IJCRR - 13(20), October, 2021
Pages: 66-70
Date of Publication: 24-Oct-2021
Print Article
Download XML Download PDF
Effect of Lumbar Stabilisation Exercises using the Stable and Unstable Surface on Pain, Disability and Electromyography (EMG) Activity in Chronic Low Back Pain
Author: Sheema Saleem, Moazzam Hussain Khan
Category: Healthcare
Abstract:Introduction: Non-specific low back pain is one of the common representations of musculoskeletal disorders which can be widely seen all over the world. It is mainly due to the unbalanced and weak muscles of the core, which plays a vital role in maintaining stability and mobility of the spine. Consequently causes recurrence of back pain with activities. The objective of the study: The study was done to evaluate the effects of lumbar stabilisation exercise using stable and unstable surfaces on pain, disability and electromyographic activity of the Erector spine and transverse abdomen are muscle in chronic low back pain patients (CLBP). Methods: Twenty-four patients with chronic low back pain were recruited in the study based on inclusion and exclusion criteria. They were randomly allocated into two groups i.e Group A (n=12) lumbar stabilization exercise (LSE) on a stable surface while Group B (n=12) LSE on an unstable surface for 3 sessions per week for 6 weeks in both the groups. The pain was assessed using the Numerous Pain Rating Scale (NPRS), functional disability using Modified Oswestry Disability Index (MODI) Scale and Muscle recruitment pattern using Electromyography (EMG). Result: Six weeks of interventions showed significant improvement in pain, functional disability and muscle activity of core muscles in both groups (p < 0.05). While comparing both groups, there was a significant improvement in pain and muscle activity of the transverse abdominal muscle in Group B patients (p < 0.05). Conclusion: Lumbar stabilization exercises using Swiss balls as unstable surfaces is effective interventional therapy for the alleviation of chronic low back pain and improving the muscle recruitment pattern in patients.
Keywords: Chronic low back pain, Functional Disability, Lumbar Stabilization exercise, Swiss Ball, Erector Spinae muscle, Trans�verse Abdominis muscl
Full Text:
Introduction
Mechanical low back pain refers to pain caused by abnormal stress and strain on vertebral column muscles which can be due to poor posture, ill-designed ergonomics or incorrect bending and lifting motions. It is the common representative muscular disorder and consists of spinal instability which further can lead to malfunctioning neuromuscular control.1Chronic low back pain (CLBP) is normally continuous back pain lasting more than 3 months.2It is widely seen in 70-85% of the population with up to 80% of patients described at least one episode in their life.3According to the world health organization low back pain constituted 37% of all occupational hazards which occupy the first rank among all the diseases.4
To provide stability of the lumbar spine, core muscles strengthening and stabilization exercises are important, and Core muscles mainly consist of deep stabilizer muscles are transverse abdominis, multifidus, pelvic floor muscles etc and global muscles are erector spinae, rectus abdominis, latissimus dorsi etc.5 Core training emphasis strengthening and reconditioning of local and global muscles that work together to stabilize the spine.6 The local muscles are slow-twitch fibres while global muscles are torque-producing muscles. The inter-segmental local muscle groups provide stabilization and control over supine position with lower force production.7
The major problem is the weakness, lack of motor control and delayed speed of muscles contraction of deep trunk muscles such as multifidus and Transverse Abdominis muscles.8 Deep stabilizer muscles in chronic low back pain patients become weak and imbalanced leading to reduced proprioceptive sense which further leads to stability problems in the spine and recurrence of back pain.9Therefore to treat LPB, deep stabilizer muscles exercise is required to balance the muscle control and counteract muscle atrophy. Unstable training equipment, such as Swiss balls, tend to increase the difficulty of performing exercises using complete bodyweight and resistance using free weights.10 Exercises done using Swiss balls employ all body regions and extensively activities can be done in comparison with exercises done on fixed floors. Using balls for performing exercises therefore can enhance the ability of dynamic balance, stability and the flexibility of the spine and improve the sense of balance to prevent injuries.11So exercises were done on a stable and unstable surface to examine its effects and measures using NPRS scale, MODI scale and surface EMG of core muscles.
Recently a study was done to see the correlation between the effects of trunk stability and LBP It has been suggested that to stabilize the trunk, correlation of deep and superficial muscles are needed as they are directly attached to the spine and stabilization exercises helps in improving the function on of neuromuscular system and hence support as well protect the spine.12LSE also helps in maintaining the neutral position of the spine, which is best for unloading of the spine. But no study shows the effectiveness of LSE on stable and unstable surfaces and their impact on global and local core muscle activation patterns in CLBP.13
Therefore, the study aimed to determine effective treatment protocol for chronic low back patients by performing LSE on the stable or unstable surface and to find out which exercise is best for reduction of pain, improving the core muscles activities and decreasing the functioning disability in chronic low back pain.
Materials and methods
Design
Pre-test and post-test experimental design.
Participants and Procedure
A total of 24 male and female subjects having chronic non-specific low back pain were recruited based on inclusion and exclusion criteria. Participants were informed about the purpose, procedure and effects of the treatment before the experiment and written consent was taken from them. Ethical clearance was taken from Institutional Ethical Committee Jamia Millia Islamia.
Inclusion Criteria
Non-specific low back pain experienced at least from last 3 months, age 18- 45 years, NPRS score from 3 to 6, MODI score from 20% to 60% (minimal disability to moderate disability), able to attend the hospital for treatment over 6 weeks, Prone instability test positive, Extensor endurance test positive, Aberrant movement pattern present.10
Exclusion criteria
Patients who have infectious pathology or injury received surgical interventions for their back pain or were awaiting surgery, diagnosis of clinical depression or other specific psychiatric pathology, contradicted to do exercises.10
All the participants were advised to avoid any other treatment interventions and they were recruited for a 6-week training program.
Measures and Interventions
Demographic data of subjects age (2.1346±4.475), height (1.676±7.471.), weight (62.130±0.113) and BMI (21.922±0.610) were taken along with the pre-test outcome measures which include pain level, functional disability and EMG of transverse abdominis and erector spinae. To measure the pain, Numerical Pain Rating Scale (NPRS) was used with an 0-10 integral rating scale. Modified Oswestry Disability Index (MODI) was used to assess the functional disability in CLBP.14The coefficient of Cronbach’s alpha was 0.92 and test-retest correlation reliability was 0.93.10
Surface EMG of erector spinae and transverse abdominis were taken by attaching disposable bipolar electrodes with a diameter of 1 cm attached parallel to muscle fibres. Skin preparation was done before the experiment to reduce impedance. Muscle activity of Transverse Abdominis was recorded by attaching surface electrode 2 cm away from the anterior superior iliac spine anteromedially while the activation pattern of the Erector spinae was recorded by attaching electrodes at 3 cm apart from the spinous process at the lateral side.12Ground electrode was attached over the superior aspect of the iliac crest of the same side.15 Every second time of the isometric phase of each exercise the root mean square (RMS) of EMG amplitude was calculated and then mean RMS obtained from three Maximum Voluntary Contraction trials for each muscle was used to provide a basis for EMG amplitudes normalization of data obtained during the experimental exercises (%MVC). The static phase of the experimental exercise was analysed, using means of three trials. The root means square (RMS) for the 3 repetitions of TA and ES muscles were normalised using 100 (%MVC). 16
Treatments
Participants are randomly assigned into two groups by using computer randomization Group A (n=12) and Group B (n=12).In Group A patients performed Lumbar Stabilization exercises on a stable surface along with hot fomentation for 10 min while Group B received hot packs for 10 min along with lumbar stabilization exercises on an unstable surface i.e Swiss ball. Equilibrium is maintained for 10 sec with a break of 3 seconds between repetitions for 40 min a day. Exercise protocol for both the groups was Back Bridging Exercise, Prone on Elbow, Posterior Pelvic Tilt, Abdominal Crunches and abdominal hollowing. Patients were instructed to maintain the final position for 10 sec then return to the initial position.10
Before initiation of each exercise program patients were given detailed verbal commands and visual clues or illustrations of exercise to patients emphasizing the starting and ending position. The selection of appropriate Swiss balls was based on demographic data given earlier. Group B was advised that the hip region must be parallel to the floor and the patient knee must maintain an angle of 90° while sitting on the Swiss ball .17
while sitting on the Swiss ball .17
Duration of treatment: Both groups received treatment for 3 days a week × 6 weeks, 10 times/set, 3 sets .10
Data analysis
Data were assessed by SPSS version 17.0.Shapiro -Wilk test for the normality of the distribution scores. The demographic characteristic and the baseline criterion measure were compared between the two experimental groups at the study evaluated by an independent t-test. Then a paired t-test was applied to analyze the effect of intervention in two groups for the measures of pain (NPRS), functional disability (MODI) and muscle activation of TA and ES muscles using EMG.
Results
Patients Demographic
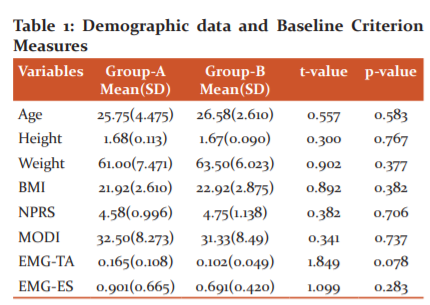
To prove the homogeneity between the two groups contrasting baseline criterion measurement was done using an independent t-test. No significant difference seen in baseline value of (p>0.05), Table 1
Analysis of data within groups
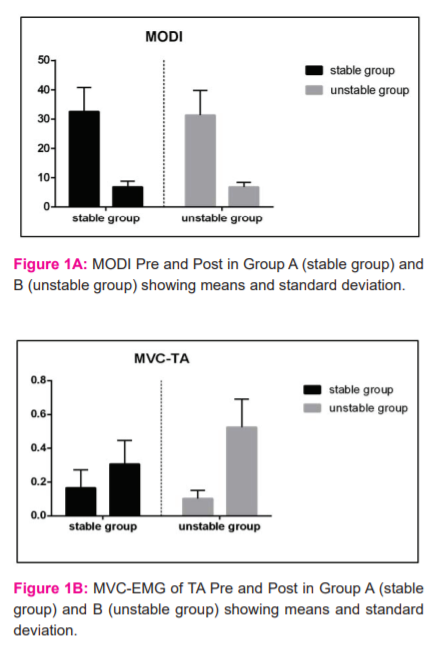
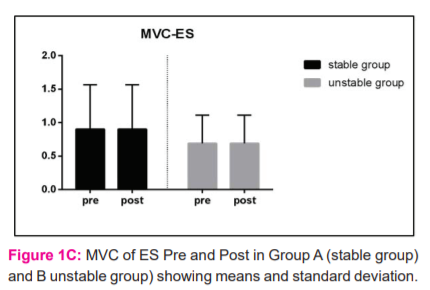
Paired t-test was used to distinguish the comparison between outcome variables at the baseline and Post-test measures in Group A and Group B. There was a significant difference in NPRS as pre mean of pain was 4.58(0.996) and post mean was 0.50(0.07)* in Group A and Group B pre mean was 4.75(1.138) and post mean was 0.00(0.00)*which shows the significant reduction of pain after 6 weeks of intervention. Similarly, there were significant reductions in MODI and EMG shown in figures 1A, 1B, 1C.
Analysis of data between the two groups
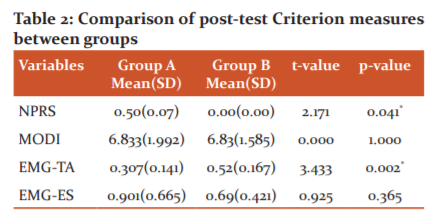
An independent t-test was used to compare post-test criterion measurement between Group-A and Group-B. A significant difference was seen between the groups in Pain (NPRS) and EMG activity of transverse abdominal muscle but there was no significant difference in Functional Disability (MODI) and EMG activity of Erector Spinae as shown in table 2. This reveals that lumbar stabilisation exercises done on Swiss balls were effective in decreasing chronic pain and increasing muscle activity patterns of local core muscles.
Discussion
Patients having non-specific mechanical low back pain show physical deconditioning of the core and manifests as muscle atrophy, decreased muscle strength and endurance. The localised and unilateral cross-sectional area of core muscles was also reduced in these patients. Active rehabilitation of trunk musculature reduced LBP symptoms, increased muscle strength, cross-sectional area and endurance.18In the current study pain was evaluated by NPRS scale so that subjective pain intensity of patients with CLBP before and after 6 weeks of training can be assessed. The reason for the reduction of pain was due to unbalanced core muscles training which leads to deep muscles activation and improves neuromuscular control. Yoon et al 2013, reported that stabilization exercises help in the reduction of pain by decreasing the signal delivered to the pain receptive tissues such as ligaments and joint capsules and further decrease the load on the lumbar vertebrae and enhance the function of the core stabilizer muscles leads to trunk positional control 16, a result which is similar with our study result. Lee et al., 2014, reported a significant reduction in pain in CLBP after training with Swiss Ball 12, a result that is consistent with our study. Along with that our result also showed that pain intensity significantly decreases Group B than Group A which was due to increased co-contraction pattern and activation in local core muscles.
In this study, the Lumbar stabilization exercise helped in increasing proprioception and co-contraction of core muscle which provide stability to the spine. Therefore emphasis should be on the stabilization exercises instead of strengthening of the muscle in low back patients.19Similarly trunk stabilizers muscles are more likely activated by unstable surfaces than stable which can be used in low back pain patients.20 There was a significant improvement in MODI in both groups after six weeks of intervention. But there was no significant difference between the two groups. A score less than 20% indicates that functional disability was not regarded as a significant functional disability in the daily life of patients .21
Muscle activity of local and global muscle was evaluated by EMG before and after six weeks of intervention and it has been seen that the MVC value of Transverse Abdominis and Erector Spinae significantly improves in both groups. The activity of transverse abdominis showed significant improvement in Group B as compared to another group, while there was no notable difference in MVIC value of Erector Spinae muscle. According to some research, good activation of the local muscles can lead to optimal stabilization of the lower back during basic stabilization exercise (O’Sullivan et al., 2000? Richardson et al., 2004).22,9,25 In the study (Escamilia et al.,2005) concluded that local muscles have a greater proprioceptive function and the exercise done on Swiss balls stresses these muscles to a greater extent which lead to improvement in balance.23,24Similarly deep abdominal muscle plays a very important role in providing spinal stability than superficial abdominal muscles. Despite the local muscles having short moment arms, which are deep and tonic muscles functioning as stabilizers of lumbar segments whereas superficial muscles are movement generating muscles that provide overall stability.2
Future studies can be done using resistance exercise using thera-band to provide resistance during LSE on both surfaces. An activity related EMG can be integrated comprising both the local and global muscle Limitations of the study where long term follow up can be taken to determine the reversibility of the result and the result cannot be generalized to the whole population.
Conclusion: The result of the study demonstrated that both stable and unstable surfaces significantly improved pain, functional disability and muscle activation pattern of the core muscles. Whereas, exercises performed on unstable surfaces are more effective as they help in achieving trunk stability and increasing the muscle activation pattern of transverse abdominal muscle to a great extent than the exercises done on a stable surface.
Acknowledgement:
We thank all the participants who helped with data collection, clinic staff, director of the centre of physiotherapy and authors whose articles are cited and included in references to this manuscript.
Conflict of interest: We have no conflict of interest.
Financial support: None
Author’s Contribution:
Sheema Saleem: Conceptualisation, data collection, data analysis, manuscript writing, manuscript modification.
Moazzam Hussain Khan: Conceptualisation, data analysis, manuscript modification, corresponding with the editor.
References:
-
Chung S, Lee J, Yoon J. Effects of stabilization exercise using a ball on multifidus cross-sectional area in patients with chronic low back pain.J. Sports Sci. Med. 2013 Sep; 12(3):533.
-
Panjabi MM. Clinical spinal instability and low back pain. J Electromyogr Kinesiol. 2003 Aug 1; 13(4):371-9.
-
Waddell G. Volvo award in clinical sciences. A new clinical model for the treatment of low-back pain. Spine. 1987 Sep 1; 12(7):632-44.
-
Manchikanti L. Epidemiology of low back pain. Pain physician. 2000 Apr 1;3(2):167-92.
-
Panjabi MM. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. J Spinal Disord .1992 Dec 1; 5:390-.
-
Dagenais S, Haldeman S. Evidence-based management of low back pain. Elsevier Health Sciences; 2011.
-
McGill SM, Grenier S, Kavcic N, Cholewicki J. Coordination of muscle activity to assure stability of the lumbar spine. J Electromyogr Kinesiol. 2003 Aug 1;13(4):353-9.
-
Akuthota V, Ferreiro A, Moore T, Fredericson M. Core stability exercise principles. Current sports medicine reports. 2008 Jan 1; 7(1):39-44.
-
Parveen A, Nuhmani S, Hussain ME, Khan MH. Effect of lumbar stabilization exercises and thoracic mobilization with strengthening exercises on pain level, thoracic kyphosis, and functional disability in chronic low back pain.J. Complement. Integr Med. 2020 Jul 27; 1(ahead-of-print).
-
Moon HJ, Choi KH, Kim DH, Kim HJ, Cho YK, Lee KH, et al. Effect of lumbar stabilization and dynamic lumbar strengthening exercises in patients with chronic low back pain. Ann Rehabil Med .2013 Feb; 37(1):110.
-
Escamilla RF, Lewis C, Bell D, Bramblet G, Daffron J, Lambert S, et al,. Core muscle activation during Swiss ball and traditional abdominal exercises. J Orthop Sports Phys Ther. 2010 May; 40(5):265-76.
-
Lee CW, Hwangbo K, Lee IS. The effects of combination patterns of proprioceptive neuromuscular facilitation and ball exercise on pain and muscle activity of chronic low back pain patients. J Phys Ther Sci. 2014; 26(1):93-6.
-
Behm DG, Drinkwater EJ, Willardson JM, Cowley PM. The role of instability rehabilitative resistance training for the core musculature. J Strength Cond. Res.2011 Jun 1; 33(3):72-81.
-
Fritz JM, Irrgang JJ. A comparison of a modified Oswestry low back pain disability questionnaire and the Quebec back pain disability scale. J. Phys. Ther.2001 Feb 1;81(2):776-88.
-
Souza GM, Baker LL, Powers CM. Electromyographic activity of selected trunk muscles during dynamic spine stabilization exercises. Archi Phys Medic Rehab. 2001 Nov 1; 82(11):1551-7.
-
Yoon JS, Lee JH, Kim JS. The effect of swiss ball stabilization exercise on pain and bone mineral density of patients with chronic low back pain. J Phys Ther Sci. 2013; 25(8):953-6.
-
Carrière B, Tanzberger R. The Swiss ball: theory, basic exercises and clinical application. Sprin Sci Busin Med. 1998.
-
Lehman GJ, Gordon T, Langley J, Pemrose P, Tregaskis S. Replacing a Swiss ball for an exercise bench causes variable changes in trunk muscle activity during upper limb strength exercises. Dyn Med .2005 Dec; 4(1):1-7.
-
França FR, Burke TN, Hanada ES, Marques AP. Segmental stabilization and muscular strengthening in chronic low back pain: a comparative study.Clinical Science. 2010, vol. 65, n. 10. ISSN. 1807; 5932:1013-7.
-
Sekendiz B, Cug M, Korkusuz F. Effects of Swiss-ball core strength training on strength, endurance, flexibility, and balance in sedentary women. J Strength Cond Res. 2010 Nov 1; 24(11):3032-40.
-
Karimzadeh, Farzaneh, Latafat Kar, Ghasemi, & Gholam Ali. The effect of 8 weeks of central stability training on pain and functional disability of mothers with low back pain in children with cerebral palsy. Scientific. Sci. J. Kurdistan Univ. Medical Sci. 2016; 21 (3): 34-44.
-
O'Sullivan PB, Phyty GD, Twomey LT, Allison GT. Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine. 1997 Dec 15; 22(24):2959-67.
-
Khan MH. How to deal with heterogeneity in people with low back pain? Saudi J. Sports Med. 2020 Jan 1;20(1):29.
-
Richardson CA, Snijders CJ, Hides JA, Damen L, Pas MS, Storm J. The relation between the transversus abdominis muscles, sacroiliac joint mechanics, and low back pain. Spine. 2002 Feb 15;27(4):399-405.
-
Ahmed N, Tufel S, Khan MH, Bhatnagar P. Errata: Effectiveness of neural mobilization in the management of sciatica. J Musculoskelet. Res. 2013 Dec 19;16(04):1392001.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





