–A microbiological study. J Indian Soc Periodontol 2010;14(4):222.
-
Moreu G, Téllez L, González-Jaranay M. Relationship between maternal periodontal disease and low-birth-weight pre-term infants. J ClinPeriodontol. 2005;32:622-627.
-
Bearfield C, Davenport ES, Sivapathasundaram V. Possible association between amniotic fluid microorganism infection and microflora in the mouth. Brit J Ob Gyn 2002;109:527-533.
-
Ebersole JL, Novak MJ, Michalowicz BS. Systemic immune responses in pregnancy and periodontitis: relationship to pregnancy outcomes in the obstetrics and periodontal therapy (OPT) study. J Periodontol 2009;80:953-960.
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License