IJCRR - 13(16), August, 2021
Pages: 159-163
Date of Publication: 30-Aug-2021
Print Article
Download XML Download PDF
Modified Sphygmomanometer as \"Biofeedback Tool\" in Retraining Quadriceps Function among Individuals with Unilateral Tibio-femoral Osteoarthritis - A Case Series
Author: Renuka K, Shristhudhi D, Sankarmani B, Seetharaman VS, Jagadevan M, Mohanakrishnan B, Prabakaran R
Category: Healthcare
Abstract:Introduction: Unilateral tibiofemoral osteoarthritis (OA) of the knee is the most common musculoskeletal impairment among the geriatric population and is associated with pain, quadriceps weakness, functional disability and progressive deformity. Quadriceps weakness is an early clinical finding which plays a major role in disease progression. Presently interventions are focused on pain relief and quadriceps reactivation on a subjective basis. Hence, physical therapists must succour these individuals at an early stage and objectively reactivate the quadriceps mechanism. This paper highlights the importance of visual biofeedback in the form of a \"modified sphygmomanometer\" in retraining quadriceps reactivation and retaining the functional status in individuals with unilateral tibiofemoral osteoarthritis. Objective: To provide an objective re-learning to regain quadriceps muscle strength in individuals with unilateral tibiofemoral osteoarthritis Methodology: It was a case series where 23 individuals in the age group of 35-65 years reporting to the orthopaedic outpatient department were recruited. 12 individuals who fulfilled the selection criteria were included in the study and were observed for 4 weeks. 2 individuals lost their follow up during treatment. After obtaining the oral and written consent basic demographic details, quadriceps isometric strength (Using modified sphygmomanometer in mm/hg), Visual analogue scale for pain (VAS) and Lysholm's knee scoring scale was measured initially and after 4 weeks. Statistics: Wilcoxon signed-rank test was performed to observe the impact of biofeedback based on the pre and post-analysis. Female individuals were found to be more when compared to male individuals. Results: Based on the analysis it was found that there was a significant reduction of pain, improved quadriceps isometric strength and functional outcome following the intervention. Conclusion: It may be concluded that the \"modified sphygmomanometer\" may be used as a visual biofeedback tool in relearning�ing the quadriceps activation objectively in individuals with unilateral tibiofemoral osteoarthritis.
Keywords: Modified sphygmomanometer, Isometric quadriceps strength, Unilateral tibiofemoral osteoarthritis, Pain, Disability
Full Text:
Introduction:
Osteoarthritis (OA) of knee is a prevalent musculoskeletal impairment among geriatric population, it is estimated that, the prevalence was found to be 22% to 39% of the total population.1 OA is common in women and the prevalence increases with age. OA knee is accompanied with pain, quadriceps weakness, altered functional abilities and progressive deformity.2 Quadriceps weakness is one of the early clinical observation which is found to emerge before limiting the functional abilities of these individuals and may play a crucial role in disease manifestations.3 Hence, it is imperative for physical therapist to succor the patient in relearning the quadriceps muscle activation at an early stage.4 The strength deficits of quadriceps in the OA knee individuals ranges from 15 to 18% prior to secondary changes to 24% in individuals with Kellgren & Lawrence (K/L) grade II OA and to as high as 38% in individuals with K/L grade IV knee OA.5
Quadriceps has a multiple role at the knee joint in routine activities and reduces impulsive load on to the intra-articular structures.6 Off late, quadriceps weakness is found to be a risk factor for knee pain and is associated with alterations in balance and postural control in individuals with knee OA.7, 8 Evidence from the past shows that quadriceps weakness is analogous with inferior outcome measures which can prognosticate the depreciation in physical ability levels over a period of time in individuals with knee OA.9 Quadriceps weakness can be attributed to multiple factors which can be mechanical or physiological. Despite, pain is identified as the important cause for quadriceps atrophy, it has been observed4 quadriceps weakness is prevalent in individuals with knee OA despite the absence of pain which suggests that pain is not the only factor which instigates the onset of weakness in quadriceps. This gives us an insight of other attributing factors in the incidence of quadriceps weakness. Of which, one of the major cause for quadriceps weakness is Quadriceps Activation Failure (QAF), which is due to impaired neural facilitators effects. These individuals have higher QAF than with their age and sex matched asymptomatic individuals4 QAF is found to be inversely related to the impairment in quadriceps with reduced maximum voluntary isometric contraction (MVIC) and lower physical performance and self?report measures in individuals with knee OA (Fitzgerald GK). The findings of Hurley et al highlights a cascade of events initiated by the mechanical alterations from the degenerated joint structures leading to altered sensory information from mechanoreceptors which results in reduced activation levels of quadriceps muscles.10
Reduced MVIC in individual’s knee OA can reversed by voluntary activation of quadriceps, which is regarded as an appropriate and a reliable approach to improve the strength.11, 12In older individuals with knee OA isometric activation of quadriceps has been found to facilitate the MVIC of the quadriceps with much ease.8, 13, 14 A modified sphygmomanometer is used as a pressure biofeedback in this study in training the strength of the quadriceps. This conventional sphygmomanometer was found to be an affordable and useful alternative in monitoring and maintaining the isometric quadriceps strength during acute phase of post?Anterior cruciate ligament (ACL) reconstruction rehabilitation.15 The objective of this study is to observe the influence of an objective training program by using a modified sphygmomanometer as visual biofeedback tool to facilitate quadriceps activation which can also be cost effective tool.
Methodology:
A case series was performed to observe the influence of a modified sphygmomanometer as a visual biofeedback in isometric quadriceps strengthening in patients with unilateral tibio-femoral Osteoarthritis. Out of 23 patients diagnosed with knee Osteoarthritis, 13 patients who fulfilled the selection criteria were included for the study. During the course of the treatment, there were 2 dropouts and the posttest evaluations were done for 10 patients and in total, females were higher than the male (Table: 1). Written consent was taken from every patient. Approval for this study was obtained from the Institutional Ethics Committee of Sri Ramakrishna Institute of Paramedical Sciences (IEC NO: SRIPMS/COPT/007/03). The inclusion criteria were, both male and female patients aged between 35- 65 years who had mild to moderate unilateral tibio-femoral osteoarthritis. The exclusion criteria were knee deformity, symptomatic patella-femoral arthritis, visual impairment, recurrent dislocation of patella, knee surgeries, recent fractures in lower limb, cardiac patients and ligament injuries. The treatment duration was for about 1 month, where initial assessment was taken on the first day and follow up assessments were taken every week. The assessment tools used are VAS scale, manual muscle testing for quadriceps strength and Lysholm’s knee scoring scale. A brief idea about the treatment and objectives were explained to the patients. Quadriceps muscle strength was assessed using a modified sphygmomanometer.
Apparatus setting
Patient was positioned in long sitting and the cuff of the conventional sphygmomanometer was placed below the knee joint which was inflated up to 100 mm/Hg. The knee joint which has to be treated was flexed to 10 – 15 degrees and supported with a rolled towel. The patient was encouraged to visualize the movement and the apparatus for a better visual feedback to enhance learning.
Procedure:
The patients were instructed to perform an isometric quadriceps contraction, observe the same with the change in mercury levels and hold the same for about 5 to 8 secs. The basal pressure was fixed at 100 mmHg10 and the pressure difference15was noted as gain in isometric quadriceps strength. The patient was instructed to observe the values which served as a visual biofeedback.
They were instructed to perform six times/ week, two sessions/ day with two to three sets/ session. Every set had 10 repetitions with a hold time of 3-5 seconds for the isometric contractions. Adequate rest periods were ensured in between every contractions and every sets. Initially for a week patients were supervised to avoid potential compensations such as pelvic hiking, excessive hamstring and gluteal muscle activity. Later home based exercises program (HEP) with the apparatus was advised for three weeks.
Statistical analysis
Non Parametric tests were performed and the data were expressed as mean and standard deviation. Wilcoxon signed rank test was performed to observe the impact of biofeedback based on the pre and post analysis.
Results:
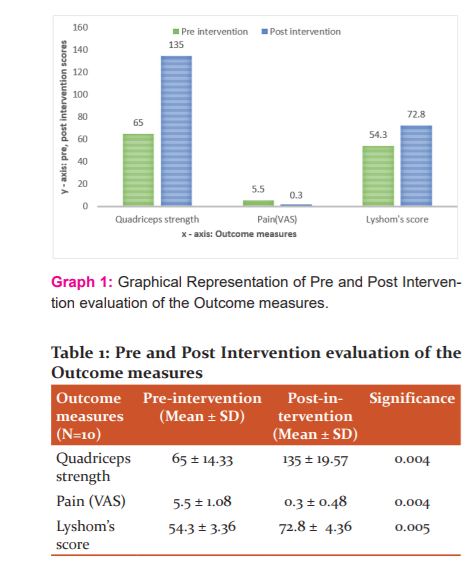
The present study involved 10 individuals between the age group of 35-65 years. The mean age of participants was 42 ± 7 while females were slightly higher than males. The study results showed that there was a statistically significant difference between the pre and post scores of outcome measures of quadriceps isometric strength, pain and functional ability (Graph: 1) with less than 0.01 level of significance (Table: 1).
Discussion:
Biofeedback is considered as a “psychophysiological mirror” which allows the patients to observe and learn from the psychological signals created from the soma. Sphygmomanometer used as a modified biofeedback uses sensors that are entirely non – invasive and helps achieving threshold activation in osteoarthritis knee which may not be possible volitionally in muscles with quadriceps activation failure.16 To gain the strength of a muscle, training programs should impart 30-50% of maximum voluntary effort to impart the overload principle.17 This type of biofeedback device creates a self- awareness and control over the persons own physiological response. As self- awareness increases, the person may achieve insight and control over this action. Concurrently, the therapist utilizes the signal information to monitor and facilitate the particular effort of activation and subsequent strengthening.
Evidence from the past validates that strength and QAF can be improvised by progressive strength training.18In older adults, Henwood and Taaffe et al demonstrated a 17% improvement in strength following retraining exercise. Similarly, individuals demonstrated improvements in both muscle strength and functional performance following progressive strength training.19 Thus, it becomes necessary on the part of the therapist to ensure threshold stimulus for effective activation of quadriceps muscle.
Learning to control brain activity is resulted by the contingent feedback and reward, potential verbal instructions and mental strategies. It is a resultant concurrent occurrence of a strong presynaptic and postsynaptic activity and dopamine release. According to Hebb et alif the activity in the presynaptic neuron led to the firing of the post synaptic neuron, an enduring alteration of the synaptic structure follows, such that subsequent activity of the presynaptic neuron has a high probability to excite the post synaptic neuron. Thus in this type of learning, the synaptic transmission is strengthened only in those neurons that simultaneously receive input coding some aspect of event in the environment and dopaminergic input20. In a clinical stand point, the neuro feedback remains in early development i.e, stimulating the quadriceps muscle in the early stage of quadriceps failure or reflex inhibition, accurate learning helps in maintaining the strength of the muscle and thereby preventing further worsening of the functional status. The improvements in muscle strength occurs as a result of patients learning to activate the quadriceps muscle to a threshold level thereby minimizing the effects of neural arthrogenic inhibition.21
In the study by Raeissadot et al has shown that, there occurs a significant improvement in VAS score on treating patients with Electromyography (EMG) biofeedback.22This is in accordance with this study which could be due to the psychological effects of modified biofeedback. On the other hand, Anwar et al in 2011, evaluated the effects of EMG biofeedback in quadriceps strength in knee OA and found that the maximal voluntary contraction of quadriceps to be significantly greater in biofeedback group.23 The use of modified pressure biofeedback device employed instead of EMG or Neuromuscular Electrical Stimulation (NMES) helps in gaining similar effects and also acts as a cost – effective and a simple acting tool.
There are numerous studies that endorsed that this method is a safe and effective method to treat and evaluate the muscle activation in cervical pathologies, hand grip strength, and low back pain. Thus, sphygmomanometer used as a pressure biofeedback can be an effective alternative in training muscle activation and is also a safe and cost effective tool.
Conclusion
Based on the outcome of this study it may be concluded that a simple “modified sphygmomanometer” may be used as an objective tool in individuals with unilateral tibio-femoral osteoarthritis. Since the study involved limited samples further studies are recommended with structured methodology and with adequate samples.
Acknowledgement:
We are grateful to the patients who volunteered to participate in this study.
Conflict of interest:
No conflict of interest.
Source of funding: Self
Individual Author’s contribution:
-
K Renuka–Methodology, Data Collection
-
Shristhudhi Deepika . S – Writing and Redrafting.
-
Prof. B Sankarmani – Conceptualization
-
Prof. V. S Seetharaman – Original Draft Preparation
-
MohanakrishnanJagadevan – Redrafting, Statistics
-
BhanumathyMohanakrishnan – Redrafting
-
R. Prabakaram- Writing.
APPENDIX
INFORMED CONSENT
Adequate information about the research should be given in simple, easily understandable, unambiguous language in the Participant/ Patient Information Sheet.
Title of the project:
Modified sphygmomanometer as “biofeedback tool” in retraining quadriceps function among individuals with unilateral tibio-femoral osteoarthritis – A case series
Name of the Principle Investigator:
Description of the Study:
The purpose of the study is to find out the effectiveness of exercise program in in retraining quadriceps function among individuals with unilateral tibio-femoral osteoarthritis
Participation in this study is completely voluntary and your consent is required before you can participate in the study.
1 month duration.
The patients will undergo physical examination. Patients with unilateral osteoarthritis underwent quadriceps retraining using a modified sphygmomanometer along with home based exercise program. The assessment tools used are VAS scale, manual muscle testing for quadriceps strength and Lysholm’s knee scoring scale. Quadriceps muscle strength was assessed using a modified sphygmomanometer.
Ethical Clearance Number: SRIPMS/COPT/007/03
-
Investigations, if any, to be performed: Nil
-
Any alternative procedures or courses of treatment that might be as advantageous to the participant as the procedure or treatment to which she is being subjected: Nil
-
Storage period of biological sample and related data with choice offered to participant regarding future use of sample, refusal for storage and receipt of its results: Nil
Possible Risks to the participant: Nil
Cost and Payments to the participant: There is no cost for participation in this study. Participation is completely voluntary and no payment will be provided.
Confidentiality: Information obtained in this study is strictly confidential. Your name will not be used in reporting of information in publications or conference presentations.
Participants’ right to withdraw from the study: You have the right to refuse to participate in this study, the right to withdraw from the study and the right to have your data destroyed at any point during or after the study, without penalty.
Voluntary consent by the participant: participation in this study is completely voluntary, and your consent is required before you can participate in this study.
I have read this consent form (or it has been read to me) and I fully understand the contents of this document and voluntarily consent to participate in the study. All of my questions concerning this study have been answered. If I have any questions in the future about this study they will be answered by the investigators listed below. I understand that this consent ends at the conclusion of this study.
References:
-
Pal CP, Singh P, Chaturvedi S, Pruthi KK, Vij A. Epidemiology of knee osteoarthritis in India and related factors. Indian journal of orthopaedics. 2016 Oct;50:518-22.
-
Punnett L, Wegman DH. Work-related musculoskeletal disorders: the epidemiologic evidence and the debate. Journal of electromyography and kinesiology. 2004 Feb 1;14(1):13-23.
-
Petterson SC, Barrance P, Buchanan T, Binder-Macleod S, Snyder-Mackler L. Mechanisms underlying quadriceps weakness in knee osteoarthritis. Medicine and science in sports and exercise. 2008 Mar;40(3):422.
-
Slemenda C, Brandt KD, Heilman DK, Quadriceps weakness and osteoarthritis of the knee. Ann Intern Med. 1997;127:97–104.
-
Mizner RL, Petterson SC, Stevens JE, Axe MJ, Snyder-Mackder L. Preoperative quadriceps strength predicts functional ability one year after total knee arthroplasty. J Rheumatol. 2005;32:1533–9.
-
Hurley MV. The role of muscle weakness in the pathogenesis of osteoarthritis. Rheum Dis Clin North Am 1999; 25: 283– 98.
-
Messier SP, Royer TD, Craven TE, O'Toole ML, Burns R, Ettinger WH Jr. Long?term exercise and its effect on balance in older, osteoarthritic adults: results from the Fitness, Arthritis, and Seniors Trial (FAST). J Am GeriatrSoc 2000; 48: 131– 8.
-
Fisher NM, Pendergast DR, Gresham GE, Calkins E. Muscle rehabilitation: its effect on muscular and functional performance of patients with knee osteoarthritis. Arch Phys Med Rehabil 1991; 72: 367– 74.
-
Miller ME, Rejeski WJ, Messier SP, Loeser RF. Modifiers of change in physical functioning in older adults with knee pain: the Observational Arthritis Study in Seniors (OASIS). Arthritis Rheum 2001; 45: 331– 9
-
Hurley MV, Scott DL, Rees J, Newham DJ. Sensorimotor changes and functional performance in patients with knee osteoarthritis. Annals of rheumatic diseases. 1997 Nov 1;56(11):641-8.
-
Pietrosimone BG, Saliba SA. Changes in voluntary quadriceps activation predict changes in quadriceps strength after therapeutic exercise in patients with knee osteoarthritis. The Knee. 2012 Dec 1;19(6):939-43.
-
Kim HH, Chang HS. Comparison of the VMO/VL EMG ratio and onset timing of VMO relative to VL in subjects with and without patellofemoral pain syndrome. J PhysTherSci, 2012, 24: 1315–1317.
-
Anwer S, Alghadir A. Effect of isometric quadriceps exercise on muscle strength, pain, and function in patients with knee osteoarthritis: a randomized controlled study. J PhysTherSci, 2014, 26: 745–748.
-
Marks R. The effects of 16 months of angle-specific isometric strengthening exercises in midrange on torque of the knee extensor muscles in osteoarthritis of the knee: a case study. J Orthop Sports Phys Ther, 1994, 20: 103–109.
-
Mohanakrishnan J, Mohanakrishnan B, Salaja R, Balaji GG. Sphygmomanometer as biofeedback in acute anterior cruciate ligament reconstruction rehabilitation: A cost?effective technique. International Journal of Clinical and Experimental Physiology. 2016 Apr 30;3(2):100-4.
-
Peper E, Harvey R, Takebayashi N. Biofeedback an evidence-based approach in clinical practice. Japanese Journal of Biofeedback Research. 2009 Apr 25;36(1):3-10.
-
Henwood TR, Taaffe DR. Detraining and retraining in older adults following long-term muscle power or muscle strength specific training. J Gerontol A BiolSci Med Sci. 2008 Jul;63(7):751–8.
-
Kawakami Y, Akima H, Kubo K, Muraoka Y, Hasegawa H, Kouzaki M, Imai M, Suzuki Y, Gunji A, Kanehisa H, Fukunaga T. Changes in muscle size, architecture, and neural activation after 20 days of bed rest with and without resistance exercise. Eur J Appl Physiol. 2001 Jan-Feb;84(1–2):7–12. ]
-
Skelton DA, Greig CA, Davies JM, Young A. Strength, power and related functional ability of healthy people aged 65–89 years. Age Ageing. 1994 Sep;23(5):371–7.
-
Sitaram R, Ros T, Stoeckel L, Haller S, Scharnowski F, Lewis-Peacock J, Weiskopf N, Blefari ML, Rana M, Oblak E, Birbaumer N. Closed-loop brain training: the science of neurofeedback. Nature Reviews Neuroscience. 2017 Feb;18(2):86-100.
-
Dunn TG, Gillig SE, Ponsor SE, Weil N, Utz SW. The learning process in biofeedback: is it feed-forward or feedback?. Biofeedback and self-regulation. 1986 Jun 1;11(2):143-56.
-
Raeissadat SA, Rayegani SM, Sedighipour L, Bossaghzade Z, Abdollahzadeh MH, Nikray R, Mollayi F. The efficacy of electromyographic biofeedback on pain, function, and maximal thickness of vastusmedialis oblique muscle in patients with knee osteoarthritis: a randomized clinical trial. Journal of pain research. 2018;11:2781.
-
Anwar S, Quddus N, Miraj M. Efficacy of Electromyographic Biofeedback Training on pain and functional status in Osteoarthritis of Knee. Indian Journal of Physiotherapy & Occupational Therapy. 2011 Apr 1;5(2).
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





