IJCRR - 13(15), August, 2021
Pages: 72-76
Date of Publication: 10-Aug-2021
Print Article
Download XML Download PDF
Efficacy of Transcutaneous Electrical Nerve Stimulation (TENS) with Muscle Energy Technique (MET) on Quadratus Lumborum in Acute Unilateral Lumbar Strain
Author: Ganesh Sundaram Subramanian, Jency Thangaseela, Mahendran Sekar
Category: Healthcare
Abstract:Introduction: Lumbar strain is characterized as pain subsequently arising in the region between the lower rib margin and the proximal thighs. However, relapses and recurrences are normal, occurring within six months in about 40% of patients. Studies of physical therapy for lumbar strain are heterogeneous because the intervention method differs, it can include education, exercises, manipulation, as well as modalities such as heat. Transcutaneous Electrical Nerve Stimulation (TENS) and Muscle Energy Technique (MET) are widely used physiotherapy techniques to reduce unilateral lumbar strain. It would be interesting to study the treatment outcome when these two techniques have combined. Objective: The present study aimed to evaluate the effectiveness of TENS with MET on quadratus lumborum in acute unilateral lumbar strain. Methods: In the total of 30 volunteers including males and females with no history of musculoskeletal disease has been selected based on the specific inclusion and exclusion criteria's. They were recruited for the study based on unilateral back pain experiencing around or near lumbar and thoracolumbar segments and positive muscle length tests for erector spinae and quadratus lumborum. All the subjects were assigned into three groups, Group-1 patients undergone TENS treatment, Group-2 patients treated by MET and Group-3 patients were treated by a combination of TENS with MET in the lumbar spine. All these treatments were given five consecutive days a week for a total of three weeks. Pain intensity and discomfort were evaluated before and after the treatment programme. The outcome of the treatment was measured after three weeks from each patient's pain and disability using the Numerical Pain Rating Scale (NPRS) and Modified Oswestry Disability Questionnaire (MODI) were considered for assessment and analysis. Results: There was a reduction in disability index and pain were observed when TENS, MET and TENS with MET treatments. However, the combined treatment of TENS with MET showed a significant reduction (p< 0.01 and p< 0.001) in disability index and pain when compared to the groups treated with TENS and MET individually. Conclusion: The results of the present study indicated that MET along with TENS can be used as an effective therapeutic maneuver to reduce pain intensity and disability improvement.
Keywords: Transcutaneous Electrical Nerve Stimulation, Muscle Energy Technique, Quadratus Lumborum, Unilateral Lum�bar Strain, Modified Oswestry Disability Questionnaire
Full Text:
INTRODUCTION
Low back pain (LBP) is an incredibly common symptom that individuals of all ages encounter.1The multifidi, erector spine, the psoas and the quadratus lumborum provide muscle support for the low back.2 Muscles that tend to become tight are usually those that span more than one joint namely, quadratus lumborum and erector spinae (especially lumbar and thoracolumbar segments). Any acute pain in the lumbar motion segment can initiate muscle responses which, if they persist, can alter the patients’ pattern of movement and in turn perpetuate adverse strains on the lumbar spine.3 The most commonly overlooked muscular source of low back pain is the quadratus lumborum muscle.4 Based on the information obtained from the literature review, it was found that joint and muscle dysfunction occur together. Franca et al., 1991 stated that a taut and painful quadratus lumborum, as well as articular dysfunction in the lumbar spine, requires appropriate therapy to provide relief and restore function.5
In patients with low back pain, the goals of physiotherapy include pain elimination, restoration of the lost extent of movements, functional improvement, and quality of life.6These goals are achieved by different techniques of exercise, electrotherapy, and relaxation protocols. One of the most common therapeutic modalities aimed at improving elasticity in contractile and non-contractile tissues is the muscle energy technique (MET).7Greenman defined MET as a manual medicine treatment technique involving the voluntary contraction of the subject's muscle in an appropriately guided direction, at varying strength rates, against the therapist's distinctly performed counterforce. MET has shown improvements in range of motion, reducing pain-relieving muscle tension and spasm. Fryer has suggested that MET will activate joint and muscle proprioceptors, enhancing muscle deep segment recruitment, motor control and joint stability.8-9
Transcutaneous electrical nerve stimulation (TENS) is used as a treatment modality because it offers a non-invasive procedure to reduce both acute and chronic pain by attaching two or more electrical pads to a person’s skin. High-frequency (HF; P10 Hz), low-frequency (LF; <10 Hz), variable-frequency (VF) and acupuncture-like (AL) are the various types of stimulation modes that employ very low-frequency, high-amplitude stimulation. Two theories have explained the mechanism of action of TENS for pain relief: the gate control theory and stimulus-induced release of endogenous endorphins.10 All though most of the studies provide mixed evidence of TENS in low back pain reduction and others reporting short term benefits for disability but not pain.11
However, so far there is no study has been reported on the effect of combined treatment of TENS with MET on quadratus lumborum in acute unilateral lumbar strain to reduce disability index and pain, though these two techniques are widely used. Therefore, the present study aimed to analyze and compare the efficacy of combined treatment of TENS with MET and its physiotherapy outcomes in unilateral lumbar strain in reducing disability index and pain.
METHODS
-
Study design:
The study was an experimental study design with pre-test and post-test. The study was conducted in the physiotherapy unit of Ram Polyclinic, Pollachi, Tamilnadu, India. The study protocol was approved by the Institutional Review Committee of Cherraan’s College of Physiotherapy, Coimbatore, Tamilnadu, India(Ref: CCPT/PG/2014/1). Patients were invited to participate in this study and their consent was obtained after describing the objective of the research, process, risk factors, benefits, withdrawal rights, and ensuring that confidentiality was maintained.
-
Study Participants:
The sample of 30 volunteer patients who visited the Ram Polyclinic, Pollachi, Tamilnadu, India, with low back pain were selected for the research. Among them 18 were male and 12 were female patients. One of the research suggested that the Oswestry Disability Index (ODI) Questionnaire's Tamil version is a legitimate and accurate instrument that can be used to assess subjective pain and impairment outcomes. The patients were placed into three groups with ten patients in each group (n=10). All the patients showed great interest in this study.
A. Inclusion criteria: (1) Patients between the ages of 18 and 45 (2) Low back pain cases of two months, or less. (3) Pain restricted to the lumbar region, without buttock radiation. (4) Orthopedic special tests: standing side flexion test or Hip Abduction test or Isometric contraction test.
B. Exclusion criteria:(1) Paresthesia, numbness and sensory fatigue in patients. (2) Patients with muscle reflexes missing or diminished; (3) Spondylolisthesis or earlier surgery to the leg. (4) History of lower back injuries. (5) Patients refusing to sign an informed consent form. (6) Acute infections, neoplasms or systemic disorders.
-
Intervention:
Pain and discomfort were measured using Modified Oswestry Disability Index (MODI) Questionnaire and the Numerical Pain Rating Scale (NPRS) for each patient as pre-test and post-test measurements.
A. Treatment by TENS
Group-1 patients (n=10) were made to lye prone in the bed and the therapist stands by the side of the patient. The electrodes of the TENS was placed at the site of pain with the ultrasound gel. Patients were treated for two sessions a day and each Session carried for 20 min.
B. Treatment by MET
Group-2 patients (n=10) were made to lye supine in the bed and the therapist stands by the side of the patient. Once the patient has adopted the banana position, the therapist places their right hand under the head of the patient and cradles the right axilla. The left hand of the therapist stabilizes the patients left pelvis. From this position, the patient is asked to side bend to the right against the resistance applied to their axilla by the therapist’s right hand. After a 10 sec contraction and on the relaxation phase, the therapist induces further side bending to the left. Patients were treated for two sessions a day and each session carried for 5 min (Figure. 1).

C. Treatment by TENS with MET
Group-3 patients (n=10) was made to lye prone in the bed and the therapist stands by the side of the patient. The TENS was carried for 20 min then MET was carried for 5 min by using the procedure mentioned above.
IV. Statistical Analysis
All the obtained data were analyzed by using GraphPad Prism software (Version 5.0). The values were expressed as mean±SD. P values <0.05 were considered as significant.
RESULTS AND DISCUSSION
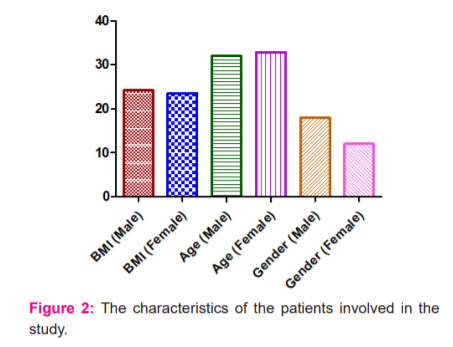
In the present study, we investigated the combinatory effect of TENS with MET treatment on pain and disability for quadratus lumborum in subjects with acute unilateral lumbar strain.The characteristics of the participants involved in the study were BMI (Male) = 24.20±1.93, BMI (Female) = 24.39±2.03, Age (Male) = 32.00±6.80, Age (Female) = 32.92±8.80, Gender (Male) = 18, Gender (Female) = 12 (Figure 2).
Muscle energy technique was demonstrated to be effective in increasing the restricted range of trunk rotation in the thoracic region and ameliorating rotational asymmetry in asymptomatic subjects.12 The disability index value was reduced from 34.77 ± 8.08 to 31.10 ± 6.67 after the treatment with TENS alone. The numerical pain rating value also reduced from 6.50 ± 1.10 to 5.20 ± 1.40 after the TENS treatment. One of the research reveals an analgesic effect under various painful conditions and confirms the utility of TENS in clinical practice.13 It was found there was no statistically significant difference between the TENS and the interferential groups; only those groups and the controls found a difference when treating chronic low back pain.14Pain study assessed on VAS and McGill pain questionnaire before and after treatment. One of the earlier studies reported that ultrasound treatment and exercise reduced pain and disability results when treated by TENS.15 Another study reported that MODI to be both accurate and appropriate for the assessment of impairment in patients with low back pain.16 Our results also in line with the results published earlier on TENS by reducing pain and disability index.12-16
The disability index value was reduced from 34.62 ± 7.15 to 32.80 ± 7.44 after the treatment with MET alone. At the same time, the numerical pain rating value also reduced from 6.60 ± 1.35 to 5.90 ± 1.45 after the MET treatment. One of the earlier studies support our findings and mentioned that MET is effective in decreasing pain in patients with acute low back pain. As MET is a low force isometric contraction in a pain-free position. The subjects receiving MET showed a decrease in the visual analogue scale (VAS), indicating that MET could be useful in reducing Lumbopelvic pain.17 The MET and mobilization are both effective in treating chronic low back pain due to sacroiliac joint dysfunction. The reduction in pain due to MET can be extrapolated, as post, isometric relaxation refers to the subsequent reduction in tone of the agonist's muscle after isometric contraction.18One another study also mentioned that MET, proprioceptive neuromuscular facilitation and static stretching can be used as an effective therapeutic manoeuvre to decrease pain, improve range of motion and flexibility of tight hamstring in a chronic low back pain patient.19
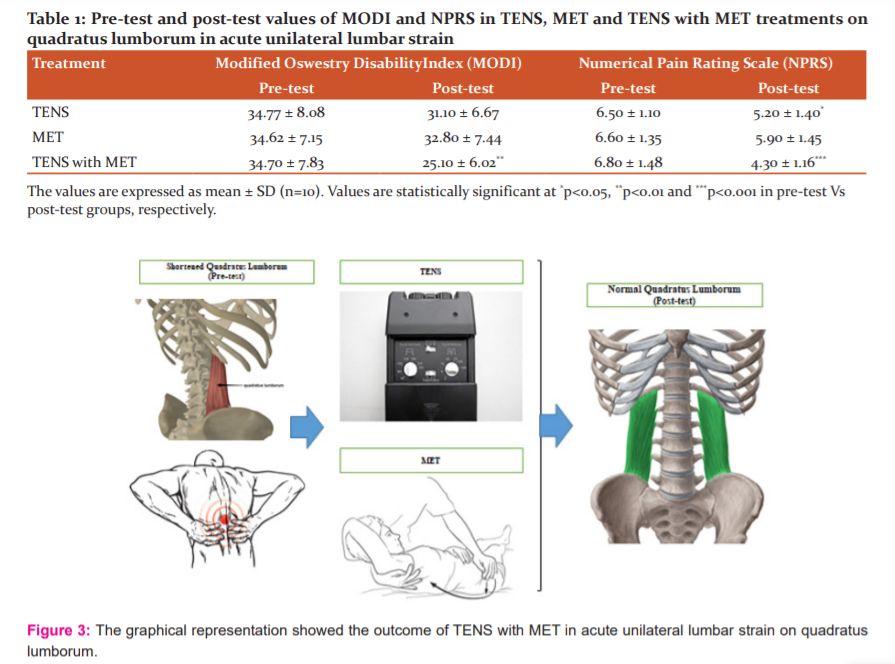
The disability index value was reduced from 34.70 ± 7.83 to 25.10 ± 6.02 after the combination treatment of TENS with MET (Table 1). The numerical pain rating value also reduced from 6.80 ± 1.48 to 4.30 ± 1.16 after combination treatment of TENS with MET. There was a significant decrease (p<0.01) in the disability index and also a significant reduction in pain (p<0.001) were observed when combination treatment with TENS and MET. Hence, our study results demonstrated that the combined treatment of TENS with MET showed a significant reduction in disability index and pain when compared to TENS and MET treatment individually. So, the changes observed in this study are noteworthy. The general graphical representation of the present study outcome shown in Figure 3.
TENS is a nonpharmacological intervention that activates a complex neuronal network to reduce pain by activating descending inhibitory system. MET technique is more advantageous as the administration time is short and release the tight muscles with no direct implication on joint structures.
Overall, the present results showed that TENS with MET showed significant effects concerning pain intensity reduction and disability improvement. Although high-frequency low-intensity TENS has been extensively used to relieve low back pain. The combined effect of TENS with MET helps to strengthen weak muscles, as the patients can perform isometric contraction before lengthening process in acute strain.
CONCLUSION
The findings of the present study showed that MET with TENS on quadratus lumborum delivered substantial improvements in the reduction of pain intensity and disability improvement. This may improve the activity levels, function and quality of life in lumbar strain patients. It is recommended that future studies can be done with a large sample size or on other electrotherapy modalities including ultrasound.
ACKNOWLEDGEMENTS
The authors appreciate Ram Polyclinic, Pollachi, Tamilnadu, India and Cherraan’s College of Physiotherapy, Coimbatore, Tamilnadu, India for providing the facilities and services required to complete the study.
CONFLICTS OF INTEREST
All the authors declared that there is no conflicts of interest.
FUNDING
Nil
AUTHOR CONTRIBUTIONS
G.S.S. conceived the idea, designed, collected the literature, interpreted the data, analyzed the data, drafted and revised the manuscript. All the authors have made noteworthy contributions to the study design, data collection, review and interpretation; have engaged in the drafting or revision of the article; have agreed to submit to the current journal; have given final approval of the version to be published.
References:
1. Hoy D, Bain C, Williams G. A systematic review of the global prevalence of low back pain. Arthritis Rheum 2012;64(6):2028-2037.
2. Sions JM, Elliot JM, Pohling RT, Hicks GE. Trunk muscle characteristics of the multifidi, erector spinae, psoas and quadratus lumborum in older adults with and without chronic low back pain. J Orthoped Sports Physiother2017;47(3):173-179.
3. Twomey L and Taylor J. Physical Therapy of the Low Back. Churchill Livingstone. 1987; pp 328.
4. Travell J, Simmons DG. Myofascial pain and dysfunction the trigger point manual. Lippincott Williams and Wilkins, 1999; pp 437.
5. Franca GD, Levine L. The quadratus lumborum and low back pain. J ManipulPhysiolTherapeut991;14(2):142-149.
6. Szulc P, Wendt M, Waszak M, Tomczak M, Cieslik K, Trzaska T. Impact of McKenzie method therapy enriched by muscular energy techniques on subjective and objective parameters related to spine function in patients with chronic low back pain. Med SciMonit2015;21:2918-2932.
7. Chaitow L. Muscle energy technique. (4th Ed.), Churchill Livingstone, 2014.
8. Fryer G. Muscle energy concepts – A need for a change. J Osteopath Med 2000;3(2):54-59.
9. Greenman PE. Principles of manual medicine. (3rd Ed.) Baltimore; Williams and Wilkins, 2003.
10. Melzack R, Vetere P, Finch L. Transcutaneous electrical nerve stimulation for low back pain – A comparison of TENS and massage for pain and range of motion. Physical Therapy. 1983;63(4):489-493.
11. Binny J, Wong NLJ, Garga S, Christine Lin CW, Maher CG, McLachlan AJ, et al. Transcutaneous electrical nerve stimulation (TENS) for acute low back pain: Systematic review. Scand J Pain. 2019;19(2):225-233.
12. Lenehan KL, Fryer G, McLaughlin.P.The effect of muscle energy technique on gross trunk range of motion. J Osteopath Med. 2003;6(1):13-18.
13. Naka A, Keilani M, Loeffler S, Crevenna R. Does transcutaneous electrical nerve stimulation (TENS) have a clinically relevant analgesic effect on different pain conditions? A literature review.Eur J Translation Myol - Basic Appl Myol. 2013;23(3):95-104.
14. Facci LM, Nowotny JP, Tormem F, Trevisani VF. Effects of transcutaneous electrical nerve stimulation (TENS) and interferential currents (IFC) in patients with nonspecific chronic low back pain: a randomized clinical trial. Sao Paulo Med J. 2011;129(4):206-216.
15. Alyazedi1 FM, Khan S, Ghamdi AH, Toriri N, Shamsi S. Effect of ultrasound and exercise together and TENS alone in the management of chronic back pain. IOSR J Nurs Health Sci. 2015;4(5):110-114.
16. Fritz JM, Irrgang JJ. A comparison of a modified Oswestry lows backs pain disability questionnaire and the Quebec back pain disability scale. Physic Therapy. 2001;81(2):776-788.
17. Selkow NM, Grindstaff TL, Cross KM, Pugh K, Hertel J, Saliba S. Short-term effect of muscle energy technique on pain in individuals with non-specific lumbopelvic pain: A Pilot Study. J Manual Manipul Therap.2006; 17(1):14-18.
18. Sharma D, Sen S. Effects of muscle energy technique on pain and disability in subjects with SI joint dysfunction. International J Physiother Res. 2014;2(1):305-311.
19. Kumar P, Moitra M. Efficacy of muscle energy technique and PNF stretching compared to conventional physiotherapy in the program of hamstring flexibility in chronic nonspecific low back pain. Indian J Physiother Occupation Ther. 2015;9(3):103-107.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





