IJCRR - 13(12), June, 2021
Pages: 160-167
Date of Publication: 22-Jun-2021
Print Article
Download XML Download PDF
Comparing Short Term Effect of Aqua Stretch with Supervised Land-Based Stretching in Chronic Non-Specific Neck Pain Among Young Working Female Physiotherapists: A Randomized Clinical Trial
Author: Esha Pandya, Komal Makhecha, Anand Patel
Category: Healthcare
Abstract:Introduction: Although the natural history of neck pain appears to be favourable, rates of recurrence and chronicity are high.As physiotherapists daily deal with all work-related musculoskeletal problems and the job nature of physiotherapists including treating the patients, lifting the body part of the patients and awkward posture to treat the patients leads to neck pain. Aqua stretch is a new form of assisted stretching in the water. It is considered a breakthrough in pain management and preventive medicine. Aqua stretch exercising seems to quickly dissolve/release fascial adhesions by controlling stretch resistance. Aim: To comparing the short term effect of aqua stretch with supervised land-based stretching among young working female physiotherapists having chronic non-specific neck pain. Methodology: 60 female physiotherapists with chronic neck pain age between 22-30 years of age were randomly allocated into 2 groups (aqua stretch and land-based stretching). After signing the consent form, patients were taken for pre-intervention NDI (neck disability index) score, NPRS (numerical pain rating scale) & ROM (range of motion). Then instructions about aqua stretch were given. Treatment sessions will be 3 sessions per week and each session will be of 30 minutes up to 6 weeks. NDI questionnaire will be taken on the 1st meeting and again on weeks 4th and 6th. ROM will be measured weekly till 6 weeks, NPRS will be taken immediately after every session, twice a week, till 6 weeks. Result: Statistical significance (p< 0.05) was observed in the AquaStretch group for pain reduction (P= 0.006), ROM (P= 0.06), and NDI (P=0.0029). Conclusion: 6 weeks of Aquastretch can reduce pain, increase restricted ROM and also can improve quality of life in patients with chronic non-specific neck pain and also suggests that AquaStretch can improve pain tolerance in the cervical region.As a practical technique used to decrease pain and increase mobility AquaStretch could be a valuable addition to the current techniques available for chronic non-specific neck pain
Keywords: Key Words: Aquatic Therapy, AquaStretch, Non-specific neck pain, Chronic neck pain in physiotherapists, Musculoskeletal problems in female physiotherapists, Stretching exercise in chronic pain
Full Text:
INTRODUCTION
The International Association for the Study of Pain-IASP-defines cervical spinal pain as "pain perceived anywhere in the posterior region of the cervical spine, from the superior nuchal line to the first thoracic spinous process"1 Pain is classified as chronic when it has a duration of 12 weeks or more. Chronic neck pain often presents hyperalgesia on palpation and in both passive and active movements in the neck and shoulder area. 1
Although the natural history of neck pain appears to be favourable, rates of recurrence and chronicity are high. 30% of patients with neck pain will develop chronic symptoms. With neck pain longer than 6 months in duration affecting 14% of all individuals who experience an episode of neck pain. 37% of individuals who experience neck pain will report persistent problems for at least 12 months. 5% of the adult population with neck pain will be disabled by the pain, representing a serious health concern. 2
Occupational health hazards are very common. As physiotherapists daily deal with all work-related musculoskeletal problems and the job nature of physiotherapists including treating the patients, lifting the body part of the patients and awkward posture to treat the patients leads to neck pain. The prevalence of neck pain in physiotherapists is 41% according to one study. One more study shows that the prevalence of neck pain among physiotherapists is 51.7%. Working in OPD & poor posture are major factors that contributed to neck pain. 3,4
Neck pain is the second most common work-related musculoskeletal disorder. And if we compare the prevalence of male and female physiotherapist having neck pain, female physiotherapists of relatively younger age are at higher cumulative risk of neck pain.5
According to one study, commonly affected muscles are upper trapezius with the prevalence of 93.75%, levator scapulae with the prevalence of 82.14%, multifidi with the prevalence of 77.68% and splenius cervicis with the prevalence of 62.5%. Till now so many different techniques are developed which are used to treat chronic neck pain, but the effectiveness of assisted stretching in water is unknown.3
Aqua stretch is a new form of assisted stretching in the water. It is considered a breakthrough in pain management and preventive medicine. Aqua stretch exercising seems to quickly dissolve/release fascial adhesions by controlling stretch resistance, by changing buoyancy, and by accepting the body’s intuitive movements that occur when joints are subjected to stretch pressure. In the low environment of water, the body may stretch in positions it cannot while under the influence of normal gravity on land and for much longer periods. Aqua stretch is a myofascial release technique performed in shallow water. Aqua stretch breaks down fascial adhesions using a combination of the facilitator/therapist's manual pressure and the client/patient's active movement, quickly restoring flexibility and reducing pain. Aqua stretch promotes relaxation, which helps to improve function, quality of life, sleep, and the overall ability to heal. Upon immersion, physical stress and load on the body, or the weight-bearing on the joints, is going to be extremely reduced. It is a zero-gravity event that the client experiences. The buoyancy, increase in blood flow, increase in flexibility, and reduction in joint compression will allow the participant to have increased movement with reduced restriction. They will be able to get into positions that they would not necessarily be able to get into when on land. That is exciting and a key factor in the effectiveness of this particular modality. 7
A previous study was done on comparison of the effect of aqua stretch and land-based stretching in patients with chronic low back pain. Statistical significance (p < 0.05) was observed in the aqua stretch group for reduction in pain with P = 0.006, in kinesiophobia with P = 0.029, and in perceived disability with P = 0.001. Both techniques are suggested to be beneficial for chronic low back pain patients however aqua stretch has key additional benefits including time efficiency and cost effectiveness.8Another study was done comparing the effect of hydrotherapy and land-based exercises in the management of chronic low back pain and they found that the two exercise media were relevant in the management of chronic low back pain, though hydrotherapy seems to be better for spinal flexibility, thus serving as a better alternative in clinical practice.9
Till now no studies could be retrieved examining the effect of aqua stretch in patients with chronic neck pain. Moreover, according to the literature, it is concluded that the effect of aqua stretch is immediate and also it persist 3 to 4 times longer than the normal land-based stretches which are used by the therapist in clinical practice.7
So, the need of this study was to find out better management for chronic neck pain which will be more effective and could be a better alternative for the management of chronic neck pain in clinical practice.
AIM OF THE STUDY
The study aimed to compare the short term effect of aqua stretch with supervised land-based stretching among young working female physiotherapists having chronic non-specific neck pain.
OBJECTIVES OF THE STUDY
-
To measure ROM (Range of Motion) Of cervical spine with a Mobile inclinometer,
-
To evaluate the pain and functional disability level with NDI (Neck Disability Index)
-
To evaluate pain perception with, NPRS (Numerical Pain Rating Scale).
MATERIALS AND METHOD:
Study design Randomised clinical trial Study population young working female physiotherapists with chronic non-specific neck pain
Study sample (TYPE OF SAMPLING)Purposive sampling
Study sampling size 60 subjects with chronic non-specific neck pain
Study setting Govt. and private clinics of Mangalore, Karnataka and ASIAN physiotherapy and research centre, Surat, Gujarat.
Inclusion criteria: 3,5,10
-
Female physiotherapists having neck pain for more than 3 months,
-
Age: 22-30 years,
-
Working in clinical field at least for 4-5 hours per day
Exclusion criteria: 3,13
-
Having neck pain before starting work as a physiotherapist,
-
Recent injuries around shoulder and neck region(less than 6 months),
-
Hydrophobia,
-
Any deformities (torticollis),
-
Any skin infections (tinea pedis, ring warms),
-
Open wound,
-
Pathological neck pain,
-
Working in academic field,
-
History of uncontrolled seizures during the last year,
Outcome measures
Method of collection of data
Subjects were screened and were selected according to the inclusion criteria. All subjects were asked to sign the written consent form stating the voluntary acceptance to participate in the study.
Then the demographic information (i.e. age, gender, height, weight, and other details) was collected from all selected subjects. Then a screening questionnaire was given to the patient to confirm the neck pain and the pain is because of their work. After that subjects were selected according to the inclusion.
Subjects were asked not to participate in any form of additional therapy for the duration of the study. They were asked to refrain from taking any pain-relief or anti-inflammatory medication on the data collection and intervention days. The subjects were instructed to continue their normal levels of physical activity throughout the study period without changes. They were specifically instructed to avoid any new form of treatment for chronic neck pain.
Then the first set of NDI (Neck disability index) questionnaire, NPRS (Numericalpain rating scale) and ROM (Range of motion) of the cervical spine was completed by the subjects.
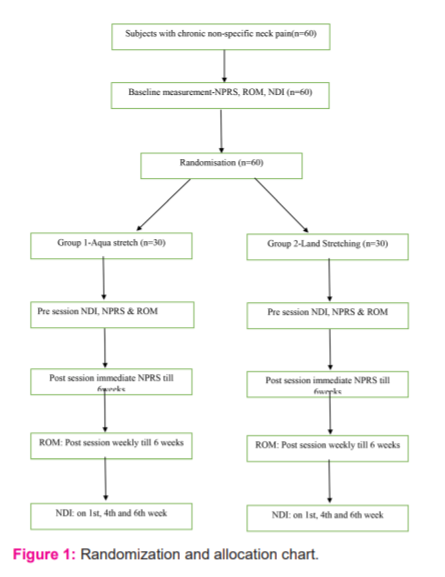
Randomization and allocation:
Subjects were randomly assigned into two groups (aqua stretch and land-based stretching) using a blind chit method to assign participants to each of the two groups, aqua stretch and land stretching (Figure 1).
Intervention
1) Land stretching group: For all stretches, position of the subjects was supine.Therapist was at the head of the treatment table. Hand placements was according tocomfort and size of the subject’s head. All stretches will be repeated 3 times with 30 seconds of hold. 13
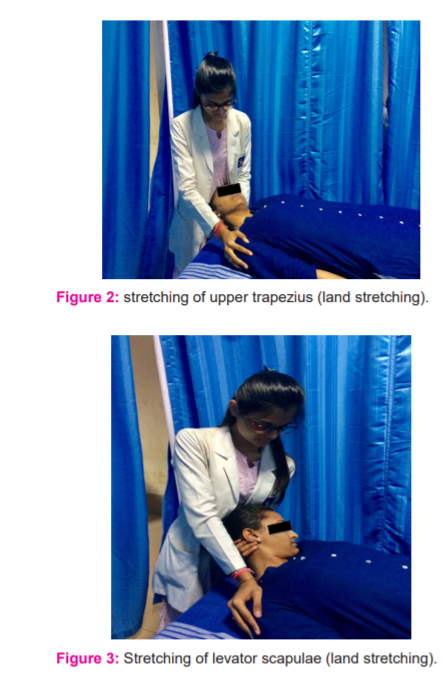
• Stretching of upper trapezius: Position of subject and therapist was as describedabove. For stretching of upper trapezius, therapist stabilized the subject’s shoulder of one side (more affected side will be stretched first) with one hand and then took subject’s head in lateral flexion to the opposite side. This was be repeated on other side too.13
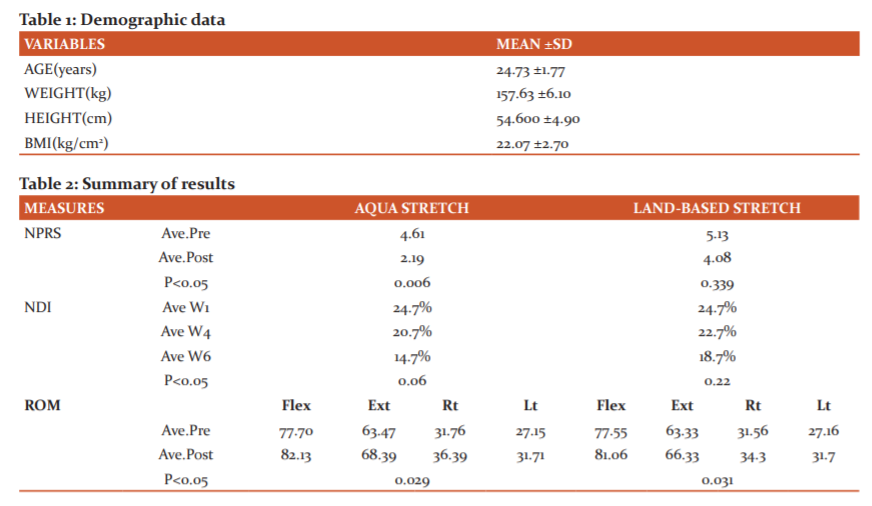
• Stretching of levator scapulae: Position of subject and the therapist was as described above. For stretching of levator scapulae, the therapist stabilized the subject’s shoulder on the side to be stretched and with the other hand, held the subject’s head from occiput. Then therapist took the subject’s head in flexion, opposite side lateral flexion and opposite side rotation. This was repeated on another side too (Figure 2).13
• Stretching of splenius cervicis: The position of therapist and subject was as described above. For stretching of splenius cervicis, the therapist stabilized the subject’s shoulder on the side to be stretched and with the other hand, held the subject’s head from occiput. Then therapist took the subject’s head on opposite side flexion and rotation (Figure 3).13
2) Aqua stretch group: For an aqua stretch, muscles to be stretched were the same as land stretching. The position of the subject was supine (buoyancy supported) with ankle and wrist floaters. The position of the therapist was the same as land stretching. All stretches were also the same as land stretching following the four-step procedure of aqua stretch. Just the treatment media was changed to water. The temperature of the pool water was maintained at around 28 degrees.7,13
The four strep procedure of aqua stretch is as below:
1. Play: Patient is asked to move (play) with their body’s movement until they experience pain or restriction.
2. Freeze: Patient freezes in the exact position they feel pain or tension
3. Pressure: The therapist applies pressure to the area of pain or restriction, while the client maintains
a frozen position (Figure 4, 5).
4. Move: Patient is asked to move if they feel the need to move


EXERCISE DOSAGE: Both the interventions were given 3 sessions per week till 6 weeks.
RESULTS
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS
v21.0.0). Results were considered statistically significant at a 95% confidence level (p<0.05).
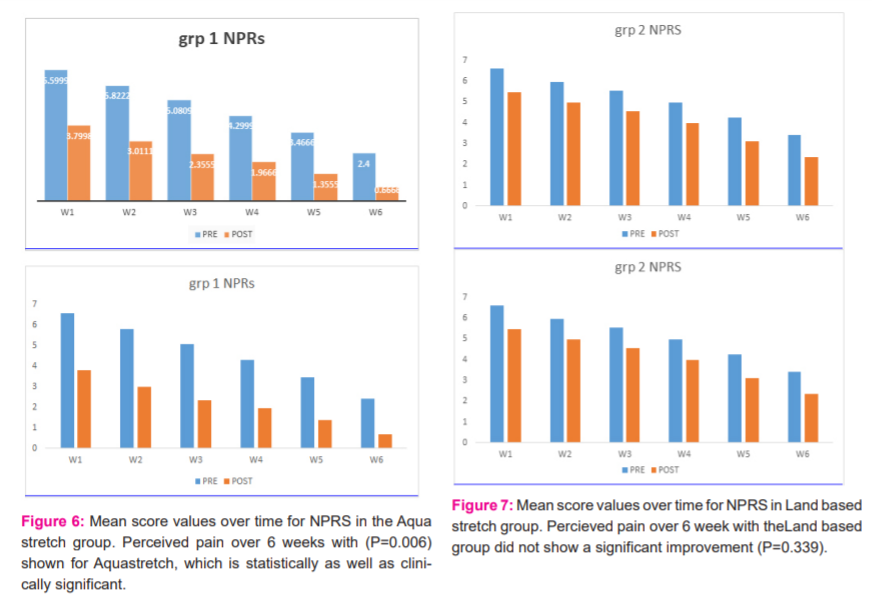
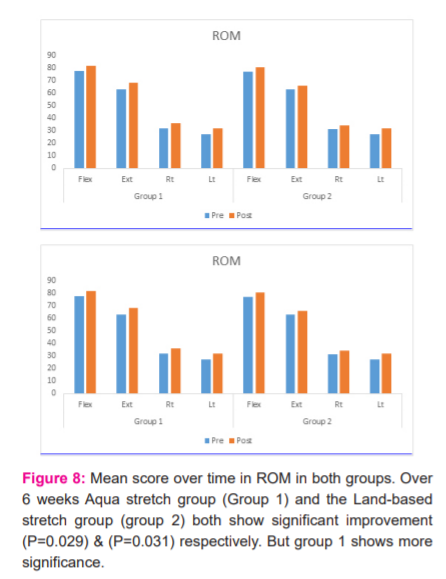
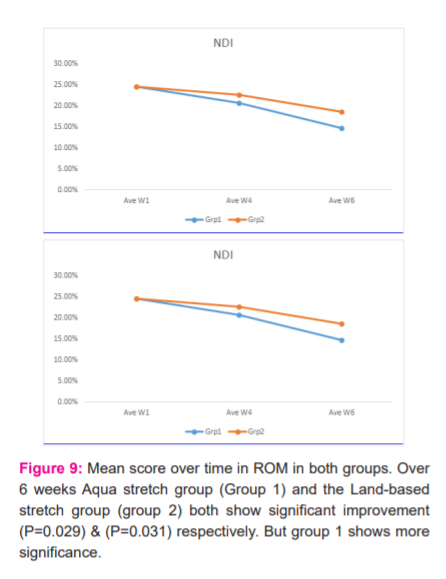
A factorial ANOVA was used to find the mean within each group. The demographic data are described in table 1 and 2. The intensity of pain on NPRS (numerical pain rating scale) was significantly reduced immediately after the treatment sessions in an aqua stretch group compared with land-based stretching. The Neck Disability Indexed showed a more significant reduction in the percentage of disability in the aquastretch group than a land-based stretch at the end of 6 weeks. Lso the range of motion of the neck was more significantly improved with aqua stretch shown in Figure 6, 7, 8, and 9.
DISCUSSION
This is the first study to the best of our knowledge which aimed to find the effectiveness of Aquastretch in patients with chronic non-specific neck pain. Studies have been done on the effect of AquaStretch in the management of CLBP 8,9, however, no study has yet been conducted on chronic non-specific neck pain.
In this study, we included 60 young working female physiotherapists (30-30 in each group) with age group 22-30 years. The age criteria and the female gender were chosen as there is a high prevalence of developing work-related neck pain among female physiotherapists according to previous studies.3,4,5
The results of our study showed significant improvement in the self-reported level of pain (intensity-NPRS) scores in the Aqua Stretch group (p<0.05) immediate as well as after 6 weeks. This concurs with the other studies (done in CLBP) of short duration that land exercise and water exercise are comparable for relieving pain in chronic non-specific neck pain also.9
The reason behind the greater improvement in pain with AquaStretch was that in the low (hypobaric) environment of water, the body may stretch in positions it cannot while under the influence of normal gravity on land and for much longer periods. Moreover, AquaStretch exercising seems to quickly dissolve/release fascial adhesions by controlling stretch resistance, accomplished by wearing weights (5 to 15 lbs.), by changing buoyancy, and by accepting the body’s intuitive movements that occur when joints are subjected to stretch pressure.7
It is important to restore normal muscle length, increase muscle performance and flexibility.19,20 Neck pain with limitation of mobility occurs mostly due to constant faulty posture or, frequently, neck movements result in decreased range of motions (ROM). A common cause of neck pain is muscle strain or tension.15,16,17 As AquaStretch is proved to quickly dissolve/release fascial adhesions7 and where on the other hand, the land-based sustained stretch also helps in elongation of pathologically shorten soft tissue structures. There was a significant improvement in cervical spine ROM after 6 weeks in both the groups, with (p=0.029) & (p=0.031) respectively for group 1 & group 2. But the AquaStretch group improved with more significance.
One well-known disablement model, proposed by Ngai, suggests that pathology produces pain and impairments, which then lead to functional limitations and disability.18 The current study showed that there is more reduction in NDI score in Aquastretch group after 6 weeks with (p=0.06), which when compared to land-based stretch, shows no significant reduction in the score (p=0.22). The reason behind this was greater improvement in pain tolerance after 6 weeks of AquaStretch exercise. According to previous literature, the benefits of AquaStretch are relief of pain and muscle soreness and restore muscle flexibility. Patients who have pain or muscle soreness in rehabilitation, wellness, or fitness environments could benefit from AquaStretch.7
A significant number of people with neck pain do not experience a complete resolution of symptoms with 50–85% reporting recurrence 1 to 5 years later. Consequently, neck pain results in enormous health costs in terms of treatment lost wages and work absenteeism.20 The results of this study showed improvement in quality of life with AquaStretch showing that it has additional key benefits including time efficiency and cost-effectiveness
This study was done only on young female physiotherapists. Also, only short-term effects were measured. The long-term effect of this technique remains unchecked.
The study can be done with other population with chronic non-specific neck pain, rather than only female physiotherapists. Also, long term follow-up has to be taken to check the long-term effects of the treatment.
LIMITATIONS OF THE STUDY
This study was done only on young female physiotherapists. Also, only short-term effects were measured. The long-term effect of this technique remains unchecked.
RECOMMENDATION FOR FUTURE RESEARCH
The study can be done with other population with chronic non-specific neck pain, rather than only female physiotherapists. Also, long term follow-up has to be taken to check the long-term effects of the treatment.
CONCLUSION
Our study found that Aquastretch can reduce pain, increase restricted ROM (Range of motion) and also can improve quality of life in patients with chronic non-specific neck pain and also suggests that AquaStretch can improve pain tolerance in the cervical region.
As a practical technique used to decrease pain and increase mobility Aqua Stretch could be a valuable addition to the current techniques available for chronic non-specific neck pain.
There was nil funding used during the study.
ACKNOWLEDGEMENT: I would like to thank my colleagues and Dr. Sagar Naik (owner of aqutherapy set up) who helped me to complete my study.
Source of funding: Nil
Conflict of Interest: Nil
References:
-
Misailidou V, Malliou P, Beneka A, Karagiannidis A, Godolias G. Assessment of patients with neck pain: a review of definitions, selection criteria, and measurement tools. J Chiropr Med. 2010 Jun 1;9(2):49–59.
-
Blanpied PR, Gross AR, Elliott JM, Devaney LL, Clewley D, Walton DM, et al. Neck Pain: Revision 2017. J Orthop Sports Phys Ther. 2017;47(7): A1–83.
-
Shah. S, Kachhadiya A., Kachhadia A, Savani P, Shukla V, Patel A, Parmar E, et al. Prevalence of back and neck pain among physiotherapists. Ind J Physiother Occup Ther Int J. 2012;6(4):1-3
-
Shah I, Gangwal A, Bedekar N, Shyam A, Sancheti P.Work related musculoskeletal disorders among Indian physiotherapists. Ind J Physic Ther.2016 Jul 3;4(1):20-4.
-
Khan U, Fasih M.Prevalence of work related neck pain among physiotherapists and its association with age and gender. Pak J Physiol.2017;13(3):39-42.
-
Cerezo Téllez E, Torres Lacomba M, Mayoral Del Moral O, Sánchez Sánchez B, Dommerholt J, Gutiérrez-Ortega C. Prevalence of Myofascial Pain Syndrome in Chronic Non-Specific Neck Pain: A Population-Based Cross-Sectional Descriptive Study. Pain Med. 2016;17(12):2369–77.
-
Sova, R. (2012). Introduction of Aquatic Therapy and Rehab. (Third Edition). Port Washington, WI: DSL, Ltd
-
Keane LG. Comparing AquaStretch with supervised land-based stretching for Chronic Lower Back Pain. J Bodyw Mov Ther. 2017 Apr 1;21(2):297-305.
-
Bello AI, Kalu NH, Adegoke BOA, Agyepong-Badu S. Hydrotherapy Versus Land-Based Exercises in the Management of Chronic Low Back Pain: a Comparative Study. J Musculoskelet Res. 2010;13(4):159–65.
-
Glover W. Work-related Strain Injuries in Physiotherapists: Prevalence and prevention of musculoskeletal disorders. Physiother. 2002 Jun 1;88(6):364-72.
-
Y., Tousignant-Laflamme, N. Boutin, A.M. Dion C., A. Vallee C.A., Vallee. Reliability and criterion validity of two applications of the iPhone to measure the cervical range of motion in healthy participants. J Neuroeng Rehabil. 2013;10(1):69.
-
Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther. 1991 Sep;14(7):409-15.
-
Kisner C, Colby LA, Borstad J. Therapeutic exercise: foundations and techniques. Fa Davis; 2017 Oct 18.
-
Häkkinen A, Salo P, Tarvainen U, Wiren K, Ylinen J. Effect of manual therapy and stretching on neck muscle strength and mobility in chronic neck pain. J Rehab Med. 2007 Sep 5;39(7):575-9.
-
Cassidy JD, Lopes AA, Yong-Hing K. The immediate effect of manipulation vs. Mobilization on pain and range of motion in the cervical spine: A randomized controlled trial. J Manipulative Physiol Ther. 1993;16:279-80.
-
Hoving JL, Koes BW, de Vet HC, van der Windt DA, Assendelft WJ, van Mameren H, et al. Manual therapy, physical therapy, or continued care by a general practitioner for patients with neck pain: a randomized, controlled trial. Ann Internal Med. 2002;136:713-22.
-
Holm LW, Carroll LJ, Cassidy JD, Hogg-Johnson S, Côté P, Guzman J, et al. The burden and determinants of neck pain in whiplash-associated disorders after traffic collisions: Results of the bone and joint decade 2000-2010 task force on neck pain and its associated disorders. J Manipulative Physiol Ther. 2009;32:S61-9.
-
Ngai SZ. Some conceptual issues in disability and rehabilitation. In: Sussman MB, editor. Sociology and rehabilitation.Washington (DC): Amer Soci Assoc. 1965. P100-13.
-
Riaz F, Haider R, Qamar MM, Basharat A, Manzoor A, Rasul A, Ayyoub A, Ahmad W. Effects of static stretching in comparison with Kaltenborn mobilization technique in nonspecific neck pain. J Health Sci. 2018 Jul 1;3(2):85.
-
Hidalgo B, Hall T, Bossert J, Dugeny A, Cagnie B, Pitance L. The efficacy of manual therapy and exercise for treating non-specific neck pain: A systematic review. J Health Sci. 2017 Jan 1;30(6):1149-69.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





