IJCRR - 13(12), June, 2021
Pages: 215-219
Date of Publication: 22-Jun-2021
Print Article
Download XML Download PDF
Utilization of Biodentine in Apexification Combined with Large Periapical lesions in Root Canal Treated Teeth- A Case Report
Author: Suruchi Agrawal, Anshul Arora, Mandeep S Grewal, Ashtha Arya
Category: Healthcare
Abstract:Background: The treatment of open apices in non-vital permanent teeth is done with apexification using various materials like MTA, Biodentine and other materials. This study aimed to assess the utilization of Biodentine in apexification and large periapical lesions. Material and Methods: A male patient with the chief complaint of pain and pus discharge in the upper front tooth region. Initially, the patient was asymptomatic but eventually developed periodic swelling. On intraoral examination, it revealed the presence of porcelain fused to the metal crown in the right maxillary central and lateral incisor along with a sinus tract in the periapical region. During percussion of the tooth, it manifests positive tenderness. On radiographic examination, it shows that the root canal was incompletely obturated in both the incisors with incomplete root formation seen in the central incisor. The treatment protocol for tooth 11 and 12 was to perform root canal treatment along with apical plug formation using Biodentine. Therefore, under rubber dam access cavity was prepared and biomechanical preparation was done along with standard disinfection protocol using activation method and given intracanal medicaments. After 2-3 sittings of medicament, the apical plug formation was done in 11 along with filling of rest of the root canal with resin material. Results: In this case report the appreciating healing was seen at 3 months and 1 year follow up. Conclusion: The non-surgical conservative approach used in this case seems to be highly effective and gave astonishing results with complete healing of periapical lesion in central incisors
Keywords: Biodentine, ParaCore, Periapical lesions, Open Apices, Retreatment, Triple Antibiotic Paste
Full Text:
Introduction
Endodontic lesions of teeth with pulpal necrosis and periapical periodontitis is having polymicrobial nature with heightened levels of gram-negative anaerobic endodontic bacteria. These pathogens eventually disseminate from the canal system and exit through root foramen to succeed in the bone surface. The success of endodontic therapy relies on the entire eradication of bacterial infection from in and around the root canal of the teeth.1Interrupted root development, incomplete root formation, results in open apices of the tooth.2
Irrigants are preferred for effective reduction of intraarticular microorganisms and also to eliminate the smear layer, particularly during apexification. NaOCl was employed in clinical studies as the most effective irrigant which is followed by 17% EDTA.3
The complete biomechanical debridement of the root canal accompanied by the placement of an intracanal medicament to initiate apical healing and the formation of an apical barrier in a root with an open apex is mainly involved in apexification.4 Historically, several materials have been advocated as biologic activators to induce apexification, and calcium hydroxide (CH) has been reported as the material of choice because of its favourable properties.2,5
Conversely, a clinician has got to face several challenges when operating the conventional endodontic treatment in open apices teeth, mainly when trying to establish an apical seal in the absence of a complete root apex formation. A fallible apical seal can increase the plausibility of persistent leaky margins and subsequent non-healing or recurrence of periapical lesions. Due to certain disadvantages of using calcium hydroxide as an apical barrier and long duration treatment protocol, new materials were introduced to reduce the treatment time and improve the success of the procedure. It uses nonsurgical condensation of a biocompatible material within the apical third of the canal as an artificial barrier against which root canal filling material can be immediately placed.
In past decades, Mineral trioxide aggregate (ProRootMTA; Dentsply Tulsa, Johnson City, TN, USA) has successfully qualified to be a gold standard and also a huge acceptance in apexification procedures.6 Recently, another calcium silicate-based material, Biodentine (Septodont, Saint-Maur-des-Fosses, France), has been introduced with advantages of a shorter setting time; improved mechanical properties like compressive strength, push-out bond strength, and hardness; and easier handling when compared with MTA.7However, only some case reports exist regarding the clinical application of Biodentine.8 Therefore, in this study the assessment of Biodentine in apexification combined with additional nonsurgical measures in root canal treated tooth for managing concomitant open root apices and large periapical/cystic lesions.
Material & Methods
A 35-year-old male patient presented to the Dept. of Conservative Dentistry and Endodontics of SGT Dental College, SGT University, Gurugram with a chief complaint of pain and pus discharge in the upper front tooth region. He had incurred trauma to the teeth due to a fall from a staircase 10-years ago and underwent endodontic treatment followed by crown 1 year ago as the patient was symptomatic. The patient was asymptomatic for some time but eventually developed periodic swelling and from few months had noticed intermittent pus discharge.
Intraoral examination revealed the presence of porcelain fused to the metal crown in the right maxillary central (11) and lateral incisor (12) associated with a sinus tract in the periapical region (Fig1). Tracing of the sinus tract with gutta-percha confirmed the involvement of both the incisor. The tooth was tender on percussion and palpation. The periodontal status was normal with no mobility ruling out any periodontal pathology. On radiographic examination of both incisors, it revealed that the root canal was incompletely obturated with incomplete root formation in 11 also having periapical radiolucency (Fig 2).
Electric and thermal tooth vital testing was performed and central and lateral incisors gave a negative response and all the other teeth show a positive response.
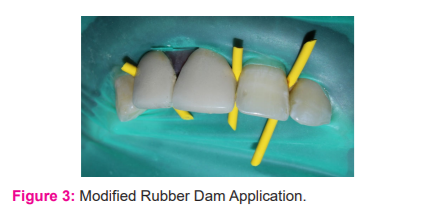
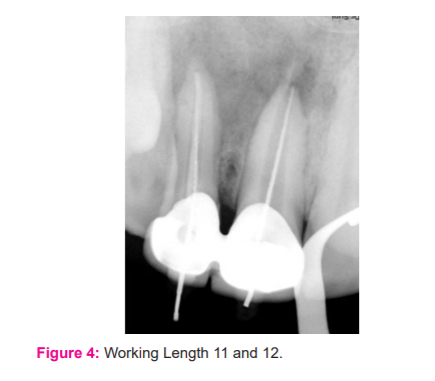
The tooth was anaesthetized with 2% lidocaine with 1:100000 adrenaline. Under the modified rubber dam technique, the access cavity was prepared through the crown in tooth 11 and 12 (Fig 3). Straw coloured fluid discharge was seen from the canal with a foul smell. Gutta-percha removal was carried out with H-files. Working length was estimated by an apex locator and confirmation was done with an intraoral periapical radiograph (IOPA) (Fig4). Manual instrumentation in 11 was done with K-files(Mani, Japan) 80 no. along with passive irrigation of 5.25% sodium hypochlorite (NaOCl) (Septodont Healthcare India Pvt.Ltd., Mumbai). Irrigation was carried out with side-vented irrigation needles (keeping them 1 mm short of the radiographic apex). Furthermore, irrigants were activated with an Endoactivator(2-3 mm vertical pumping action) keeping the tip 2 mm short of apex without damaging the apical tissue. After a final rinse with 2% chlorhexidine, the canal was dried thoroughly with sterile absorbent paper points. The shaping and cleaning of 12 were completed with rotary NiTi files Hero Shaper up to size 30.04% and 17% EDTA(SybronEndo, CA, USA)was used as a lubricant. The intra-canal medicament of calcium hydroxide was placed for two weeks in 11 and 12. The access cavity was temporarily sealed with Cavit(3M, Espe, Saint Paul, MN, USA).
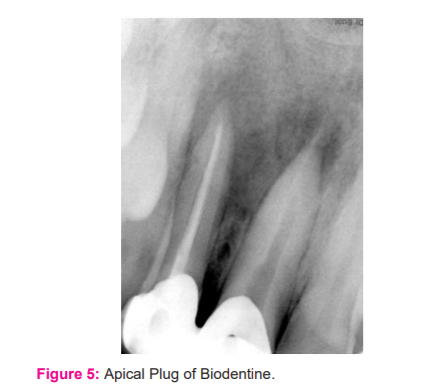
After a 2-week interval, placement of two dressings of Triple antibiotic paste (TAP) (ciprofloxacin 500mg, metronidazole 400mg and minocycline 100mg mixed with normal saline) were also done for 15 days respectively. On the next endodontic visit, the patient was asymptomatic. The removal of intracanal dressing done with copious irrigation of 5.25% hypochlorite followed by EDTA and dried with absorbent paper points. The formation of apical plugin 11Biodentine(Septodont, St. Maur.des.Fosses, France)was manipulated according to the manufacturer's recommendation and placed in the apical one-third of the root canal with the help of an amalgam carrier. It was condensed into the canal with a plugger to create an apical plug of 5 mm and was left undisturbed for the next 24-48 hour (Fig 5).
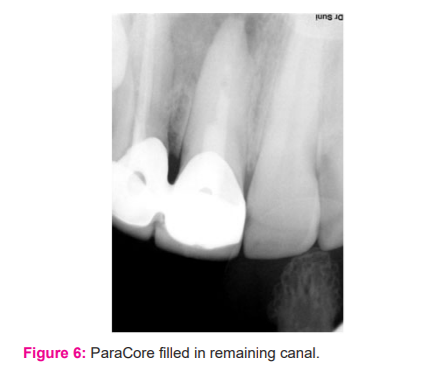
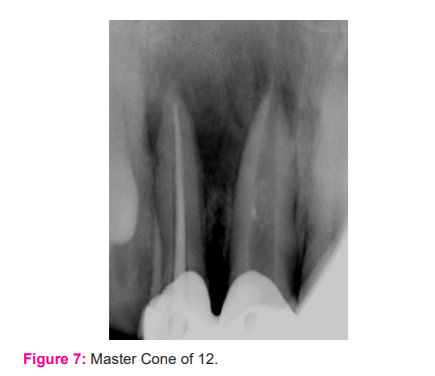
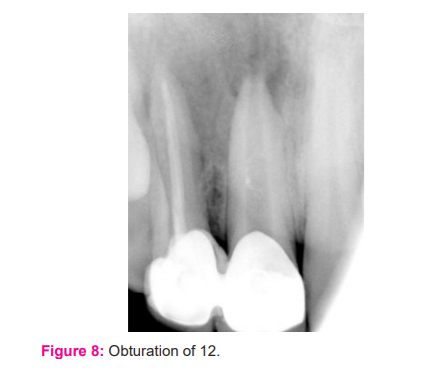
The correct position of the Biodentine mixture was controlled with a periapical radiograph and the access cavity was closed with a temporary filling material for the setting. The temporary filling was removed after two days and check the hardness of the apical plug with an endodontic plugger. The remaining portion of the root canal was filled with ParaCore (ColteneWhaledent) (Fig 6).12 was obturated using lateral condensation technique with zinc oxide eugenol based sealer and post-operative restoration done with composite (Fig 7-8).
Results
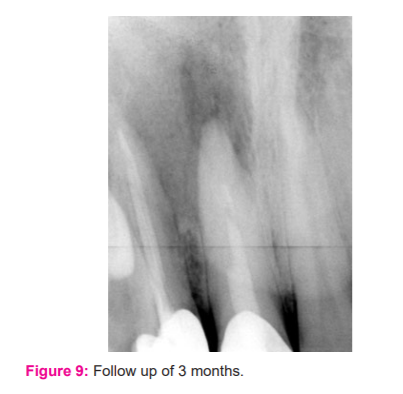
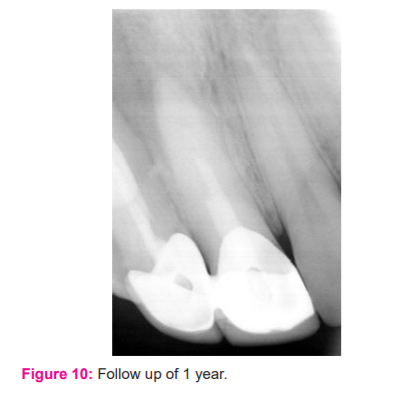
The clinical follow-up of 3 months and 1 year was taken, revealed no sinus formation and complete healing of periapical radiolucency (Fig 9-10). The formation of the apical third was seen on radiographic examination along with the formation of bone at the periapical region.
Discussion
Periapical pathology of pulpal origin develops in response to microbial irritants in the root canal system. Irreversible pulpitis and pulpal necrosis usually occur due to constant trauma and injury to the dental pulp.1 Complete eradication of the microbes from the root canal system is the biggest trouble while treating the tooth with non-vital pulp and open apex.9
Removal of necrotic pulp tissue remnants and microorganisms from the root canal system and canal disinfection is that the primary factor required for successful apexification. An antibacterial dressing is used to fortify the elimination of bacteria which are impenetrable to instrumentation and irrigation.10
Various studies had been reported that when a conservative approach is performed using endodontic therapy alone, the appropriate success rate was to be about 85% and 94.4% in partial or complete healing for the management of periapical lesions.11 The treatment process for non-vital teeth with open apex, it is proposed that the intracanal disinfection protocol has to be highly effective, which involve 5.0% NaOCl as irrigant and CH as an intracanal medicament to reduce the bacterial load, to neutralize acidic environment, activation of phosphate enzyme, for its hygroscopic properties, to repair the damage occur within the root canal and finally to arrest external inflammatory root resorption and promotion of hard tissue deposition; and subsequent placement of TAP dressings were done.12Several studies within the literature have confirmed the antimicrobial efficacy of TAP against endodontic pathogens, especially resistant organisms like Enterococcus faecalis and Candida and biofilms than calcium hydroxide, and also delivered effects within 14 days of duration.13
Biodentine is formulated on the theory of ‘‘active borosilicate technology’’.It is without any metallic impurities within the mixture accountable for lowering material strength.14Biodentinealso provide various advantages over MTA as expedite setting and ease in manipulation and working. The manufacturer advocates thorough and uniform speculation. The properties of dentine incorporate an initial set of 9 to 12 minutes, therefore further steps like complete root canal obturation, permanent restoration can be performed on the single visit of the apical plug formation. During the setting of the material, precipitation of hydroxyapatite crystallites occurs between the dentinal surface and interface and also provide micromechanical adhesion and adaptability with surrounding dentin. The higher calcium release from Biodentine and prominent uptake of calcium by adjacent root dentin enhances its bioactive effect and periapical healing compared with MTA.15
On clinical and radiographic evaluation, the treatment procedure which has been opted shows highly satisfactory results along with the complete resolution of all clinical signs and symptoms along with complete radiographic healing at 3 months and 1 year follow up.
Conclusion
A conservative approach for treating the periapical lesion and open apices in the non-vital permanent tooth was done by using Biodentine, the outcome of the report was astonishing without surgical intervention. It helps in the protection of anatomic structures and prosthesis against injury and also minimizes the risk and complications of surgery which seems to be beneficial for the patient as well.
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of Funding: nil
Conflict of Interest: nil

References:
-
Khan SZ, Karim S, Mirza S. Effect of photodynamic therapy on the morphological changes of periapical inflammation: An experimental study in rats. Photodiagnosis Photodyn Ther. 2020 Sep;31:101839.
-
Sharma S, Sharma V, Passi D, Srivastava D, Grover S, Dutta SR. Large Periapical or Cystic Lesions in Association with Roots Having Open Apices Managed Nonsurgically Using 1-step Apexification Based on Platelet-rich Fibrin Matrix and Biodentine Apical Barrier: A Case Series. J Endod. 2018 Jan;44(1):179-185.
-
Pace R, Giuliani V, Nieri M, Di Nasso L, Pagavino G. Mineral trioxide aggregate as an apical plugin teeth with necrotic pulp and immature apices: a 10-year case series. J Endod. 2014 Aug;40(8):1250-4.
-
KandemirDemirci G, Kaval ME, Güneri P, Çal??kan MK. Treatment of immature teeth with nonvital pulps in adults: a prospective comparative clinical study comparing MTA with Ca(OH)2. Int Endod J. 2020 Jan;53(1):5-18.
-
Rafter M. Apexification: a review. Dent Traumatol. 2005;21(1):1-8.
-
Sharma V, Sharma S, Dudeja P, Grover S. Endodontic management of nonvital permanent teeth having immature roots with one step apexification, using mineral trioxide aggregate apical plug and autogenous platelet-rich fibrin membrane as an internal matrix: Case series. Contemp Clin Dent 2016;7:67-70.
-
Pérard M, Le Clerc J, Watrin T, Meary F, Pérez F, Tricot-Doleux S, Pellen-Mussi P. Spheroid model study comparing the biocompatibility of Biodentine and MTA. J Mater Sci Mater Med. 2013 Jun;24(6):1527-34.
-
Villat C, Grosgogeat B, Seux D, Farge P. Conservative approach of the asymptomatic carious immature permanent tooth using a tricalcium silicate cement (Biodentine): a case report. Restore Dent Endod. 2013 Nov;38(4):258-62.
-
Yadav S, Nawal RR, Talwar S, Verma M. Low-level laser therapy for the management of large periapical lesions associated with open apex cases. Indian J Dent Res. 2020 Mar-Apr;31(2):334-336.
-
Cvek M. Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha. A retrospective clinical study. Endod Dent Traumatol. 1992 Apr;8(2):45-55.
-
Murphy WK, Kaugars GE, Collett WK, Dodds RN. Healing of periapical radiolucencies after nonsurgical endodontic therapy. Oral Surg Oral Med Oral Pathol. 1991 May;71(5):620-4.
-
Soares J, Santos S, Silveira F, Nunes E. Nonsurgical treatment of extensive cyst-like periapical lesion of endodontic origin. IntEndod J. 2006 Jul;39(7):566-75.
-
Abbaszadegan A, Dadolahi S, Gholami A, Moein MR, Hamedani S, Ghasemi Y, Abbott PV. Antimicrobial and Cytotoxic Activity of Cinnamomumzeylanicum, Calcium Hydroxide, and Triple Antibiotic Paste as Root Canal Dressing Materials. J Contemp Dent Pract. 2016 Feb 1;17(2):105-13.
-
Grech L, Mallia B, Camilleri J. Investigation of the physical properties of tricalcium silicate cement-based root-end filling materials. Dent Mater. 2013 Feb;29(2):e20-8.
-
Han L, Okiji T. Bioactivity evaluation of three calcium silicate-based endodontic materials. Int Endod J. 2013 Sep;46(9):808-14.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





