IJCRR - 13(20), October, 2021
Pages: 12-19
Date of Publication: 24-Oct-2021
Print Article
Download XML Download PDF
Assessment of Renal Vasculature Variations, in Contrast, Computed Tomography Studies of 640 Patients at a Tertiary Care Centre in South India
Author: Karegowda H Lakshmikanth, Mathew Oshin, Raju Vinay, Pendem Saikiran, Priyanka, Ramprasad Bolar
Category: Healthcare
Abstract:Introduction: Renal vasculature is affected by a spectrum of variations that bears a high clinical impact while planning transplant surgeries/biopsies. Large scale Indian data is not available and a single study assessing these variations separately in male and female populations from a different country is available in the literature. Aims: To study the prevalence of renal artery(RA), renal vein(RV) variations, and investigate their gender distribution in patients undergoing contrast-enhanced computed-tomography(CECT) abdomen study. Materials and Methods: One-year prospective study, included 640 contiguous patients (320 males and 320 females) referred for the CECT study. Statistical Analysis: Descriptive analysis of different types of RA, RV variations, and analytical analysis of the association between these variations and association between gender and renal vascular variations(RVV)using the Chi-square test. Results: RA variations (376 patients -46.71%) predominated over the RV variations (131 patients -20.46%). Additional RA(AdRA) was the most common arterial variation (315 patients \? 49.21%), with occurrence in the female population dominating over the male population (52.81% and 45.62%% respectively, P>0.05). Accessory RA(AcRA) showed an increased prevalence over aberrant RA(AbRA) (29.37% and 19.68%, respectively). Unilateral AcRA and unilateral aortic-origin of AbRA(Ao-AbRA) showed female predominance; all bilateral Ao-AbRA and bilateral mixed origins (aortic and renal) of AbRA were seen exclusively in the female population (Eight patients and five patients, respectively). Among RV variations, the late confluence of RV(LcRV) was the most common variation (9.84%), with 60% being males and 40% females. No significant association between RA and RV variation(p>0.05) and between gender and vascular variations(p>0.05). Conclusion: Knowledge of RVV bears paramount importance in clinical practice, which helps radiologists/surgeons in better patient management.
Keywords: Renal artery, Renal vein, Variation, Aberrant renal artery, Accessory renal artery, Perihilar branching
Full Text:
Introduction
The vascular variation that is mandatory for the uro-surgeons to know beforehand is the variations in RA and RV, especially when the surgery is planned through laparoscopy or in cases of nephrectomy performed in donor1. Most studies on renal vascular variations in literature are retrospective in nature, with unequal sample sizes among each gender. Large scale Indian data is not available and a single study assessing these variations separately in male and female populations from a different country is available in the literature.2
The study's purpose was to assess the prevalence of renal vasculature variations in patients undergoing Contrast-Enhanced Computed Tomography, investigate their gender distribution, and find any association between them.
Materials and Methods
Study type, Sample size, and Ethics:
This is a prospective cross-sectional study performed in a tertiary care centre for a year. Institutional Ethical Committee approval was obtained (No: 304/2019), and 640 contiguous patients (320 males and 320 females) referred for CECT in whom both arterial and venous phases were acquired were analysed for RA and RV variations.
Inclusion and Exclusion criteria:
Inclusion criteria included all patients referred for CECT abdomen between the age range of 18 to 70 years. The exclusion criteria were the existence of renal pathology that destroyed the anatomy of renal vasculature, ectopic or ptotic location of kidneys, prior donor nephrectomy, and recipients of renal transplantation.
CT study protocol:
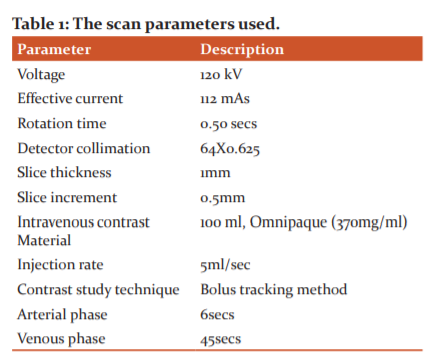
CECT was performed using 128-slice Philips Incisive CT with contrast injection administered through an 18-gauge cannula placed in the antecubital vein. The scan parameters were as mentioned in the table.1.
Definitions used for interpretation of variations:
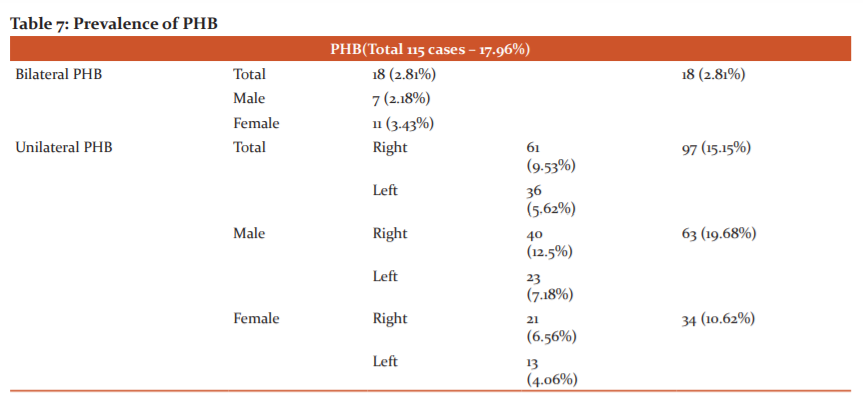
AdRA is the RA supplying the kidney apart from the main RA. AcRA is a type of AdRA that arise from the aorta and enters the kidney at the hilum. AbRA is another type of AdRA arising from the aorta or the main renal artery or any of the branches of the abdominal aorta but entering the kidney at its poles.3,4 Prehilar branching (PHB) of right RA is defined as retrocaval bifurcation or bifurcation within 1 cm of the right margin of inferior vena cava (IVC). PHB of the left RA is the bifurcation of left RA within 1.5 cms distal to its origin.5 PHB needs to be differentiated from Re-AbRA as both originate from the main renal artery. While the PHB enters the kidney at the hilum, the Re-AbRA enters the kidney at its pole.3,6(Figure 1)
RV variations included LcRV defined on the right side as the confluence of right RV within 1.5 cm from IVC and on the left side as the confluence of left RV within 1.5 cms from the aorta; multiple RVs (double or triple renal veins), circumaortic left RV (CaLRV) where left RV bifurcates and encases the aorta, retro aortic course of left RV (RaLRV) where the vein courses posterior to the aorta.5,7
Image interpretation:
The source images of both arterial and venous phases were analysed in multiplanar reconstruction (MPR), volume rendering (VR), and maximum intensity projection (MIP) images using Radiant DICOM viewer(V-19.2.3) by two experienced Radiologists having nine years and two years of experience and the interpretations were made by consensus.
The radiologists assessed RA parameters such as origin levels of main renal arteries, the total number of AdRA, AcRA, AbRA on either side, PHB on either side and the RV parameters such as the number of renal veins on either side, LcRV on either side, CaLRV and RaLRV.
Descriptive analysis of different types of RA, RV variations, and analytical analysis of the association between these variations and association between gender and renal vascular variations(RVV) using Chi-square test was performed. SPSS version 20 software was used for statistical analysis.
Observations and Results
A total of 640 patients (320 males and 320 females) were analysed. The mean age of the entire population was 42.2 (Males: 44.2 and Females: 40.5).
The overall prevalence of RA, RV variations:
Overall, the arterial variations (56.40%) dominated over the venous variations (20.46%). The male population showed higher incidences of both variations, as shown in table 2. The differences in the arterial and venous variations among the gender were not statistically significant (p>0.05).

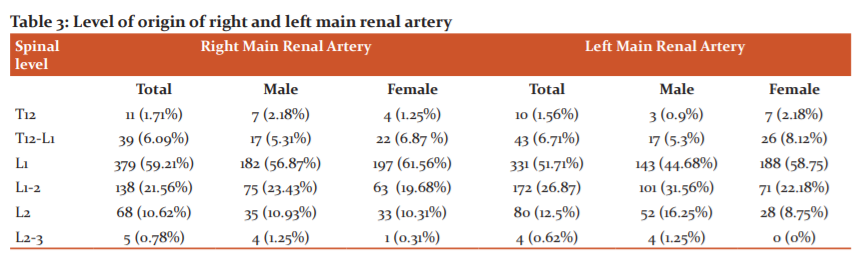
Level of origin of renal arteries:
Levels of origin of RA varied from T12 to L2-3 levels, out of which the most common level of origin was L1 level for both sides (59.21% on right and 51.71% on the left side). The next common level of origin was the L1-2 level. Both male and female populations conferred to the same trend, which is summarised in table 3.
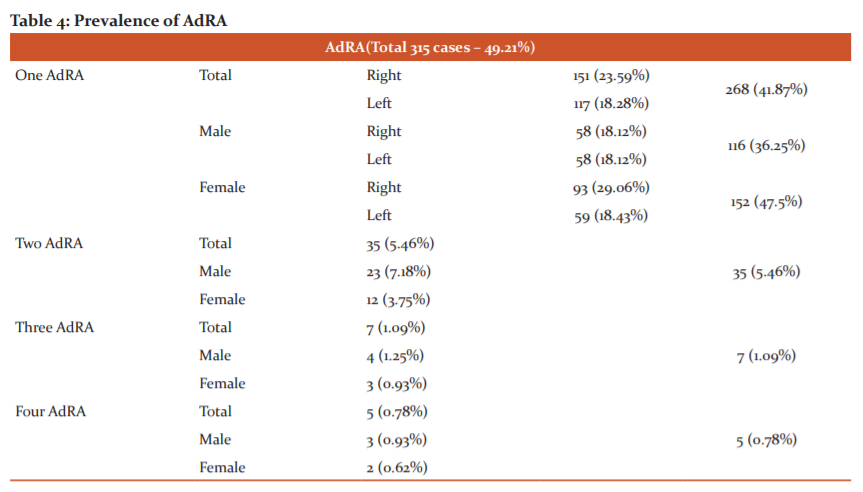
Prevalence of AdRA:
The count of AdRA (both AcRA and AdRA) was assessed as shown in table 4. The female population showed an increased prevalence of additional arteries as compared to the male population. A total of 315 cases showed single, double, triple and quadruple RA (Figure 2). More than 4 AdRA were not detected in any of the cases. Though the female population showed more tendency of having additional renal arteries (52.81% vs 45.62% in males), the difference was not statistically significant (p > 0.05).
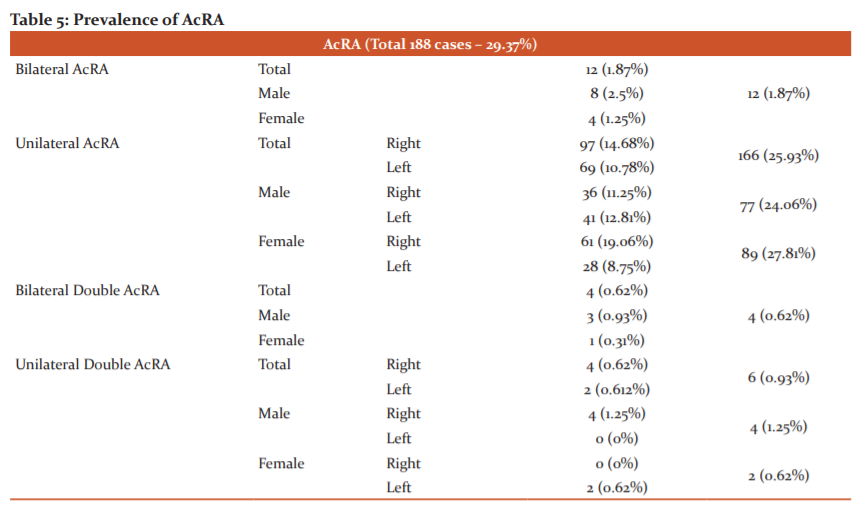
Prevalence of AcRA:
A total of 188 patients showed AcRA (29.37%). Prevalence of single unilateral AcRA was the most common variation in male (24.06%), female (27.81%), and total (25.93%%) populations. Right-sided variations were more common than the left side in all three groups as shown in Table 5. The female population showed an increased tendency of having unilateral AcRA (89 cases) as compared to the male population (77 cases), and the difference was not statistically significant (p>0.05). Single bilateral AcRA, double unilateral, and double bilateral AcRA were more prevalent among the male population.
Prevalence of AbRA:
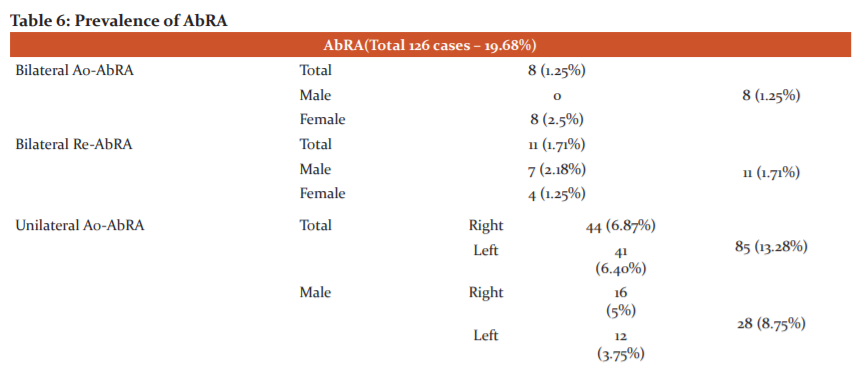
Though AbRA can arise from the abdominal aorta or any of its branches like a celiac trunk, superior mesenteric artery, inferior mesenteric artery, main renal arteries, or iliac arteries, only the AbRA arising from the aorta (Ao-AbRA) or main renal artery (Re-AbRA) were found in our study (Table 6). A total of 126 patients showed AbRA (19.68%).
The unilateral Ao-AbRA showed predominance (85 cases in total) over all other categories of AbRA, as shown in Table 4. All bilateral Ao-AbRA (Figure 3A) and mixed (aortic and renal) origins of bilateral AbRA was seen exclusively in the female population (8 patients -2.5% and 5 patients – 1.56%, respectively). While the prevalence of unilateral or bilateral Re-AbRA (Figure 3B) showed increased tendency in the male population (p>0.05), the prevalence of unilateral Ao-AbRA showed predominance in the female population (p=0.044). No case of unilateral or bilateral double AbRAs detected.
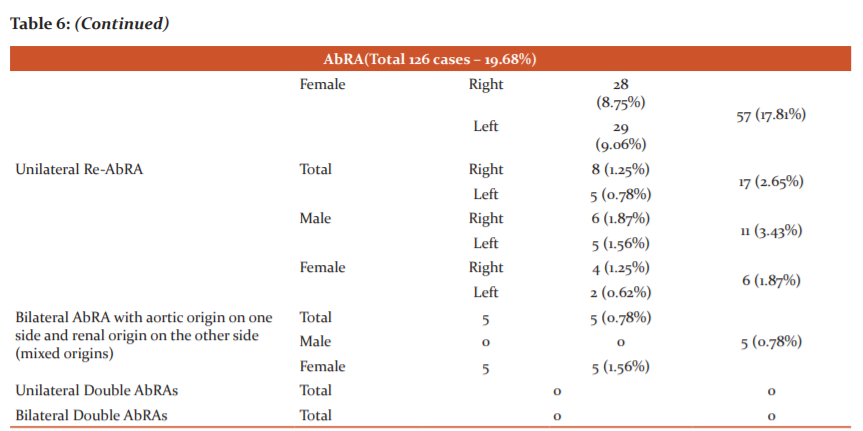
Prevalence of PHB:
Females showed a slightly higher prevalence of bilateral PHB (p>0.05), while males showed a higher prevalence of unilateral PHB (p>0.05). Right PHB had a higher prevalence than the left PHB in both males and females (p>0.05) (Table 7).
Prevalence of LcRV:
Among the venous variations, unilateral LcRV was the most common variation found (63 cases -9.84%) (Figure 4A), with the male population showing slightly increased prevalence (p>0.05) and occurrence more towards the right side (p>0.05). Bilateral LcRV had equal prevalence in both male and female populations.
Prevalence of Multiple RV:
No cases of bilateral multiple RV were detected. Unilateral double RV showed slight male predominance (p>0.05) and an increased prevalence on the right side (Figure 4B) in both male and female populations (p=0.00003) (Table 9). No case of unilateral/bilateral triple or quadruple renal veins was detected.
Prevalence of RaLRV and CaLRV:
CaLRV was seen in only 5 patients, with majority being the female population (Table 10) (Figure 4C). RaLRV was the most common variation in the left RV course, having a total prevalence of 6.71% with slight predominance in the male population (p>0.05) (Figure 4D).
Statistical Association between RA and RV variations:
The right-sided late confluence of RV with right AcRA showed the most frequent occurrence (19 cases- 2.96%). The Chi-square test, however, showed no significant association between the renal artery and renal vein variations in both males (p>0.05) and females (p>0.05).
Discussion
The definitive location of the “embryonal wandering” kidneys determines their permanent vascular supply implying an abnormal location would lead to an abnormal vascular supply.8,9 Hence, the ectopic or ptotic kidneys were excluded from our study.
The male population showed an increased overall tendency in RA and RV variations as compared to females (p>0.05). Our study and the study by Ozkan et al.10 found the most common level of origin for right RA to be L1 (59.21% and 43%, respectively). However, the latter study found that the left RA origin was slightly more common at L2 (38% vs. 37% at L1) though we found the L1 level to be most common for left RA origin (51.71%). Famurewa et al.11 reported that both right and left renal arteries broadly originated between the upper margin of L1 and lower margin of L2, which fits well with our study.
Satyapal KS et al.7 reported a wide range of variations in the prevalence of the AdRA across various studies ranging from 8.7% to 75.7%, with an average of 28.1%. Our study's prevalence was 45.62%, which is close to the studies by Macalister A et al.12 of 43% and Ugurel et al.13 of 42%. Among AdRA, single AdRA had the most common occurrence like other studies in the literature.7,13,14 The prevalence of single AdRA of 41.87% in our study is close to the prevalence of 37.7% found by Kher GA et al.14 Occurrence of single AdRA was more frequent on the right side, which is congruent with the studies by Holden et al.15 Ozkan et al.10 and Ugurel et al.13
We detected increased prevalences of the AcRA over AbRA of 29.37% and 19.68%, respectively. Khamanarong et al.16 found a higher prevalence of AbRA, and Cinar C et al.2 found a higher prevalence of AcRA like our study. Among the AbRA, we had a particular interest in studying the prevalence of Re-AbRA as we could not find any English literature addressing the same. This may be because most of these arteries could have been mislabelled as early (prehilar) division of the main renal artery. We strictly followed the distinctions between the two as defined in the introduction and found the overall prevalence of Re-AbRA to be 5.15%. Interestingly, bilateral Ao-AbRA and bilateral mixed origin AbRA were exclusively found in the female population.
For easier control of haemorrhage during transplant and for suitable anastomosis, incision of the renal artery should be at 1.5 to 2 cms from the aortic origin. Hence determining PHB is of paramount importance. The prevalence of it across the existing literature has a wide range between 4.3% and 26.7%.2,10,15,17,18,19 depending on the investigation method. Our study showed a total of 115 patients (17.96%) having PHB with unilaterality seen in 15.15% and bilaterality in 2.81%. Our rate of 17.96% falls within the rate interval seen across the literature for PHB.
RV variations, in general, do not form a contraindication for donor nephrectomy. However, to prevent inadvertent incisions of RV, there is a need to know the variations like RaLRV and CaLRV. Also, planning for RV catheterisation for renin sampling becomes easier if the variations are known beforehand. On similar lines, venous variations become important before placing an inferior vena cava filter.
Studies by Koc et al.20 Raman et al.21 and Cinar C et al.2 found the prevalence of multiple right RV of 14.3%, 24%, and 21.6%, respectively. In our study, multiple right RV was found in 5.78% of the total population and is lower than the other studies. Cinar C et al.2 found a total prevalence of LcRV of 7.3%, while we found its prevalence to be a little higher (9.84%). Concerning the variations in the course of the left renal vein, Raman et al.21 found 2% RaLRV and 8% CaLRV while Cinar et al.2 found 4.2% RaLRV and 5.2% CaLRV. Our prevalence rate of 6.71% RaLRV is higher, and 0.78% CaLRV is lower than those studies. These differences in various RV variations in our study compared to other studies could be due to racial differences.
Only a single study available in the present literature has investigated the gender association with renal artery variations2 They found no significant difference between the gender in terms of RA variation prevalences, though they found PHB more frequently in men. We too observed an increased prevalence of unilateral PHB in men, but the bilateral PHB was more prevalent in women. However, the differences in these arterial variations among the gender were not significant statistically (p>0.05). Our study's interesting findings include the exclusive occurrence of bilateral Ao-AbRA and bilateral mixed origin of AbRA in the female population.
All venous variations except the CaLRV showed a male predominance in our study. Cinar et al.2 also found men to have increased prevalence rates of multiple right RV and RaLRV like our study. However, unlike our study, they found that the CaLRV had an increased prevalence in the male population and LcRV had near equal prevalences in the men and female populations. However, the differences in these venous variations among the gender were not significant statistically, and the same was true in our study.
Limitations of the study include no comparison with the digital subtraction angiography which is still the gold standard for vascular assessment and the interobserver variation among the radiologists was not assessed.
Conclusion:
Knowledge and awareness of renal vessel variations are crucial for radiologists and surgeons, and CECT forms an excellent modality in their evaluation. AdRA was the most common arterial variation, and among the venous variations, the unilateral LcRV formed the most common variation, especially on the right side. Re-AbRA, which is seldom studied in the available literature, had a prevalence of 5.15%, and bilateral Ao-AbRA and bilateral mixed origin AbRA were exclusively seen in females. No statistically significant association between the gender and vascular variations was seen. Likewise, no significant association between RA and RV variations was detected.
Source(s) of support: Nil
Presentation at a meeting: Nil
Conflicting Interest (If present, give more details): Nil
Acknowledgment:
The authors would like to thank Dr Prakashini, HOD and Professor, Radiology Dept., KMC Manipal and Dr Rajagopal K V, Professor, Radiology Dept., KMC Manipal for constant support and encouragement during this study.
Authors Contribution:
1. Karegowda H Lakshmikanth – Principal Investigator
2. Mathew Oshin - lead Investigator
3. Raju Vinay - lead Investigator
4. Pendem Saikiran - lead Investigator
5. Priyanka – lead investigator
6. Ramprasad Bolar – statistics and methodology.
Figure 1: VR images which show the difference between PHB (early branching) and Re-AbRA. Note in image A, the branch of main renal artery (thin white arrow) enters the kidney through the hilum suggestive of PHB while in image B the branch from main renal artery (bold white arrow) is coursing to its pole suggestive of Re-AbRA.
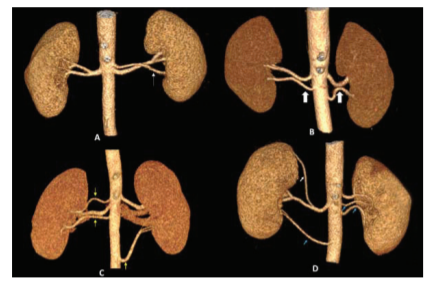
Figure 2: VR images showing, A – One AdRA represented by a left-sided AcRA (thin white arrow), B- Two AdRA represented by bilateral AcRA (bold white arrows), C- Three AdRA represented by two right-sided AcRA and one left-sided AcRA (thin yellow arrows) and D- Four AdRA represented by three AcRA (thin blue arrows) and one AbRA (thin white arrow)
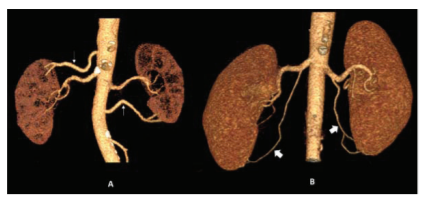
Figure 3: VR images showing, A- Bilateral Ao-AbRA (thin white arrows) and B- Bilateral Re-AbRA (bold white arrows)
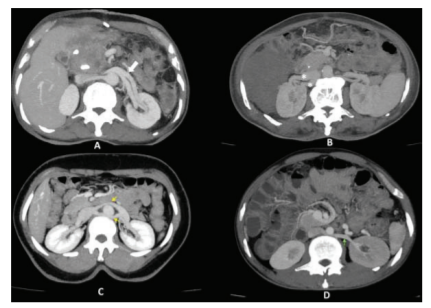
Figure 4: Axial MIP reconstructions during the venous phase of contrast study. A- shows left-sided LcRV (bold white arrow), B- shows double right renal vein (white asterisks), C- shows CaLRV (yellow arrows) and D- shows RaLRV (green arrow)
References:
-
Al-Katib S, Shetty M, Jafri SMA, Jafri SZH. Radiologic assessment of native renal vasculature: a multimodality review. Radiograph. 2017;37(1):136-56.
-
Çnar C, Türkvatan A. Prevalence of renal vascular variations: Evaluation with MDCT angiography. Diagnostic and interventional imaging. 2016;97(9):891-7.
-
Graves F. The aberrant renal artery. J Anat. 1956;90(4):553.
-
Rao TR. Aberrant renal arteries and its clinical significance: a case report. Int J Anat Var. 2011;4:37-9.
-
Sebastià C, Peri L, Salvador R, Buñesch L, Revuelta I, Alcaraz A, et al. Multidetector CT of living renal donors: lessons learned from surgeons. Radiograp. 2010;30(7):1875-90.
-
Kang W, Sung DJ, Park B, Kim MJ, Han NY, Cho SB, et al. Perihilar branching patterns of renal artery and extrarenal length of arterial branches and tumour-feeding arteries on multidetector CT angiography. Br J Radiol. 2013;86(1023):20120387.
-
Urban BA, Ratner LE, Fishman EK. Three-dimensional volume-rendered CT angiography of the renal arteries and veins: normal anatomy, variants, and clinical applications. Radiogr. 2001;21(2):373-86.
-
Satyapal KS, Haffejee AA, Singh B, Ramsaroop L, Robbs JV, Kalideen JM. Additional renal arteries: incidence and morphometry. Surg Radiol Anat. 2001;23(1):33-8.
-
Pohlman AG. Abnormalities in the form of the kidney and ureter dependent on the development of the renal bud. Johns Hopkins Med J. 1905;16:51.
-
Özkan U, Oguzkurt L, Tercan F, Kizilkilic O, Koç Z, Koca N. Renal artery origins and variations: angiographic evaluation of 855 consecutive patients. Diagnostic and interventional Radiology. 2006;12(4):183.
-
Famurewa O, Asaleye C, Ibitoye B, Ayoola O, Aderibigbe A, Badmus T. Variations of renal vascular anatomy in a Nigerian population: A computerised tomography study. Niger J Clin Pract. 2018;21(7):840-6.
-
MacalisterA. Multiple renal arteries. J Anat Physiol. 1883;17:250-2.
-
Ugurel M, Battal B, Bozlar U, Nural M, Tasar M, Ors F, et al. Anatomical variations of the hepatic arterial system, coeliac trunk and renal arteries: an analysis with multidetector CT angiography. Br J Radiol. 2010;83(992):661-7.
-
Kher GA BI, Makhani JS. Intrarenal branching of the renal artery. Ind J Surg. 1960;22:563-9
-
Holden A, Smith A, Dukes P, Pilmore H, Yasutomi M. Assessment of 100 live potential renal donors for laparoscopic nephrectomy with multi-detector row helical CT. Radiology. 2005;237(3):973-80.
-
Khamanarong K, Prachaney P, Utraravichien A, Tong?Un T, Sripaoraya K. Anatomy of renal arterial supply. Radiology. 2004;17(4):334-6.
-
Gümü? H, Bükte Y, Özdemir E, Çetinçakmak MG, Tekba? G, Ekici F, et al. Variations of renal artery in 820 patients using 64-detector CT-angiography. Renal Failure. 2012;34(3):286-90.
-
Kim J-K, Park S-Y, Kim H-j, Kim C-S, Ahn H-J, Ahn T-Y, et al. Living donor kidneys: usefulness of multidetector-row CT for comprehensive evaluation. Radiology. 2003;229(3):869-76.
-
Rydberg J, Kopecky KK, Tann M, Persohn SA, Leapman SB, Filo RS, et al. Evaluation of prospective living renal donors for laparoscopic nephrectomy with multisection CT: the marriage of minimally invasive imaging with minimally invasive surgery. Radiographics. 2001;21(suppl_1):S223-S36.
-
Koc Z, Ulusan S, Oguzkurt L, Tokmak N. Venous variants and anomalies on routine abdominal multi-detector row CT. Eur J Radiol. 2007;61(2):267-78.
-
Raman SS, Pojchamarnwiputh S, Muangsomboon K, Schulam PG, Gritsch HA, Lu DS. Surgically relevant normal and variant renal parenchymal and vascular anatomy in preoperative 16-MDCT evaluation of potential laparoscopic renal donors. JR Am J. Roentgenol. 2007;188(1):105-14.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





