IJCRR - 13(14), July, 2021
Pages: 96-100
Date of Publication: 20-Jul-2021
Print Article
Download XML Download PDF
Strategies in The Management of Acute Appendicitis Among South Indian Population-Comparison of Modified Ripasa and Alvarado Scores
Author: Kannappan M, Ravindra Kumar, Dhanapal RR, Ramakrishnan R
Category: Healthcare
Abstract:Introduction: Acute Appendicitis is one of the most common surgical emergencies and the most difficult to diagnose clinically in equivocal cases. Of the various clinical scoring systems, ALVARADO is the time tested scoring system. But the reliability of this scoring system among the Asian population has been debated. So we have compared the modified Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA), a score designed for the Asian population, to the ALVARADO scoring system in diagnosing acute appendicitis among the South Indian population. Aim: To compare the usefulness of modified RIPASA and Alvarado's scores in the diagnosis of acute appendicitis among the Indian population. Materials and Methods: The entire study population who presented to Sri Ramachandra Medical College and Research Insti�tute, above the age of 18 years, with history and clinical features suggestive of acute appendicitis were scored with both Alvarado and Modified RIPASA scores. The modification done in the original RIPASA score for our study is the removal of the score for residential foreigner, as our study is based on the Indian population. The cut-off score to diagnose acute appendicitis in Modified RIPASA and ALVARADO was fixed at 7.5 and 7. Results: On comparing both the scores the sensitivity and specificity were higher for the Modified RIPASA score. This statistical significance is further backed up by the receiver operator curve (ROC) graph, which shows a larger area under the curve for Modified RIPASA (0.818) when compared to Alvarado (0.615). Conclusion: The Modified RIPASA, a simple and easy scoring system, shows promising results in a South Indian population with higher sensitivity and specificity than the ALVARADO score.
Keywords: Modified RIPASA, ALVARADO, Acute Appendicitis, Laparoscopic Appendicectomy
Full Text:
INTRODUCTION
Acute appendicitis is the most common cause of abdominal pain in both developed and developing countries. The lifetime risk of acute appendicitis in males and females is 8.6%, 6.7%, respectively with a lifetime risk of having an appendectomy reported to be 12% for men and 25% for wome.1,2
Though being very common in surgical practice, the diagnosis of acute appendicitis remains elusive even to the best of clinicians; hence the time tested clinical scoring system ALVARADO, which incorporates 6 clinical findings and 2 laboratory results and gives a total score of 10, is used in segregating patients into high, moderate and low suspicion of appendicitis. But in equivocal cases, still, imaging techniques are also used generously to prevent negative appendectomies and avert the risk of perforation. But a recent study has suggested that such indiscriminate use of CT imaging may lead to early low-grade appendicitis and unnecessary appendectomies which would otherwise be resolved spontaneously by antibiotics therapy.3 To mitigate this low sensitivity and specificity a new scoring system was devised in Malaysia, namely RIPASA.
The RIPASA score is a simple and easy to use the quantitative scoring system and most of the 14 clinical parameters are easily obtained from a good clinical history and examination. The RIPASA scoring system includes more parameters than the Alvarado system and the latter did not contain certain parameters such as age, gender, and duration of symptoms before presentation. These parameters are shown to affect the sensitivity and specificity of the Alvarado scoring system in the diagnosis of acute appendicitis. This also includes a urinalysis, which can be easily performed on the spot. Hence a score can be obtained quickly and a rapid diagnosis made without having to wait for the full investigations to be available when a score of >7.5 is obtained. The additional parameter that is unique to our local population consists of foreign nationality, as the probability of acute appendicitis among foreign nationals presenting with RIF pain is high. The RIPASA score has been shown to have significantly higher sensitivity, specificity and diagnostic accuracy compared to Alvarado Score, particularly when applied to Asian population.4The modified RIPASA scoring’s sensitivity and specificity is tested in the Indian population in this study.
MATERIALS & METHODS
The study was done after obtaining the Institutional Ethics Committee’s clearance (IEC ref no. CSP MED/15/OCT/25/91). All patients who presented to Sri Ramachandra Institute of Higher Education and Research (SRIHER), with a history and clinical features suggestive of acute appendicitis were included in the study. The study was done from April 2015 to October 2017.
All patients above the age of 18 years with history and clinical features suggestive of acute appendicitis were included in the study. Patients willing to participate in the study with no previous history of acute appendicitis were also included in the study. Patients excluded from the study were those not willing to participate and those with other coexistent pathologies.
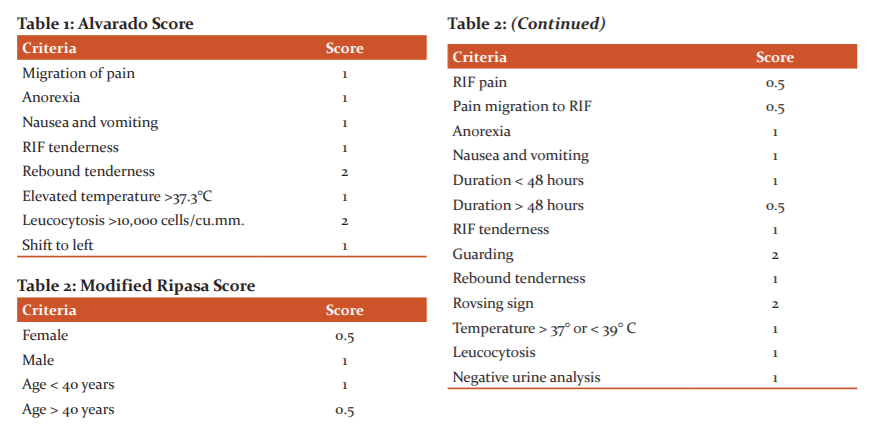
All patients were scored using both Alvarado [Table 1] and Modified RIPASA [Table 2]. The removal of foreign NRIC (which amounts to a value of 1) from the original RIPASA score will be the modification made in this study.
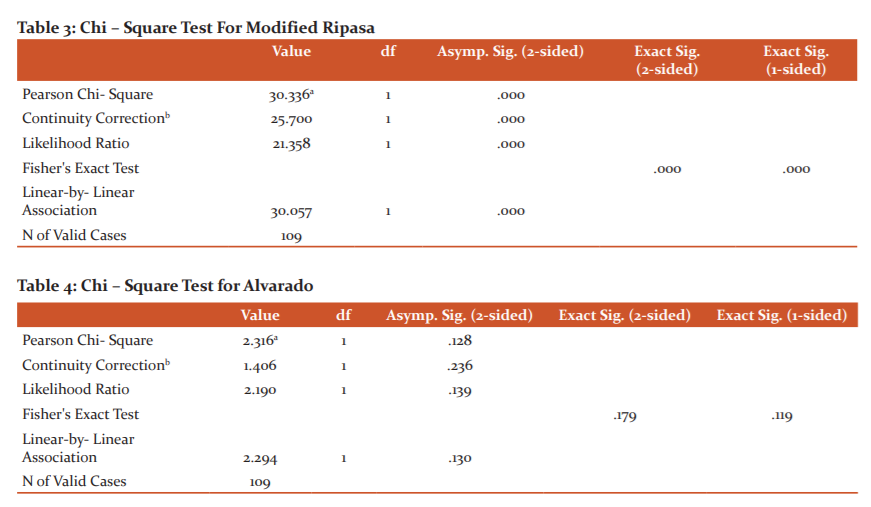
All patients underwent Laparoscopic appendicectomy by standard three-port technique under general anaesthesia.5 A 10mm port was placed at the umbilicus and pneumoperitoneum created with carbon dioxide and two more 5 mm ports placed in the right and left iliac fossa to perform appendicectomy [Figure 1]. The histopathology reports of the appendicectomy specimen were collected. Acute appendicitis was diagnosed based on neutrophilic infiltration in the muscular propria [Figure 2].
The data were reported as the mean, +/- standard deviation or median, depending on their distribution. The individual characteristics of both the scores were statistically grouped using frequency tables. The chi-square test was used to assess differences in categorical variables between groups. The sensitivity and specificity of both scores were calculated. Statistical analysis was performed using SPSS software (version 17).
RESULTS
Our study had 109 patients who underwent Laparoscopic Appendicectomy based on clinical and radiological evidence, of which 68 were male and 41 were female. All patients underwent ultrasound imaging and 58% of them had an equivocal or negative ultrasound report and needed CT scans to confirm the diagnosis of acute appendicitis. On histopathological analysis, 98 patients biopsies were proven to be appendicitis and 11 patients had negative appendectomies. Out of the 98 cases, 41 was reported as acute appendicitis, 24 as appendicitis with periappendicitis, 31 as acute suppurative and 2 as gangrenous appendicitis. Out of the 11 negative appendectomies, 9 were reported as reactive lymphoid hyperplasia and 2 was reported as eosinophilic appendicitis
The cut-off score to diagnose acute appendicitis in Modified RIPASA was fixed at 7.5. The percentage of patients who had a score of above 7.5 in the modified RIPASA was 84.4% (9 2 patients). 17 patients had a score below 7.5, which amounted to 15.6% of the total cases. The cut-off score to diagnose acute appendicitis in ALVARADO was fixed at 7. The percentage of patients who had a score of above 7 in Alvarado was 66.1% (72 patients). 37 patients had a score below 7, which amounted to 33.9% of the total cases.
On evaluating the Modified RIPASA score with the histopathological report in diagnosing appendicitis, the sensitivity is 90.82%, Specificity is 72.73%, Positive predictive value is 96.74%, Negative predictive value is 47.06%, Positive likelihood ratio is 3.33 and Negative likelihood ratio is 0.13. By chi-square test, the P value was 0.000, which is highly significant [Table 3].
On evaluating the ALVARADO score with the histopathological report in diagnosing appendicitis, the Sensitivity is 68.37%, Specificity is 54.55%, Positive predictive value is 93.06%, Negative predictive value is 16.22%, Positive likelihood ratio is 1.50 and Negative likelihood ratio is 0.58. By chi-square test, P-value was 0.128, which is significant [Table 4].
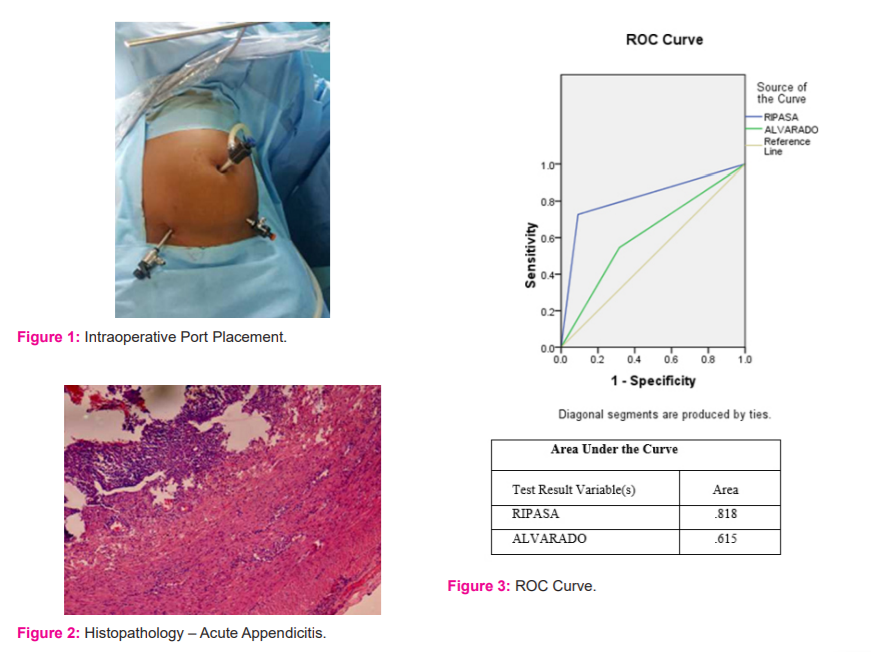
A Receiver Operating Characteristic (ROC) curve showed the area under the ROC curve for RIPASA is significantly higher than Alvarado’s area under the curve [Figure 3]. This signifies that RIPASA has a higher statistical significance in predicting acute appendicitis.
DISCUSSION
Acute appendicitis is essentially a clinical diagnosis with a lifetime risk of approximately one in seven.3 The earlier the diagnosis of acute appendicitis is made the risk of complications can be reduced. On the other hand, overdiagnosis of acute appendicitis could also increase the rate of negative appendectomies. Scoring systems are very useful, especially in equivocal cases that are encountered now and then. Widely used scores like Alvarado, which aid in the diagnosis of acute appendicitis, have been developed in and for a Caucasian population. A new scoring system RIPASA for the Asian population was devised, which was evaluated in this study.
In our study, a total of 109 patients were included. There is a male predominance noted in the incidence of acute appendicitis. There was an incidence of 62.4% in males when compared to a 37.6% incidence in the female population. This increase in male incidence was noted in similar studies such as Chong et al, Cuscheri A et al and other published data.3,6 The mean age noted in our study was 31.05 years. The incidence in various parts of the world like Poland, Turkey and the United States all remain high in this age group of patients.7,8
The entire study population was scored with both Alvarado and Modified RIPASA. The Alvarado score’s cut off was set at a score of 7 and above for a diagnosis of acute appendicitis. This data was analyzed in comparison with the histopathology reports. The sensitivity and specificity were calculated at 68.37% and 54.55% respectively. The positive predictive value was 93.06% and the negative predictive value was 16.22%. The P-value calculated by the Chi-square tests gave a P value of 0.128, which was statistically significant. Nanjundaiah et al. and Hasan et al. reported similar sensitivities and specificities.9,10
As part of the evaluation of acute right iliac fossa pain all the patients included in the study underwent ultrasound examination of the abdomen. In 42% ultrasound showed features suggestive of acute appendicitis. 58% of the patients required CT abdomen to diagnose appendicitis. CT was found to significantly increase the accuracy of diagnosing acute appendicitis, which was similar in comparison to other studies such as Park JS et al.11
The cut off for Modified RIPASA score was set at a score of 7.5 and above. The sensitivity and specificity were calculated at 90.82% and 72.73% respectively. The positive predictive value was 96.74% and the negative predictive value was 47.06%. The P-value calculated by the Chi-square tests gave a P value less than 0.000, which was highly significant. Similar studies like Ravi et al. reported a sensitivity of 84.2% and a specificity of 100% for RIPASA.12
On comparing both the scores the sensitivity and specificity were higher for the Modified RIPASA score. The positive predictive value was higher for Alvarado and the negative predictive value was higher for the Modified RIPASA score. Both P values suggested statistical significance; however, the P-value for Modified RIPASA was highly significant (P < 0.000). This statistical significance is further backed up by the receiver operator curve (ROC) graph, which shows a larger area under the curve for Modified RIPASA (0.818) when compared to Alvarado (0.615).
This study, along with various other quoted articles, suggests that the Alvarado score is not very sensitive in an Asian population as compared to a Western population.13 On the other hand the Modified RIPASA score seems more sensitive and specific in the Asian population.14
The authors who have devised the score suggest it uses many parameters important for the diagnosis of acute appendicitis, such as age, sex and duration of symptoms, which are not present in the Alvarado and Modified Alvarado scores.3 The local inflammatory indicators such as Rovsing’s sign and guarding were also included in the score. The original RIPASA score had scored residential foreigners as one; since our study was based on an Indian population and no foreigners were included we decided to omit the score. This is based on the fact that the diet of the Western population is low in dietary fibre and high in saturated fatty foods. This puts this in a higher incidence of acute appendicitis. Thus the Modified RIPASA was concluded to be a more applicable and useful score in an Indian population.
CONCLUSION
The Modified RIPASA score has shown a promising result in the South Indian population with higher sensitivity and specificity than ALVARADO. The various parameters required in the score can easily be obtained from a simple history and physical examination. In a resource-limited set-up, this score can help us to stratify patients based on the need for further evaluation, thereby reducing unnecessary admissions. The difference in diagnostic accuracy between Modified RIPASA and Alvarado was statistically significant (P value<0.000) in our study.
ACKNOWLEDGEMENT
The authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
CONFLICT OF INTEREST – NIL
SOURCE OF FUNDING – NIL
AUTHOR’S CONTRIBUTION
Manickkam K is responsible for the acquisition of data, analysis and interpretation of data and critical revising of intellectual content. Chandru R contributed to conception, design, writing the article and revising the paper critically. Rajiv Raj D made a substantial contribution in analyzing and interpreting data. Ramya R also made a substantial contribution in design, the conception of the content and revising the paper critically for important intellectual content.
References:
-
Rothrock SG, Pagane J. Acute appendicitis in children: Emergency department diagnosis and management. Ann Emerg Med. 2000; 36(1):39 - 51.
-
Khairy G. Acute appendicitis: Is removal of a normal appendix still existing and can we reduce its rate? Saudi J Gastroenterol. 2009;15(3):167 - 170.
-
Chong CF, Adi MI, Thien A, Suyoi A, Mackie AJ, Tin AS, Tripathi S, Jaman NH, Tan KK, Kok KY, Mathew VV. Development of the RIPASA score: a new appendicitis scoring system for the diagnosis of acute appendicitis. Singap Med J. 2010 Mar 1;51(3):220-25
-
Jang SO, Kim BS, Moon DJ. Application of Alvarado score in patients with suspected appendicitis. Korean J Gastroent. 2008; 52:27-31.
-
Ali R, Khan MR, Pishori T, Tayeb M. Laparoscopic appendectomy for acute appendicitis: Is this a feasible option for developing countries?. Saudi J Gastroent. 2010 Jan; 16(1):25-29.
-
Shirah BH, Shirah HA, Alhaidari WA, Abdulbagi OE. Challenges in the management of subhepatic acute appendicitis in the emergency setting. Int J Curr Res Rev. 2016 Mar 22;15(8):6;47- 52
-
Mohammed A, Shanbhag V, Ashfaque K. A Comparative Study of RIPASA Score and ALVARADO Score in the Diagnosis of Acute Appendicitis. Journal of Clinical and Diagnostic Research?: J Curr Drug Res. 2014;8(11): NC03 -NC05.
-
Naveen K, Sareesh NN, Satheesha BN, Murlimanju BV, Suhani S, Mamatha H, Sampath PK. Appendicitis and appendectomy: A retrospective survey in South Indian population. J Surg Acad. 2013;3(2):10-3.
-
Walczak DA, Pawe?czak D, ?ó?taszek A, Jagu?cik R, Fa?ek W, Czerwi?ska M, Ptasi?ska K, Trzeciak PW, Pasieka Z. The Value of Scoring Systems for the Diagnosis of Acute Appendicitis. Polski przeglad chirurgiczny. 2015 Feb 1;87(2):65-70.
-
Erdem H, Çetinkünar S, Da? K, Reyhan E, De?er C, Aziret M, Bozkurt H, Uzun S, Sözen S, ?rkörücü O. Alvarado, Eskelinen, Ohhmann and Raja Isteri Pengiran Anak Saleha appendicitis scores for diagnosis of acute appendicitis. World J Gastroent. 2013 Dec 21;19(47):9057- 9062.
-
Park JS, Jeong JH, Lee JI, Lee JH, Park JK, Moon HJ. Accuracies of diagnostic methods for acute appendicitis. Amer Surg. 2013 Jan;79(1):101-6.
-
Kumar R. To Evaluate Use of Combined Modified Ripasa Scoring and Ultrasonography to Improve Diagnostic Accuracy in Acute Appendicitis. J Med Sci Clin Res. 2017;5(5):21643-50.
-
Kariman H, Shojaee M, Sabzghabaei A, Khatamian R, Derakhshanfar H, Hatamabadi H. Evaluation of the Alvarado score in acute abdominal pain. Ulus Travma Acil Cerrahi Derg. 2014 Mar 1;20(2):86-90.
-
Malik MU, Connelly TM, Awan F, Pretorius F, Fiuza-Castineira C, El Faedy O, Balfe P. The RIPASA score is sensitive and specific for the diagnosis of acute appendicitis in a western population. Int J Color Dis. 2017 Apr 1;32(4):491-7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





