IJCRR - 13(16), August, 2021
Pages: 38-51
Date of Publication: 30-Aug-2021
Print Article
Download XML Download PDF
Ayurvedic Management of Serous Pigmentary Epithelial Detachment Associated with Cystoid Macular Edema: A Case Report
Author: Narayanan NN, Kumar A, Krishnendu S, Agaja PL
Category: Healthcare
Abstract:Background: Pigmentary epithelial detachment is classified based on its contents into drusenoid, serous, vascularized, or mixed. It may have ocular and/or systemic involvement. Management options in modern medicine have not been proven effective, hence alternative options may be sought. Case Report: A 70-year-old male who presented with the blurring of vision in his right eye (OD) and diminished vision in his left eye (OS), and who was previously diagnosed with serous PED and who had undergone multiple rounds of LASER photocoagulation, is presented here. He reported for eight rounds of inpatient Ayurvedic management, which involved administering oral medicines and external therapies for both eyes and the head. Results: Improvement in visual acuity fundus photography and optical coherence tomography scanning was noted throughout the eight courses of treatment. Conclusion: The main aim of management was to restore vision as much as possible while giving the patient a better quality of life. This study illustrates that cases of serous PED with cystoid macular oedema can be successfully managed using Ayurveda, and these treatments can be considered as an alternative option.
Keywords: Case report, holistic approach, Kriyakalpa, Timira
Full Text:
Introduction
Physiological forces that maintain adhesion between the retinal pigment epithelium (RPE) and the inner layer of the Bruch’s membrane are disrupted in the different types of PED.1 Long-standing cases have the predilection to develop choroidal neovascularization (CNV), the recognition of which is a major concern secondary to its increased risk for vision loss.2 Serous PED, though having a sometime association with exudative age-related macular degeneration, has a favorable prognosis.3 Blurred vision seen in this variety of PED may be associated with induced hyperopia in some cases.4 Patients over 60 years tend to have a poor prognosis, although variation in the speed of deterioration is demonstrable. No treatment has been proven effective for serous PED, neither have recommendations been established. Although injection of anti-vascular endothelial growth factors (anti-VEGF) may stabilize vision, it carries a 10% risk of RPE tear.5 Cystoid macular edema and macular scarring occur independently of PED. In light of the above, management in the realms of complementary and alternative medicine (CAM), including Ayurveda, may be sought.
Methodology
The efficacy of an Ayurvedic protocol to manage serous PED with cystoid macular edema and macular scar in a 70-year-old male is described in this case report. The report adheres to the Case Report (CARE) guidelines to ensure transparency and efficacy in reporting.6 Institutional Ethics Committee clearance was not required for the study; however, written informed consent was obtained from the patient prior to documenting his case.
Case Report
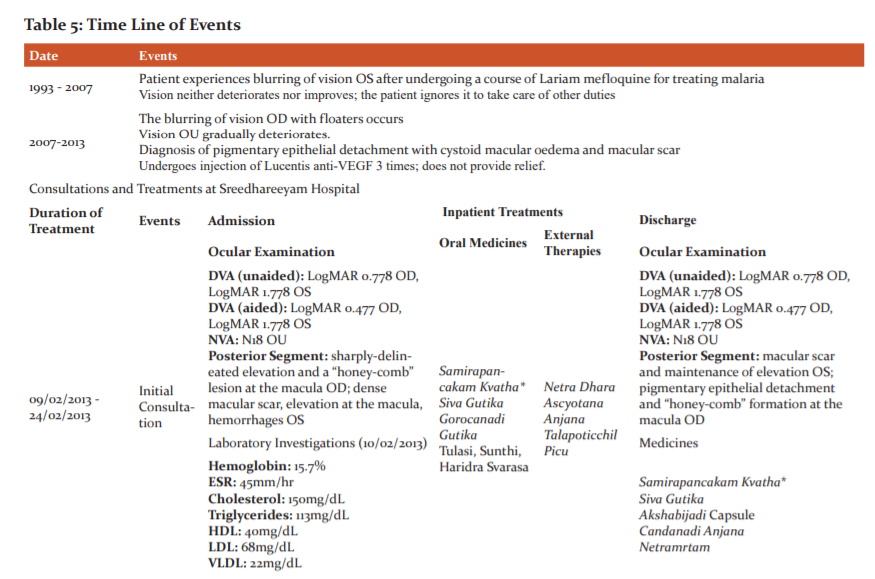
The patient presented with blurring of vision in his right eye (OD – oculus dexter) since 8 years and diminished vision in his left eye (OS – oculus sinister) since 1993. In 1993, he contracted malaria, for which he was prescribed Lariam mefloquine. Blurring of vision OS commenced soon after this, but as it neither increased nor decreased, the patient did not seek ophthalmic consultation. In 2007, he experienced blurring of vision with floaters OD and deterioration of vision OS. He was diagnosed with pigment epithelial detachment and macular scarring and was prescribed anti-VEGF injection. He underwent 3 rounds of injection, but got no relief. His past history is notable for cardiac problems and gouty arthritis, for which he is under medication. His immediate family members do not present with similar complaints. Personal history readings were normal. Review of systems and vital signs were normal.
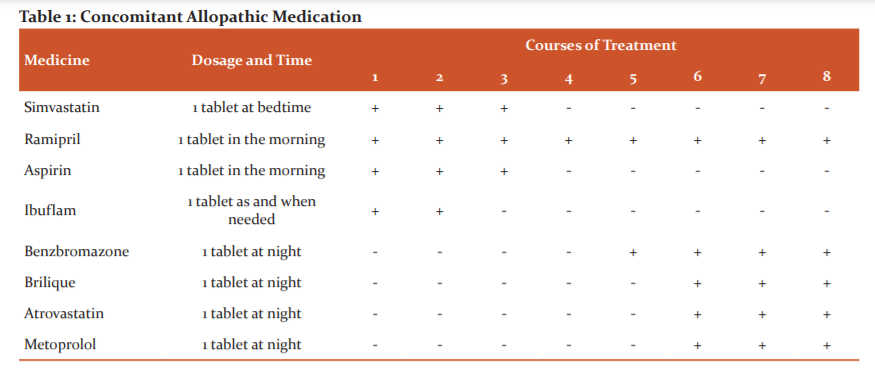
He was taking Simvastatin (1 tablet at bedtime), Ramipril (1 tablet in the morning), Aspirin (1 tablet in the morning), and Ibuflam (1 tablet as and when needed) when he was admitted for his first two courses of treatment. Ibuflam was halted prior to admission for the third course, and all medicines except Ramipril were halted before the fourth course of treatment. Ramipril was continued throughout the remainder of the treatments. The patient had started Benzbromazone (1 tablet at night) prior to admission for his fifth course. Brilique (1 tablet at night), Atrovastatin (1 tablet at night), and Metoprolol (1 tablet at night) were being consumed when the patient came for his sixth course of treatment, and were continued through the seventh and eighth courses. (Table 1)
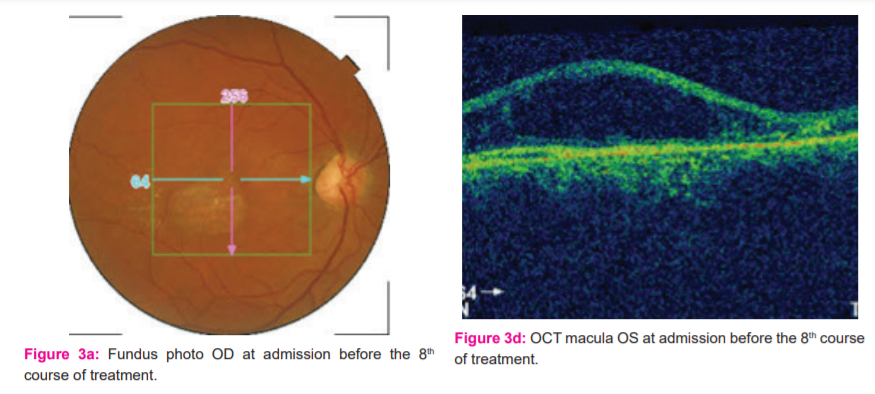
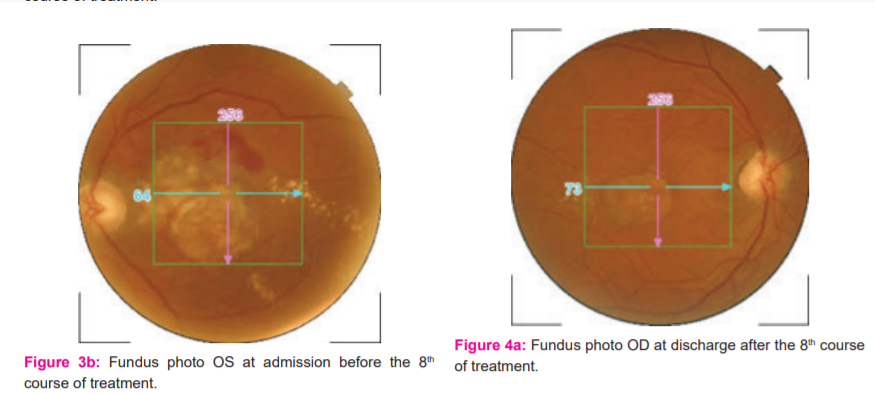
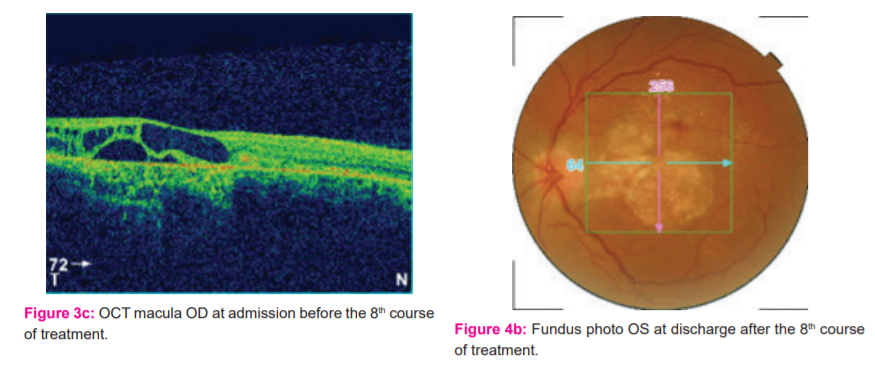
Unaided distant visual acuity ( DVA) was LogMAR 0.778 OD and LogMAR 1.778 OS, aided DVA was LogMAR 0.477 OD and LogMAR 1.778 OS, and near visual acuity (NVA) was N18in both eyes OU (oculus uterque). Anterior segment examination showed normal findings OU. Direct and consensual pupillary reflexes were normal OU. Posterior segment examination by ophthalmoscopy demonstrated a sharply-delineated elevation and a “honey-comb” formation at the macula OD, and a dense macular scar, elevation at the macula, and a few small hemorrhages OS.
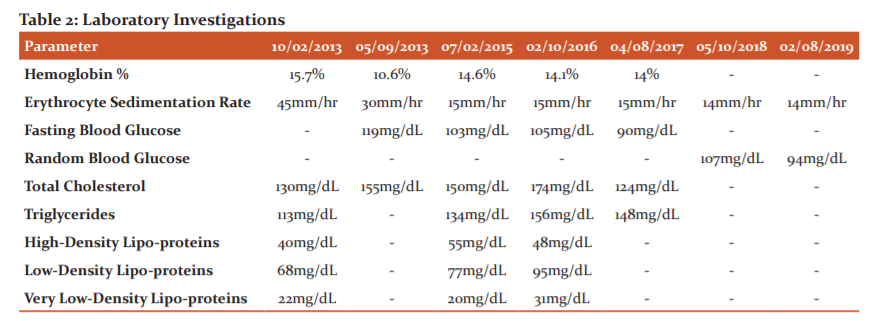
Laboratory investigations conducted at the first course of treatment were hemoglobin percentage, erythrocyte sedimentation rate, and lipid profile analysis, which included total cholesterol, triglycerides, high-density lipo-proteins, low-density lipoproteins, and very low-density lipo-proteins. (Table 2)
Ashta Sthana Pariksha7demonstrated normal Nadi (pulse), Mutra (urine), Mala (excreta), and Sabda (sound), Anupalipta Jihva (non-coated tongue), Anunshna Sita Sparsha (lukewarm touch), abnormal vision, and normal Akrti (stature). Dasavidha Pariksha8 demonstrated a Prakrti (somatic constitution) of Kapha and Vata, normal Sara (essence of tissues), Samhanana (compactness), and Pramana (measurement), medium Sattva (psyche) and Satmya (habituation), low Ahara Sakti (digestion) and Vyayama Sakti (capacity for exercise), and Jirna Vaya (advanced age).
A diagnosis of serous pigment epithelial detachment, cystoid macular edema, and macular scar was made based on the findings. Comparison to Timira (blurring of vision), a Drishtigata Roga (disease of vision) as per Ayurveda was made due to the patient’s symptom of blurring of vision matching with the feature of inability to see distant objects as described in Timira.9
Vulnerability Assessments administered prior to all treatments grouped the patient in the geriatric cohort. Fall Risk Assessment determined that the patient has a visual deficit and no disorientation, self-care deficit, problems with motility, history of a fall, or impaired judgment. Psychological assessment determined that the patient was calm and could carry out his day-to-day activities without assistance.
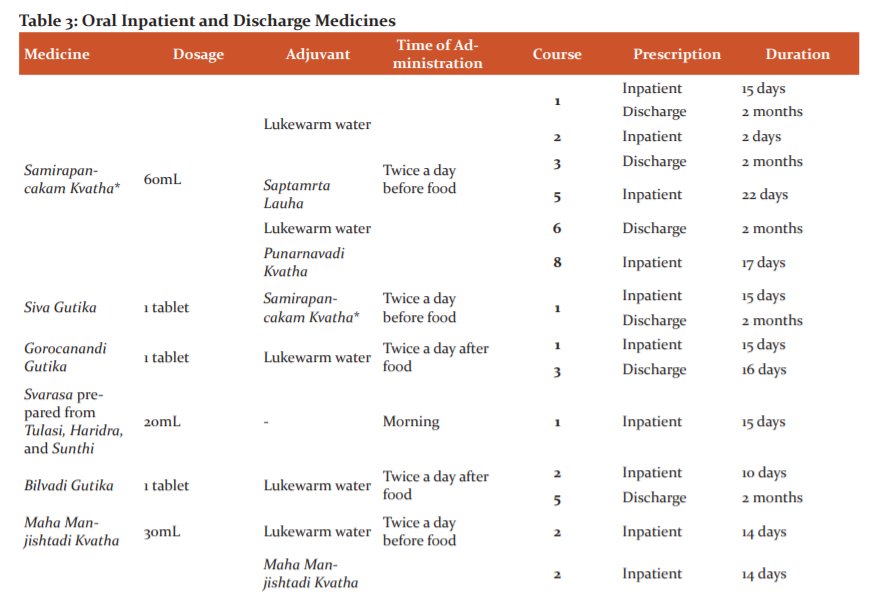
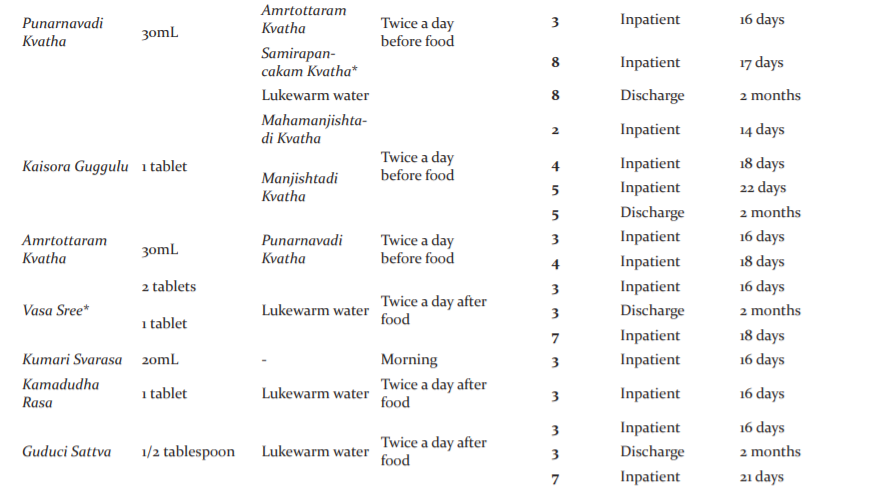
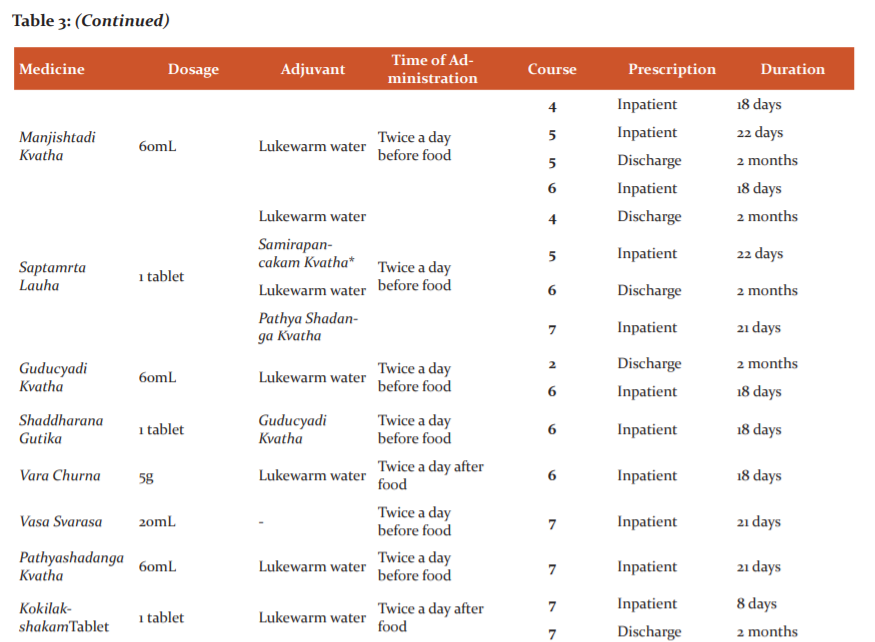
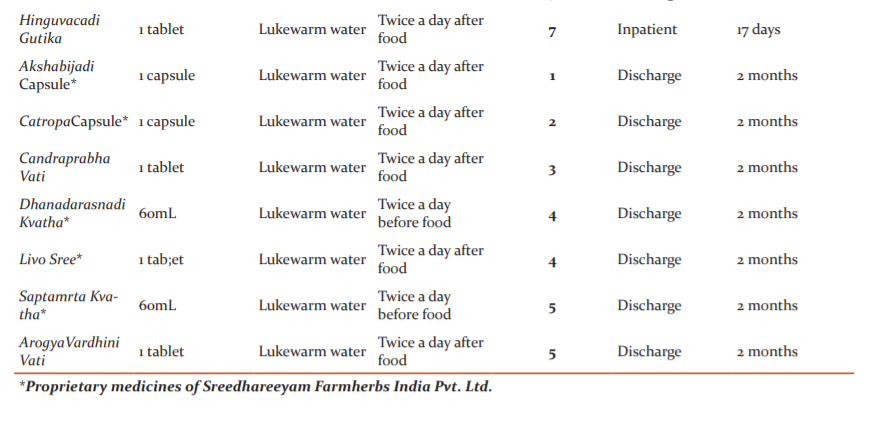
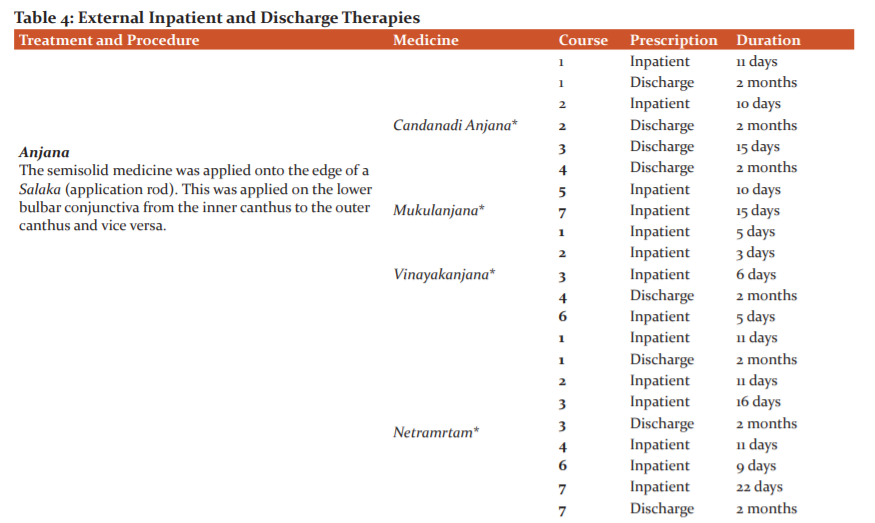
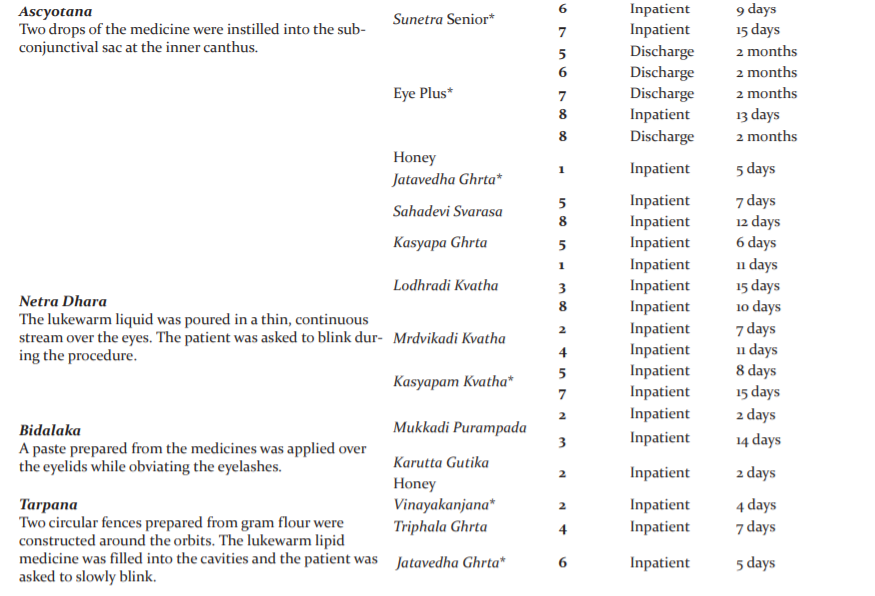
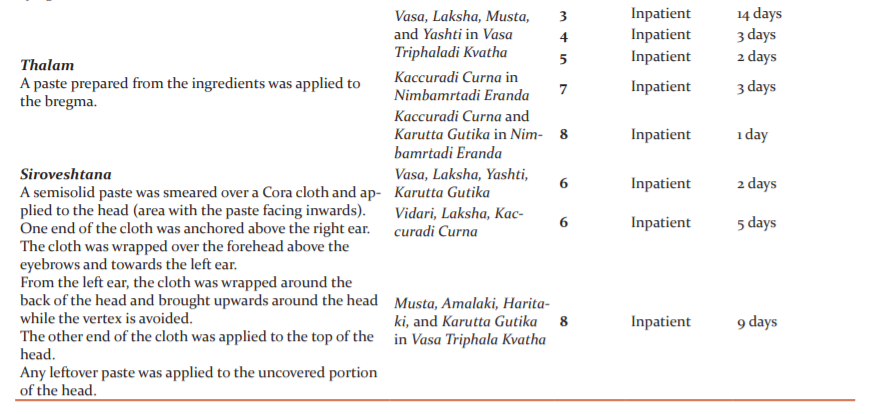
The patient underwent 8 courses of Ayurvedic in-patient therapy. Two rounds were done in 2013, and one round every year from 2014-2019. His tailored Ayurvedic protocol included oral medicines (Table 3) and external therapies for both the eyes (Kriyakalpa) and head (Table 4). He was also advised to continue his allopathic oral medicines at the appropriate times. Pancakarma (bio-purification), generally a requisite in the management of Drishtigata Roga, was not attempted for this patient because of his advanced age.
All medicines were manufactured by Sreedhareeyam Farmherbs India, Pvt. Ltd., the hospital’s GMP-certified drug manufacturing unit.
Outcome Measures and Results
Assessment was done by unaided and aided DVA, posterior segment examination, and optical coherence tomography (OCT) scanning. Initial posterior segment examination was done by ophthalmoscopy.In-house fundus photography and OCT scanning were done at admission before the fifth and sixth courses of treatment; at both admission and discharge of the seventh course; and at discharge after the eighth course of treatment.
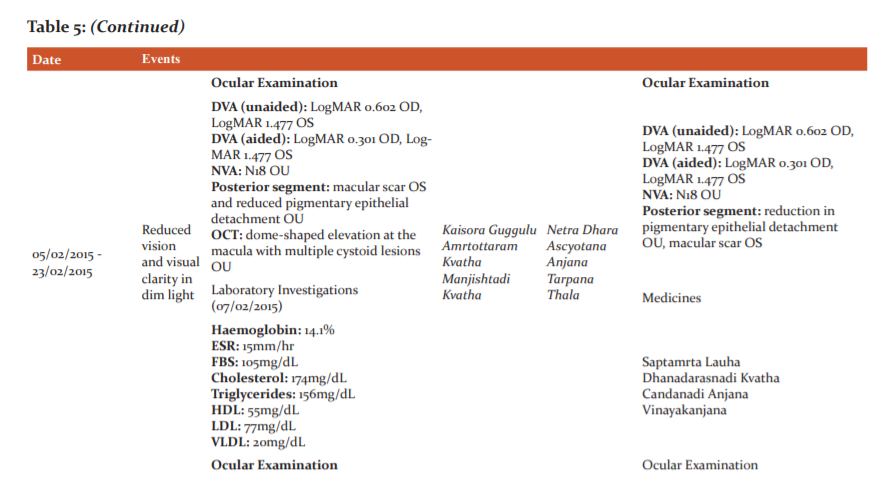
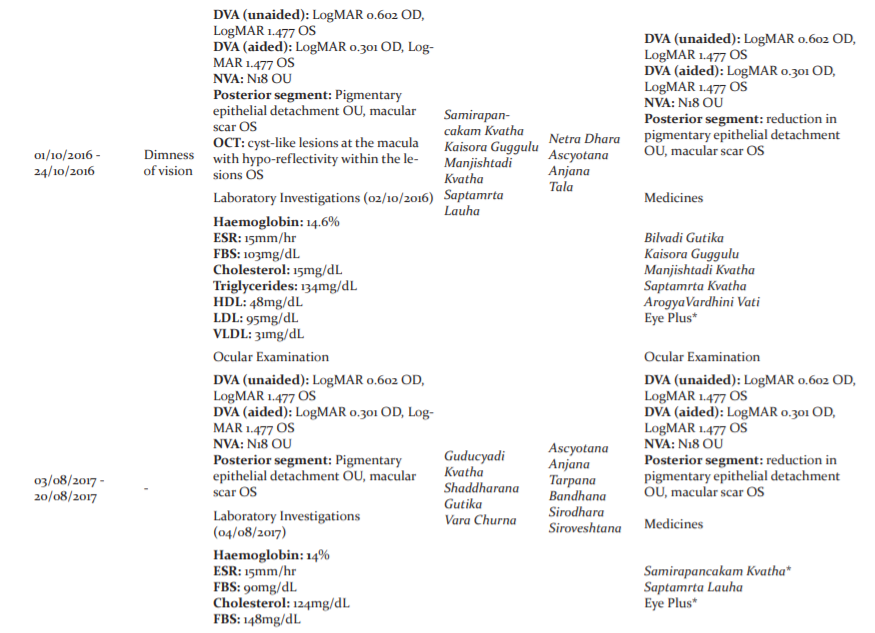
Unaided and aided DVA and NVA was maintained from the end of the first course till discharge after the third course of treatment. Unaided DVA improved to LogMAR 0.602 OD and LogMAR 1.477 OS and aided DVA improved to LogMAR 0.301 OD and LogMAR 1.477 OS at admission for the fourth course of treatment and was maintained till discharge after the seventh course. Unaided and aided DVA OD improved to LogMAR 0.477 and LogMAR 0.176 with maintenance of the other values at admission for the eighth course. The same readings were reported at discharge after the eighth course of treatment.
Laboratory investigations were conducted at all courses of treatment, except the third course. The results of these are described in Table 4.
Posterior segment examination at discharge after the first course of treatment demonstrated gradual reduction and eventual resolution of the “honey-comb” lesion at the macula OD. Complete resolution of the lesion with persistence of the raised pigmentary elevation OU and macular scar OS was demonstrable at the end of the second course of treatment.
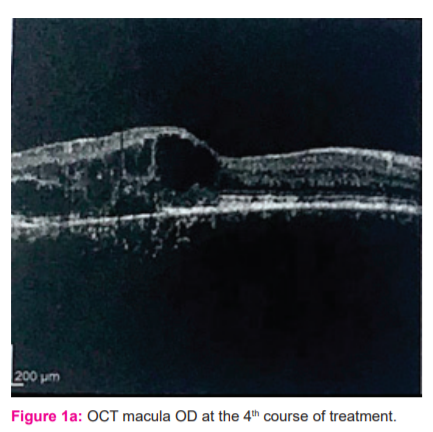
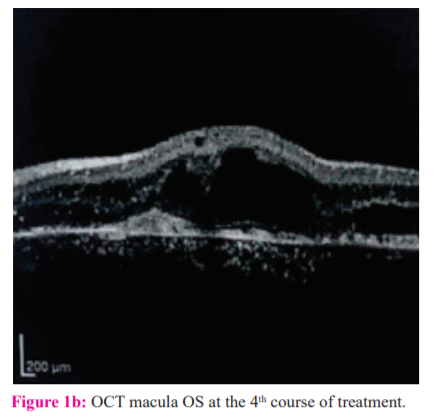
An OCT macular scan brought by the patient at admission for his 4th course of treatment showed a dome-shaped elevation at the macula with multiple cystoid lesions with areas of hypo-reflectivity within them OU (Figures 1a and 1b).
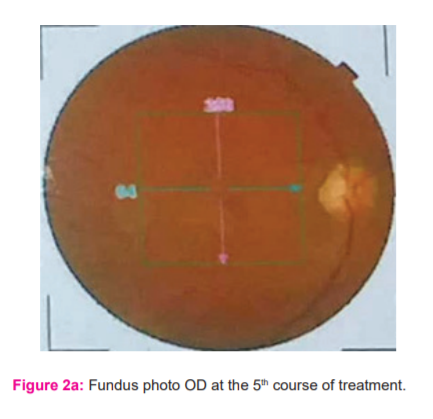
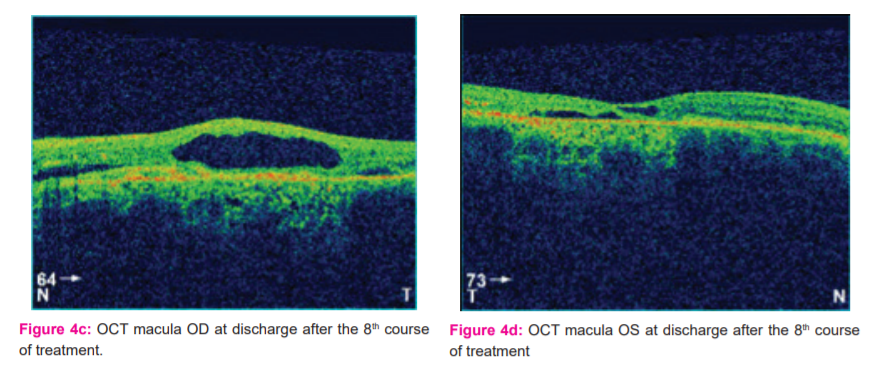
Fundus photography, started at the 4th course of treatment, demonstrated gradual reduction in the pigmentary epithelial elevation OU, although macular scarring OS still persisted. (Figures 2a, 3a, 3b, 4a, and 4b).
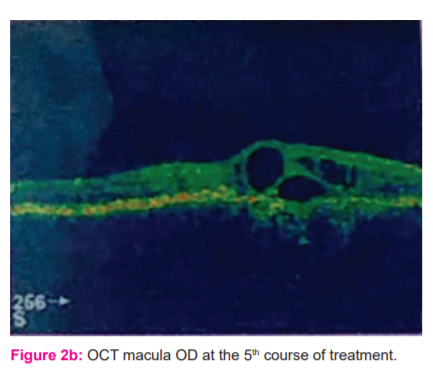
OCT macular scanning demonstrated gradual reduction and ultimate resolution of the cystoid lesions and macular edema. (Figures 2b, 3c, 3d, 4c, and 4d).
A timeline of events for this case is provided in Table 5.
Discussion
The patient’s ocular symptoms started shortly after a course of Lariam mefloquine, a medication used for chemo-prophylaxis against malaria. Maculopathy and optic neuropathy have been described in single cases as side effects to mefloquine chemo-prophylaxis.10 A drug safety study demonstrated pseudo-vitiliform macular dystrophy, central serous retinopathy, macular scarring, and bilateral maculopathy in 9 patients out of 23 cases of retinal disease.11This patient’s blurred vision could be due to macular scarring as a result of lariam mefloquine.
Timira is a dreadful condition that warrants immediate management to prevent it from progressing to Kaca(diminished vision) and Linganasa (blindness).12 It encompasses a wide range of symptoms from indistinct vision (AvyaktaRupa) to Andha(total blindness). The pathology of Timira and all Drishtigata Rogas (diseases of vision) revolves around the Patalas or layers of the eye. Susruta describes Timira when the Doshas settle in the third Patala,13 while Vagbhata describes it when the second Patala is afflicted.14
The scarring of the macula was due to excess Kapha lodging in the retina. Cystoid macular edema was the result of Vata being aggravated at the macula resulting in a crack in the tissue. The accumulation of sub-retinal fluid at the macula was due to excess Kapha seeping through the crack. Detachment of the pigmentary epithelium was due to aggravation of Vata, resulting in the tissue’s detachment.
Oral medicines were prescribed with special care so as to not cause any untoward reactions with the patient’s concomitant allopathic medication. The medicines were instrumental in normalizing metabolism, maintaining homeostasis among the three Doshas, and augmenting the effects of the allopathic medication. Medicines with Guduci (Tinosporacordifolia Miers.) were additionally aimed at the gouty arthritis, as Guduci is the ideal medicine for gout as per Ayurveda. Another medicine specifically indicated for gouty arthritis was the KokilakshakamTablet, described by Ashtanga Hrdaya in the management of Vatarakta, the Ayurvedic correlation of gout. Other medicines were aimed at reducing the edema, normalizing retinal metabolism, and improving vision. The discharge medicines augmented the effects of the inpatient prescriptions.
Kriyakalpas such asAnjana, Tarpana, and Putapaka are indicated after complete Suddhikara (purification) of both the Kaya (body) and Siras (head). However,the dominance of Kapha in this patient warranted the initial application of Anjana from the course of treatment onward. This is echoed in the management of KaphajaAbhishyandaby Acarya Susruta, in which Kriyakalpas such as Anjana and Putapaka may be initially administered.15Netra Dhara and Bidalaka facilitated more rapid expulsion of toxins from the eyes by acting on the eyelids. The use of Tarpana at certain intervals of treatments was to prevent untoward increase of Vata, the prime Dosha in Vriddhavastha. As Timira is a Nanatmaja Vikara (unique disease) of Vata, its management with Tarpana is warranted. The head treatments augmented the effects of the Kriyakalpa and enabled absorption of the essential elements through the scalp to reach the target tissues of the retina.Sirodhara was done with oil at the first course of treatment and with decoction at the sixth and seventh courses. This was due to stabilizing the Doshas in the head.
The majority of the ingredients have the property of Rasayana or rejuvenation. It is a Karma that reinvigorates the Rasadi Dhatus (seven tissue elements) and nourishes them to health.16Acarya Caraka explains that advanced age and conditions due to it warrant some form of Rasayana. This property is effected by not only plants such as Guduci (TinosporacordifoliaMiers.), Guggulu (Commiphoramukul Linn.), Pippali (Piper longumLinn.) and Triphala (Terminalia chebulaRetz.,Terminalia bellericaLinn., and EmblicaofficinalisGaertn.), but also by mineral ingredients such as bitumen, iron, copper, and sulfur.
Conclusion
Two challenges in this case were to maintain vision and improve retinal findings. A concerted effort made by the oral medicines and external treatments resulted in improvements in both vision and retinal findings. Despite these, the retinal scar still persisted. However, the patient felt comfortable with the results of his treatment and was pleased to report for further courses. Multiple rounds of treatment garnered positive results; it reflects the multiple times that treatment needs to be administered in Drishtigata Rogas as per Vagbhata. The results of this report may be analyzed by large-scale sample trials.
Acknowledgment
The authors acknowledge Sreedhareeyam Ayurvedic Eye Hospital and Research Center, and Sreedhareeyam Farmherbs India Pvt. Ltd., for their help in preparing this case report. The authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to the authors/editors/publishers of all those articles, journals, and books from where the literature for this article has been reviewed and discussed.
Conflicts of Interest: None declared
Sources of Funding: None declared
Authors’ Contribution: Dr. N. Narayanan Namboothiri collected the data and reviewed the article. Dr. Aravind Kumar wrote the draft and analyzed the data. Dr. Krishnendu Sukumaran analyzed the data and reviewed the article.
Abbreviations:
PED: pigmentary epithelial detachment
OCT: optical coherence tomography
DVA: distant visual acuity
NVA: near visual acuity
LogMAR: logarithm of the minimal angle of resolution
OD: oculus dexter
OS: oculus sinister
OU: oculus uterque
Previous Publications in the International Journal of Current Research and Review
-
Narayanan Namboothiri Narayanan, Aravind Kumar, Krishnendu Sukumaran, Agaja Peethambaran Leena, An Ayurvedic Protocol to Manage Retinitis Pigmentosa - A Case Report, Int J Cur Res Rev, July 2020; 12(13):25-32 (http://dx.doi.org/10.31782/IJCRR.2020.12135)
-
Narayanan Namboothiri Narayanan, Aravind Kumar, Krishnendu Sukumaran. An Ayurvedic Protocol to Manage Rhegmatogenous Retinal Detachment and the Resultant Macular Hole - A Case Report,Int J Cur Res Rev, July 2020;12(14):10-16 (http://dx.doi.org/10.31782/IJCRR.2020.12143)
-
Narayanan Namboothiri Narayanan, Sreekala Nelliakkattu Parameswaran, Sreekanth Parameswaran Namboothiri, Anjaly Naduvathu Vasudevan, Aravind Kumar, Krishnendu Sukumaran. Management of Proliferative Diabetic Retinopathy and its Associated Conditions using Ayurvedic Therapies: A Case Series, Int J Cur Res Rev, September 2020;12(17):10-22 (http://dx.doi.org/10.31782/IJCRR.2020.121713)
-
Parameswaran SN, Kumar A, Sukumaran K. Management of Central Serous Chorioretinopathy Using Ayurvedic Outpatient Therapies: A Case Report. Int J Cur Res Rev, November, 2020; 12(21):129-135 (http://dx.doi.org/10.31782/IJCRR.2020.12211)
-
Sreekanth Nelliakkattu Parameswaran, Aravind Kumar, Krishnendu Sukumaran. An Ayurvedic Protocol to Manage Myopia in Children: A Case Series.Int J Cur Res Rev., 2020;12 (22):57-65 (http://dx.doi.org/10.31782/IJCRR.2020.12228)
-
Sreekala Nelliakkattu P, Manjusree Radhakrishnan P, Aravind Kumar, Krishnendu Sukumaran. Non-Ischemic Central Retinal Vein Occlusion (CRVO) and its Management using Ayurvedic Therapies: A Case Series. Int J Cur Res Rev, December 2020;12(24): 85-95 (http://dx.doi.org/10.31782/IJCRR.2020.122423)



References:
-
Bowling B, Kanski’s Clinical Ophthalmology: A Systematic Approach, Eighth Edition, Elsevier, Limited. 2016, 606pg.
-
Zayit-Soudry S., Moroz I., Loewenstein A., Retinal pigment epithelial detachment. Surv. Ophthalmol. 2007;52(3):227-243
-
Thorell MR, Pigment Epithelial Detachment, American Academy of Ophthalmology, 2020, https://eyewiki.aao.org/Pigment_Epithelial_Detachment
-
Kanski JJ, Bowling B, Kanski’s Clinical Ophthalmology: A Systematic Approach, Seventh Edition, Elsevier Saunders, an imprint of Elsevier Limited, 2011,618 pg.
-
Bowling B, Kanski’s Clinical Ophthalmology: A Systematic Approach, Eighth Edition, Elsevier, Limited. 2016, 607pg.
-
Gagnier J, Kienle G, Altman DG, Moher D, Sox H, Riley DS, CARE group, The CARE guidelines: Consensus-based clinical case-reporting guideline development, Glob Adv Health Med. 2013;2(5):38-43
-
Kumari A. (Ms.), Tiwari PV. (Ms.), Yogaratnakara: A Complete Treatise on Ayurveda, Part I, Chaukhambha Vishwabharati, Varanasi, First Edition, 2010, 7-20pg.
-
Sharma RK., Dash B., Caraka Samhita: Text with English Translation and Critical Exposition based on CakrapaniDatta’s Ayurveda Dipika, Vol. II, Chaukhambha Sanskrit Series Office, Varanasi, Reprint 2013, 260-67pg
-
Murthy KRS, Ashtangahrdaya of Vagbhata: Text, English Translation, Notes, Appendices, and Index, Vol. III, Krishnadas Academy, Varanasi, 2000, 121pg.
-
Walker RA, Colleaux KM, Maculopathy associated with mefloquine (Lariam) therapy for malaria prophylaxis, Can J Ophthalmol.2007;42:125-126
-
Adamcova M, Schaerer MT, Bercaru I, Cockburn I, Rhein HG, Schlagenhauf P, Eye disorders reported with the use of mefloquine (Lariam) chemoprophylaxis: A drug safety database analysis, Travel Med Infect Di. 2015, http://dx.doi.org/10.1016/j.tmaid.2015.04.005
-
Murthy KRS, Ashtangahrdaya of Vagbhata: Text, English Translation, Notes, Appendices, and Index, Vol. III, Krishnadas Academy, Varanasi, 2000, 121 pg.
-
Sharma PV, Susruta Samhita: With English Translation of Text and Dalhana’s Commentary alongwith Critical Notes, Vol. III, Chaukhambha Vishwabharati, Varanasi, 2010, 101 pg.
-
Murthy KRS, Ashtangahrdaya of Vagbhata: Text, English Translation, Notes, Appendices, and Index, Vol. III, Krishnadas Academy, Varanasi, 2000, 101pg.
-
Sharma PV, Susruta Samhita: With English Translation of Text and Dalhana’s Commentary alongwith Critical Notes, Vol. III, Chaukhambha Vishwabharati, Varanasi, 2010, 161 pg.
-
Sharma RK., Dash B., Caraka Samhita: Text with English Translation and Critical Exposition based on Cakrapani Datta’s Ayurveda Dipika, Vol. III, Chaukhambha Sanskrit Series Office, Varanasi, Reprint 2013, 4 pg.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





