IJCRR - 13(13), July, 2021
Pages: 08-12
Date of Publication: 05-Jul-2021
Print Article
Download XML Download PDF
Adhesive Capsulitis in Diabetes Mellitus - An Observational Study
Author: Neha Mukkamala, Jitendra Lakhani, Lata Parmar
Category: Healthcare
Abstract:Background: Shoulder problems are the most disabling manifestation of musculoskeletal disorders in diabetes. Patients with diabetes are five times more likely to develop capsulitis compared to non-diabetic controls. Aim: The present study aimed to see the prevalence of adhesive capsulitis in patients with diabetes. Methodology: This was a cross-sectional study approved by the Institution Ethics Committee. Patients diagnosed with type I and type II diabetes, aged 18 years and above, having a complaint of shoulder pain (unilateral or bilateral) were included in the study. Those patients who had undergone surgeries, fractures around the involved shoulder and any neurological conditions of the upper limb were excluded. Demographic data, duration of diabetes, dominance, type of treatment for diabetes were taken for all the patients. Shoulder ranges and functional activities were assessed in detail. Results: A total of 243 patients with diabetes was enrolled in the study. 116 (47.74%) were females, 127 (52.26%) were males. Out of 243 patients with diabetes, 22 patients had adhesive capsulitis. The prevalence of adhesive capsulitis was 9.1%. A sig�nificant correlation (p< 0.05) was seen between adhesive capsulitis and the duration of diabetes. No significant correlation was found between adhesive capsulitis and age, gender, BMI, HbA1c, dominance and type of treatment (oral hypoglycemic, insulin or both). Conclusion: The prevalence of adhesive capsulitis in patients with diabetes was 9.1%. A significant correlation (p< 0.05) was seen between adhesive capsulitis and the duration of diabetes.
Keywords: Adhesive capsulitis, Diabetes mellitus, Frozen shoulder, Periarthritis, Hyperglycemia
Full Text:
INTRODUCTION
India, with 65 million cases of diabetes, stands second only to China worldwide in the number of cases with diabetes.1Musculoskeletal complications in diabetes are not very widely known.2
The hand and shoulder are the most commonly affected areas due to musculoskeletal complications in diabetes.3,4Shoulder problems are described as the most disabling manifestation of musculoskeletal disorders.5,6Several studies have shown the prevalence of adhesive capsulitis (AC)in diabetes to be around 10-30%, and 2-5% in the general population.5,7-13A meta-analysis by Zreik et al (2016) has shown that patients with diabetes are five times more likely to develop capsulitis compared to non-diabetic controls. In the same study, the mean prevalence of diabetes mellitus in patients with AC was found to be 30%.9
Thus the present study aimed to know the prevalence of adhesive capsulitis in diabetes.
METHODOLOGY
This was a cross-sectional study that was approved by the Institutional Ethics Committee (Ethical clearance letter no: SVIEC/ON/205/15008). After taking a written informed consent, consecutive patients diagnosed with type I and type II diabetes, aged 18 years and above, who complained of shoulder pain (unilateral or bilateral) were approached to take part in the study. Patients with a history of surgery around the shoulder, rotator cuff tear, fractures of the upper limb on the involved side in the past one year, patients having radiating pain from the neck, rheumatoid arthritis, arthritis of glenohumeral joint and neurological deficits were excluded. The patients who gave written consent for inclusion in the study were assessed in detail.
Demographic features including age, gender and body mass index (BMI) were taken. Diabetes-related questions like a method of control (diet, oral hypoglycemic drugs or insulin) and duration of diabetes were taken. The dominance of the hand was noted. Adhesive capsulitis was confirmed as shoulder pain along with loss of active and passive range of the shoulder in the absence of a known shoulder disorder. Shoulder ranges were assessed with a goniometer and functional activities like combing the hair, taking the hand behind the back, wearing clothes were assessed.
Statistical analysis
Baseline characteristics are presented as means with standard deviation (SD), medians with range. Normality of the data was seen using the Shapiro Wilk test. As the data was non-parametric, Spearman’s correlation coefficient and Mann Whitney U test were performed. Statistical significance was kept at p < 0.05.
RESULTS
A total of 243 patients with diabetes was enrolled in the study.116 (47.74%) were females, 127(52.26%) were males.
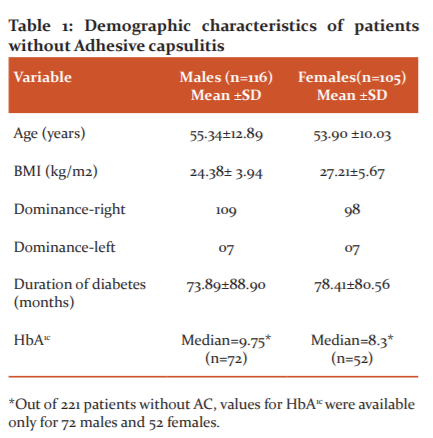
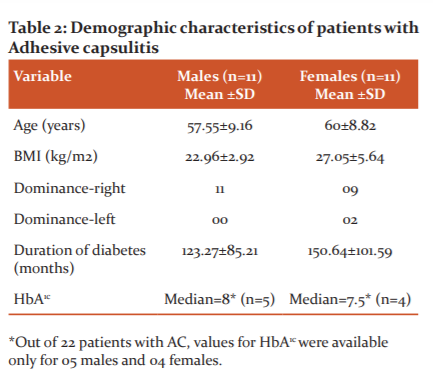
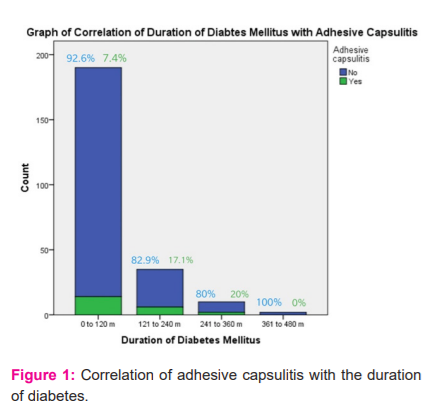
Out of 243 patients with diabetes, 22 patients had adhesive capsulitis. The prevalence of adhesive capsulitis was 9.1%. Tables 1 and 2 show the demographic characteristics of patients without and with adhesive capsulitis respectively. Table 3 compares the different variables in patients with diabetes mellitus, with and without Adhesive capsulitis. Figure 1 shows the correlation of adhesive capsulitis with the duration of diabetes.
The duration of capsulitis varied from 01 months to 03 years in the present study. The most affected ranges were external rotation (average range-150) and abduction (average range-1000). All patients complained of more pain during overhead activities like combing with the affected side which involves a combination of flexion, abduction and external rotation at the shoulder and wearing clothes with the uninvolved side first. Women complained of more pain in bringing the saree from behind which involves a combination of extension, adduction and internal rotation of the shoulder and men had more pain in removing the wallet from the back pocket which also involves the combination of extension, adduction and internal rotation.

DISCUSSION
The present study was undertaken to know the prevalence of adhesive capsulitis in patients with diabetes. The prevalence of adhesive capsulitis was found to be 9.1% in the present study, which is slightly lower than the prevalence in other Indian states: Mathew et al. -16.45%, 14Bhat et al.-13.1%, 15Gupta et al.-29.61%, 16Kumar et al.-45.31%. 17The prevalence of capsulitis in other countries was:Yian et al.- 0.65 %, 18Ramchurn et al.-25%, 19Majjad et al.-12.5%, 20Kidwai et al.-10.9%, 21Hassan et al.-13%, 22Attar S-6.7%. 23Fasika et al. found a 16.6% cumulative prevalence of hand and shoulder disorders, 24and Shah et al. found a 63% prevalence of shoulder pain and/or disability. 25Lower prevalence in our study could be because most of the population (70% in the present study) that comes to our hospital comes from the villages in and around Vadodara as well as rural areas of the neighbouring state of Madhya Pradesh. The prevalence of diabetes is lesser in rural areas compared to urban areas. 6,26
The prevalence of capsulitis in diabetes can be attributed to the high glucose levels in patients with diabetes which leads to 1) abnormal collagen deposition in the connective tissues and 2) an increase in advanced glycation end products (AGEs), which causes stiffness of connective tissue. 3,4,27
All 22 patients with AC had type 2 diabetes. Capsulitis was present in 08 patients on the left side, 10 patients on the right side and bilaterally in 04 patients. 12,27Sixty four per cent had it on the dominant side and 36% had on the non-dominant side. This shows more involvement on the dominant side which is similar to Gupta et al’s study16and contrary to Le et al’s study. 10 Also 81.8% had unilateral involvement which is consistent with other studies.6,27
A significant correlation was found between AC and duration of diabetes showing that patients with AC had a longer duration of diabetes. The prevalence of AC was 7.4%, 17.1%, 20% and 0% in patients with duration of diabetes of 10 years, 20 years, 30 years and 40 years. This is in agreement with several studies.12,18,22According to Yian et al. (2012) patients whose treatment for diabetes lasted longer than 10 years had an odds ratio of 1.85 to develop AC vs an odds ratio of 1.40 for those with 5-10 years of treatment.18Inayat et al. did not find a correlation with the duration of diabetes. 6 However the number of patients with diabetes and with or without capsulitis in all the groups was not similar.
There was no significant correlation seen between AC and age and BMI.6,12Arkkila et al. showed a significant correlation between age and AC but not between BMI and AC. 28
Also, no significant correlation was seen between AC and gender, both genders were equally affected. 12According to some studies, females are,1.27 to 2.66 times, more commonly affected than males.6,9,18
None of the three patients with type 1 diabetes had capsulitis. This could probably be because all three of them were young (<37 years) and their duration of diabetes ranged from 1.5 months to 4 years which was very less. Doria et al (2017) and Arkkila et al. (1996) have shown an association of age and duration of diabetes with AC in type 1 diabetes.12,28
There was no significant relationship between glycated haemoglobin (HbA1c) and the prevalence of AC. Previous studies have also shown no correlation between AC and HbA1c.11,12,18,28According to Chan et al. singular HbA1cis only a measure of short-term blood sugar control, reflecting an average of only 3 months’ disease which might not portray total diabetic disease burden.11
In the present study, out of 22 patients with AC, 05 patients were on insulin, 14 were on oral hypoglycemic drugs and 03 were on a combination of drugs and insulin. There was no significant correlation seen between the type of treatment for diabetes (medications, insulin or both) and AC which is in agreement with several studies.9These findings are in contrast to Yian et al’s (2012) findings that patients on insulin along with or without oral hypoglycemics were 1.93 times more likely than those not on insulin to have AC. 18Those on oral hypoglycemic drugs were1.5 times more likely to develop AC than those who did not take oral hypoglycemic drugs or use insulin.6,18
One of the limitations of the present study was that HbA1c was not taken for all the patients. But studies say that HbA1c is not a true marker for diabetes as it gives only average values of the past three months. Also, it is an expensive test. It is not possible to test all patients with diabetes with this.
CONCLUSION
Screening for adhesive capsulitis in patients with diabetes should be done by physicians/diabetologists. Awareness and education about AC should be created in all patients with diabetes so that an earlier diagnosis and treatment may prevent progression to chronic, treatment-resistant AC and improve the quality of life. Screening, prevention, and rehabilitation strategies for shoulder dysfunction should be included in diabetic care programs.
ACKNOWLEDGEMENTS: The authors are grateful to the patients who participated in the study as well as Sumandeep Vidyapeeth trust.
CONFLICT OF INTEREST: The authors declare no conflict of interest.
FUNDING: This was a self-funded project.
AUTHORS’ CONTRIBUTION
Neha Mukkamala- 1) conception and design, analysis and interpretation of data; 2) drafting the article, revising it critically for important intellectual content; and 3) final approval of the version to be published.
Dr Jitendra Lakhani- 1) conception and design 2) revising the article critically for important intellectual content; and 3) final approval of the version to be published.
Dr Lata Parmar- 1) drafting the article, revising it critically for important intellectual content; and 2) final approval of the version to be published.
References:
1. Ramachandran A, Snehalatha C, Wan Ma R. Diabetes in South-East Asia: An update. Diab Res Clin Pract. 2014; 103:231-237.
2. Merashli M, Chowdhury TA, Jawad AS. Musculoskeletal manifestations of diabetes mellitus. Quant J Med. 2015; 108 (11): 853–857.
3. Smith L, Burnet S, McNeil J. Musculoskeletal manifestations of diabetes mellitus. Br J Sports Med 2003; 37:30–35.
4. Kaka B, Maharaja S, Fatoye F. Prevalence of musculoskeletal disorders in patients with diabetes mellitus: A systematic review and meta-analysis. J Back Musculosk Rehab. 2018; 1:1-13.
5. Tighe C, Oakley W. The Prevalence of a Diabetic Condition and Adhesive Capsulitis of the Shoulder. Sout Med J. 2008; 101 (6): 591-595.
6. Inayat F, Ali N, Shahid H, Younus F. Prevalence and Determinants of Frozen Shoulder in Patients with Diabetes: A Single Center Experience from Pakistan. Cureus. 2019; 9(8): e1544.
7. Hsu J, Anakwenze O, Warrenderb W, Abboud J. Current review of adhesive capsulitis. J Shoul Elbow Surg. 2011; 20: 502-514.
8. Whelton C, Peach C.Review of diabetic frozen shoulder. Eur J Orthop Surg. 2018; 28(3):363-371.
9. Zreik N, Malik R, Charalambous C. Adhesive capsulitis of the shoulder and diabetes: a meta-analysis of prevalence. Muscles, Lig Tend J. 2016;6 (1):26-34.
10. Le H, Lee S, Nazarian A, Rodriguez E. Adhesive capsulitis of the shoulder: a review of pathophysiology and current clinical treatments.Shoul Elbow. 2017; 9(2): 75–84.
11. Chan J, Ho B, Alvi H, Saltzman M, Marra G. The relationship between the incidence of adhesive capsulitis and haemoglobin A1c. J Shou Elbow Surg. 2017; 26 (10):1834-1837.
12. Doria C, Mosele G, Badessi F, Puddu L, Caggiari G. Shoulder Adhesive Capsulitis in Type 1 Diabetes Mellitus: A Cross-Sectional Study on 943 Cases in Sardinian People. Joints 2017;5:143–146.
13. Austin D, Gans I, Park M, Carey J, Kelly J. The association of metabolic syndrome markers with adhesive capsulitis. J Shoulder Elbow Surg 2014; 23(7):1043-1051.
14. Mathew A, Nair J, Pillai S. Rheumatic-musculoskeletal manifestations in type 2 diabetes mellitus patients in south India. Int J Rheum Dis. 2011; 14: 55–60.
15. Bhat T, Dhar S, Dar T, Naikoo M, Naqqash M, Bhat A, et al. The Musculoskeletal Manifestations of Type 2 Diabetes Mellitus in a Kashmiri Population. Int J Health Sci Qassim Univ. 2016;10 (1): 57-68.
16. Gupta S, Raja K, Manikandan N. Impact of adhesive capsulitis on quality of life in elderly subjects with diabetes: A cross sectional study.Int J Diabetes Dev Ctries. 2008; 28(4): 125–129.
17. Kumar T, Das A. Rheumatological Manifestations in Diabetes Mellitus: Distribution And Associated Factors (2016).http://iosrjournals.org/iosr-jdms/papers/Vol15-Issue%206/Version-9/K1506095154.pdf. 10.9790/0853-1506095154
18. Yian E, Contreras R, Sodl J. Effects of Glycemic Control on Prevalence of Diabetic Frozen Shoulder.J Bone Joint Surg Am. 2012;94:919-23..
19. Ramchurn N, Mashamba C, Leitch E, Arutchelvam V, Narayanan K, Weaver J, Hamilton J, Heycock C, Saravanan V, Kelly C. Upper limb musculoskeletal abnormalities and poor metabolic control in diabetes. Eur J Int Med. 2009;20: 718–721.
20. Majjad A, Errahali Y, Toufik H, Djossou J, Ghassem M, Kasouati J, Maghraoui A. Musculoskeletal Disorders in Patients with Diabetes Mellitus: A Cross-Sectional Study. Int J Rheum. 2018;23(19): 1-6.
21. Kidwai S, Wahid L, Siddiqi S, Khan R, Ghauri I, Sheikh I. Upper limb musculoskeletal abnormalities in type 2 diabetic patients in low socioeconomic strata in Pakistan. BMC Res Notes 2013; 6:16.
22. Hassan R, Alourfi Z. Shoulder adhesive capsulitis prevalence among patients with type 2 diabetes mellitus in Damascus, Syrian Arab Republic: a case-control study. East Mediterr Health J. 2014;19(3): S19-24.
23. Attar S. Musculoskeletal manifestations in diabetic patients at a tertiary centre. Libyan J Med. 2012; 7 (1): 19162.
24. Fasika S, Abebe S, Kebede A. The prevalence of shoulder and hand complications and associated factors among diabetic patients at University of Gondar Teaching Referral Hospital in Northwest Ethiopia. J Diab Res Clin Metab.2013; 41(6):2-8.
25. Shah K, Clark B, McGill J, Mueller M. Upper extremity impairments, pain and disability in patients with diabetes mellitus. Physioth. 2015; 101(2): 147–154.
26. Mohan V, Bhansali A, Yajnik CS, Dhandhania VK, Joshi S, Joshi P. ICMR INDIA Diabetes (INDIAB) study, Phase I final report (2008-2011). Available at [https://main.icmr.nic.in/sites/default/files/reports/ICMR_INDIAB_PHASE_I_FINAL_REPORT.pdf] Last accessed 23rd August,2020 8 am.
27. Moin Uddin M, Khan A, Haig A, Kafil Uddin M. Presentation of frozen shoulder among diabetic and non-diabetic patients. J Clin Orthopaed Traum. 2014; 5(4): 193-198.
28. Arkkila PE, Kantola IM, Viikari JS, Ronnemaa T. Shoulder capsulitis in type I and II diabetic patients: association with diabetic complications and related diseases. Ann Rheum Dis. 1996;55:907-914.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





