IJCRR - 13(13), July, 2021
Pages: 129-133
Date of Publication: 05-Jul-2021
Print Article
Download XML Download PDF
A Comparative Study on Mastoidectomy Cavity Obliteration with Soft Tissue Graft and Cartilage Graft in Canal Wall Down Mastoidectomy
Author: Sivasubramanian Thirani, Rajkamal Pandian Durairaj, Radhakrishnan Kailasm Ramamoorthy, Balasubramanian Covindarasu, Sneka Periasamy
Category: Healthcare
Abstract:Introduction: Chronic suppurative otitis media is a long-standing infection of apart or whole of the middle ear cleft characterised by ear discharge. In conditions of Atticoantral type of pathology and cholesteatoma disease clearance from the middle ear cleft, mastoid antrum is done using modified radical mastoidectomy. Aim: This study aims to compare the mastoidectomy cavity obliteration with soft tissue graft and cartilage graft in canal wall down mastoidectomy. Methods: This prospective comparative study on mastoidectomy cavity obliteration with soft tissue graft in 20 patients (Group A) and cartilage graft in 20 patients (Group B) in canal wall down mastoidectomy surgeries conducted on patients diagnosed with chronic suppurative otitis media of atticoantral pathology. Postoperative outcome was compared between 2 groups. Results: The outcome showed that the patients obliterated with cartilage showed a faster rate of epithelialization and formation of the dry cavity when compared to patients obliterated with soft tissue with a statistically significant difference (Pvalue=0.003). There was a gradual decrease in ear discharge in Group A patients compared to Group B at the end of the third month with a significant statistical difference (Pvalue=0.046); however, there was no statistical difference by the end of the sixth month. There was no statistically significant difference in the postoperative hearing in terms of the Air-bone gap between the groups. Conclusion: From this study, we concluded that obliteration with cartilage provided much better results regarding the cavity's epithelialization, thereby forming dry ear at a faster rate both statistically and clinically, along with good anatomical configuration than soft tissues.
Keywords: Mastoidectomy, Cholesteatoma, Suppurative, Cartilage, Mastoid cavity, Obliteration
Full Text:
INTRODUCTION
Chronic suppurative otitis media is a prolonged standing infection of a part or whole of the middle ear cleft, characterised by ear discharge. There are two types of chronic suppurative otitis media: Tubotympanic type/ Mucosal ear and Atticoantral type/ Squamous type. From a historical point of view, Moscher1was the first to introduce this concept in 1911, ever since many obliteration techniques are in practice using different obliteration materials. These include soft tissues (muscle pedicled flaps, muscle, fascia), Cartilages (autogenous conchal, tragal cartilage), hydroxyapatite crystals, glass isomers, ceramides.1 Various material have been used for obliteration, which is divided into two categories as free grafts (biologic and non-biologic); such as cartilage, fat tissue, fascia, hydroxyapatite crystals, and local flaps; such as Palva flap (musculoperiosteal flap), temporoparietal fascia flap, and postauricular myocutaneous flap.2-8Different materials and techniques are in vogue in the present scenario, and the merits and demerits of each of these techniques are still under research.
Atticoantral type/ Squamous type involves attic, antrum, mastoid, associated with bone eroding, such as cholesteatoma, granulations, and osteitis. This type is more prone to complications. In cholesteatoma cases, surgical intervention is mandatory wherein we prefer Canal wall down mastoidectomy procedures, otherwise called Modified radical mastoidectomy. This procedure provides complete clearance of the disease, thereby leaving behind a wide, open mastoid cavity. However, the creation of a wide cavity is associated with Chronic discharging problems from the cavity. Collection of debris. In this surgical procedure, the disease is eradicated from the middle ear cleft, followed by conversion of mastoid cavity, middle ear, external auditory canal into a single smooth self-cleansing cavity exteriorised through the external auditory canal, leaving behind healthy tissues for future reconstruction.9 Complication of chronic otitis media includes direct bony erosion, acute mastoiditis, petrositis, facial paralysis, labyrinthitis, meningitis, brain abscess and thromphobhebitis. Our study compares mastoidectomy cavity obliteration with soft tissue graft (temporalis muscle pedicled flap, temporalis muscle fascia, temporalis muscle) and cartilage graft (autogenous conchal and tragal cartilage) and their postoperative outcomes.
AIM
This study compares the mastoidectomy cavity obliteration with soft tissue graft and cartilage graft in canal wall down mastoidectomy.
MATERIALS AND METHODS
This study comprised 40 patients who attended the ENT department, Thanjavur Medical College Hospital, Thanjavur, from November 2018 to September 2019. Ethical committee approval was received (EC/approval no.580/2018). Patients were diagnosed to have chronic suppurative otitis media of Atticoantral pathology by clinical history and otoscopic examination. Exclusion criteria include Chronic suppurative otitis media - Tubotympanic type (safe type), Chronic suppurative otitis media -Intracranial complication, age less than five years, pregnant and lactating mothers. Informed and written consent was obtained before proceeding with the surgery. The patients underwent the following evaluation like History taking, General examination, Systemic examination, ENT examination, Specific investigations like Aural swab culture and sensitivity, Tuning fork test, X-ray both mastoids, pure tone audiometry, CT temporal bone and Examination under the microscope, Nonspecific investigations like Complete haemogram, Urine analysis and Blood sugar, urea, serum creatinine and assessment of the patient for general anaesthesia.
The 40 patients included in our study underwent Canal wall down mastoidectomy procedure after their fitness for surgery was ensured. They were divided into two groups, each containing 20 patients. Cartilage graft was used for 20 patients (Group A), and soft tissue was used for the remaining 20 patients for obliteration (Group B). Autogenous Conchal cartilage and tragal cartilage, temporalis muscle pedicled flap, temporalis muscle fascia were the graft materials used for obliteration.
Postoperatively the patients were treated with intravenous antibiotics, analgesics, anti-inflammatory drugs. One week after the procedure, mastoid bandage, postauricular sutures were removed, and ear canal pack and discharged. Advised to review at ENT op at corresponding interval seven days. They were given steroid ear drops for two weeks and vinegar with normal saline (1:4) for the next four weeks to ensure average PH balance and proper epithelialisation. The patients were followed up regularly at the second, third, sixth month, respectively. By the end of the third month, the patients were subjected to Puretone audiometry. The postoperative outcomes were compared between the two groups.
RESULTS
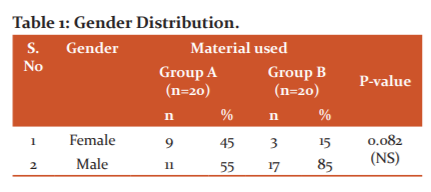
Out of 40 patients, 20 patients included in Group A and 20 patients included in Group B. In Group A, 9 patients were females, and 11 were males. In Group B, 3 cases were females, and 17 were males. (Table 1)
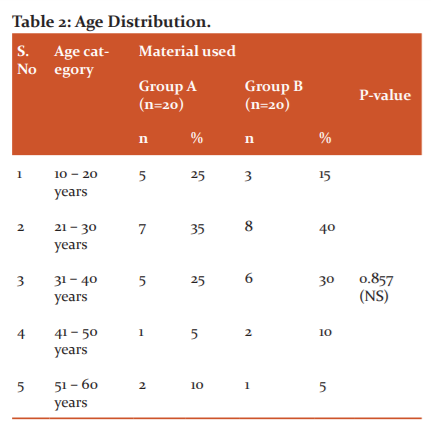
Out of 40 patients, 20 patients included in Group A and 20 patients included in Group B. In Group A 5 were in the age group between 10-20years, 7 patients between 21-30 years, 5 were in age between 31-40 years, 1 patient between 41-50 years and 2 patients between 51-60 years. In Group B 3 were in the age group between 10-20years, 8 patients between 21-30 years, 6 were in age between 31-40 years, 2 patients between 41-50 years and 1 patient between 51-60 years. (Table 2).
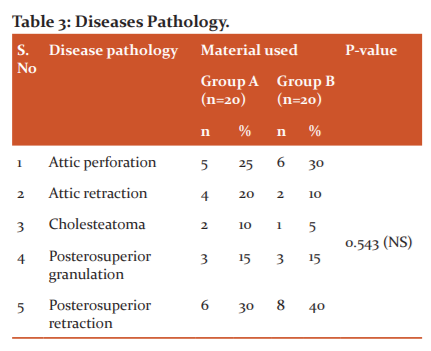
Out of 40 patients, 20 patients included in Group A and 20 patients included in Group B. In Group A, five patients had attic perforation, 4 patients had attic retraction, 2 patients had cholesteatoma, 3 patients had posterosuperior granulation, and 6 patients had posterosuperior retraction. In Group B, 6 patients had attic perforation, 2 patients had attic retraction, 1 patient had cholesteatoma, 3 patients had posterosuperior granulation, and 8 patients had posterosuperior retraction. (Table 3)
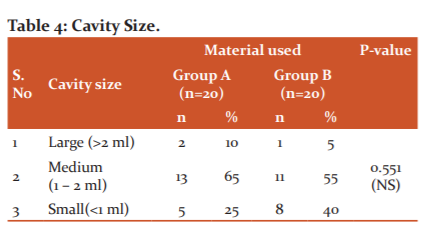
Out of 40 patients, 20 patients included in Group A and 20 patients included in Group B. In Group A, 2 patients had a large cavity, 13 patients had a medium cavity, and 5 patients had a small cavity. In Group B 1 patient had a large cavity, 11patients had a medium cavity, and 8 patients had a small cavity. (Table 4)
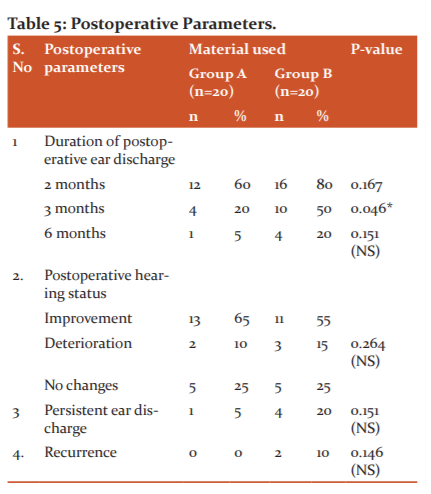
Out of 40 patients, 20 patients included in Group A and 20 patients included in Group B. In Group A, based on the duration of postoperative ear discharge, 12 patients had 2 months, 4 patients had 3 months, 1 patient had 6 months, based on postoperative hearing status improvement seen in 13 patients, 2 patients had deterioration, 5 patients had no changes, 1 patient had persistent ear discharge. In Group B based on the duration of postoperative ear discharge, 16 patients had 2 months, 10 patients had 3 months, 4 patients had 6 months, based on postoperative hearing status improvement seen in 11 patients, 3 patients had deterioration, 5 patients had no changes, 4 patients had persistent ear discharge, and 2 patients had a recurrence. (table 5)
DISCUSSION
There were previous studies where different materials were used for obliteration. A retrospective study was conducted on 30 patients regarding mastoidectomy cavity obliteration using Conchal cartilage from May 2014 to January 2017 in Al- Sulaimania city in Iraq. Their patients showed complete epithelialization at the end of the follow-up period. The mean Air-bone gap was 42.2dB +/-10.8, preoperatively that became 27.4dB (+/-12.9) with p-value <0.05. Finally, obliteration of the cavity with conchal cartilage was proven to be an effective technique in canal wall downprocedures.10
Another study was published in the year2012, a retrospective study with 56 patients diagnosed with chronic suppurative otitis media of Atticoantralpathology and underwent canal wall down procedure. Mastoid cavities were obliterated with Conchal cartilage graft and temporalis muscle fascia graft after being sorted into two groups, and postoperative results were observed. A completely dry cavity was achieved in 49 patients out of 56(approx. 88%, 95% confidence interval 77-95%). An overall statistically improved hearing (P < 0.05) was obtained, with the mean pure-tone average air-bone gap decreasing from 33.4+/-8.2 dB (average +/- SD) to 18.3 +/- 9.7Db.It was concluded that both the Group of patients obtained the benefit of obliteration, but still, there were better results in patients obliterated with conchal cartilage.11
A study was published in Andhra Pradesh in 2016, a prospective study with 100 patients of atticoantral pathology subjected to canal wall down mastoidectomy. Their mastoid cavities were obliterated with conchal cartilage, and postoperative results observed. A completely dry cavity was observed in nearly 80-85% of the patients with an overall improvement in hearing and the mean preoperative and the postoperative Air-bone gaps were 29.2 +/- 13.5Db and 25+/-15.4 dB. There was a reduced incidence in discharge and a faster rate of epithelialization with this technique. Thus usage of conchal cartilage was considered to be the best material in mastoid cavity obliteration procedures.12
In the study done by Walker et al., ABG improved to 23.4dB from 27.8dB, 13% recidivism of cholesteatoma second-look ossiculoplasty.13
To the removal of cholesteatoma, Kronenberg et al. removed the posterior canal wall during mastoidectomy and reimplanted the canal wall again.12% of recurrent cholesteatoma noted in all ears by non-EPI diffusion-weighted MRI.14
Harris et al. found that in CWD mastoidectomy, the frequency of ear discharge was greater (27%) than in CWU mastoidectomy (3.3%). In contrast, the reconstruction of the meat wall occurred in 9.7% of the ears.15
The patients placed under group A - cartilage variety showed a faster rate of epithelialization when compared to group B – Soft tissue and the difference was found to be statistically significant with a value of 0.0032(P< 0.05). Patients under Group A also showed a good and a gradual decrease in ear discharge when compared to Group B by the end of the third month with a significant difference of 0.046 (P<0.05), however by the end of six months, there was no statistical significance though the results were clinically in favour of group A (cartilage).
There was an improvement in postoperative hearing in Bone Gap in group A patients; however, 10 patients in both groups did not show any significant improvement. At the end of six months, there were 5 patients with persistent ear discharge, 1 (5%) belonged to Group A, 4(20%) belonged to Group B.Out of the 2 (10%) patients in GroupB had granulation tissue along with foul-smelling ear discharge that needed to be repeated follow-ups and examination. The remaining two patients of Group B and the remaining one patient in Group A developed wax in due course of time. There was an overall improvement in hearing in terms of the Air-Bone gap clinically, though the comparison between the two materials did not show any significant difference statistically.
At the end of the study, patients under group A (cartilage) showed a faster rate of epithelialization and a more rapid rate formation of dry cavity compared to group B with a statistically significant difference, which appears to be the primary purpose of this cavity obliteration study. Other parameters were found to have a similar impact statistically on both groups.
CONCLUSION
To conclude, obliteration with cartilage provided much better results regarding the epithelialization of the cavity, thereby forming dry ear at a faster rate both statistically and clinically, along with good anatomical configuration than soft tissues. However, the other criteria were statistically similar to both groups.
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references to this manuscript.
Conflict of interest: Nil
Financial support: No
References:
-
Mosher HP. A method of filling the excavated mastoid with a flap from the back of the auricle. Laryngoscope . 1911 Dec 21(12):1158-63.
-
PalvaT. Cholesteatoma surgery today. Clin. Otolaryngol. 1993 Aug 18(4):245-52.
-
Hung T, Leung N, van Hasselt CA, Liu KC, Tong M. Long?term Outcome of the Hong Kong Vascularized, Pedicled Temporalis Fascia Flap in Reconstruction of Mastoid Cavity. Laryngoscope. 2007 Aug;117(8):1403-7.
-
Kaur N, Sharma DK, Singh J. Comparative evaluation of mastoid cavity obliteration by vascularised temporalis myofascial flap and deep temporal fascial-periosteal flap in canal wall down mastoidectomy. J Clin Diagn Res J Clin Diagn. 2016 Dec;10(12):MC08.
-
Olson KL, Manolidis S. The pedicled superficial temporalis fascial flap: a new method for reconstruction in otologic surgery. Otol Head Neck Surg. 2002 May 1;126(5):538-47.
-
Abramson M. Open or closed tympanomastoidectomy for cholesteatoma in children. Otol Neurotol. 1985 Mar 1;6(2):167-9.
-
Kahramanyol M, Özünlü A, Pabusçu Y. Fascioperiosteal flap and neo-osteogenesis in radical mastoidectomy: long-term results. Ear Nose Throat J. 2000 Jul;79(7):524-6.
-
Jo SY, Eom TH, Yang HC, Cho YB, Jang CH. Comparison of obliteration materials used for revision canal wall-down mastoidectomy with mastoid obliteration. J In vivo Laryngoscope. 2014 Nov 1;28(6):1207-12.
-
Lee HJ, Chao JR, Yeon YK, Kumar V, Park CH, Kim HJ, Lee JH. Canal reconstruction and mastoid obliteration using floating cartilages and mucoperiosteal flaps. Laryngoscope. 2017 May;127(5):1153-60.
-
Al-Tayyar M, Baban M, Khdhayer A, Najeeb R, Othman S. The Efficacy of Mastoid Cavity Obliteration by Conchal Cartilage in Canal Wall Down Mastoidectomy. J Otolaryngol Res 1: 103.
-
Maniu A, Cosgarea M. Mastoid obliteration with concha cartilage graft and temporal muscle fascia. ORL J Otorhin Relat Spec. 2012;74(3):141-5.
-
Chhapola S, Matta I. Mastoid obliteration versus open cavity: a comparative study. Indian J Otolaryngol Head Neck Surg. 2014 Jan 1;66(1):207-13.
-
Walker PC, Mowry SE, Hansen MR, Gantz BJ. Long-term results of canal wall reconstruction tympanomastoidectomy. Otol Neurotol. 2014 Jul 1;35(6):954-60.
-
Kronenberg J, Shapira Y, Migirov L. Mastoidectomy reconstruction of the posterior wall and obliteration (MAPRO): preliminary results. Acta Otolaryngol. 2012 Apr 1;132(4):400-3.
-
Harris AT, Mettias B, Lesser TH. Pooled analysis of the evidence for an open cavity, combined approach and reconstruction of the mastoid cavity in primary cholesteatoma surgery. J Laryngol Otol. 2016 Mar 1;130(3):235.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





