IJCRR - 2nd Wave of COVID-19: Role of Social Awareness, Health and Technology Sector, June, 2021
Pages: 159-165
Date of Publication: 11-Jun-2021
Print Article
Download XML Download PDF
Anxiety, Depression, Stress and Post-Traumatic Stress Disorder Among the General Population in Assam During the Early Phase of the COVID 19 Pandemic
Author: Dhrubajyoti Bhuyan, Seujee Goswami, Mustakim Ahmed, Hiranya Saikia
Category: Healthcare
Abstract:Introduction: Recent research has revealed the increased occurrence of anxiety, depression, PTSD and higher stress levels during the ongoing novel coronavirus 2019 (COVID-19) pandemic, similar to those of past epidemics like SARS (Severe Acute Respiratory Syndrome) and Ebola. Objective: This study aimed at assessing the occurrence of anxiety, depression and post-traumatic stress disorder (PTSD) among the general public of Assam during the early phase of the COVID 19 pandemic. Methods: Using quota sampling, data were obtained by emailing questionnaires to the participants. The symptoms of anxiety, depression and stress were assessed by the 21 item version of Depression Anxiety Stress Scales (DASS-21). The symptoms of PTSD were evaluated by using the revised version of the Impact of Events scale (IES R). Results: On analysis by SPSS version 24, among 247 final respondents, using DASS-21, symptoms of anxiety, depression and stress were noted in 29.5 per cent, 29.7percent and 19.7 per cent respondents. The Impact of Events Scale-Revised revealed a clinical concern for PTSD in 43 per cent, a probable diagnosis of PTSD in 26.6 per cent and a high risk of PTSD in 20.1 per cent of the respondents. Students and non-medical professionals were found to be affected to a greater degree, while healthcare professionals showed more severe symptoms of anxiety. Conclusion: Symptoms of anxiety, depression, increased stress and PTSD were noted in the population of Assam during the early phase of the COVID 19 pandemic. Further research in this field with larger sample sizes could aid in planning the neces�sary psychiatric interventions and prepare for future pandemics.
Keywords: COVID 19, Anxiety, depression, Stress, Post-traumatic stress disorder
Full Text:
INTRODUCTION
The 2019–20 coronavirus pandemic caused by the novel coronavirus (COVID-19) has led to extensive suffering and death all over the world.1 As of April 2020, more than 896 000 cases of COVID-19 have been reported with over 45525 deaths in at least 170 countries and territories, with major outbreaks in China, Iran and the European Union.2 Its management consists of providing symptom relief and supportive therapy to the patient. To date, no vaccine or specific antiviral medication against this illness is available to mankind. An outbreak of such magnitude and severity can naturally be expected to have a deep and widespread impact on the mental well-being of people as well as instil terror into the hearts of millions globally. The measures implemented to stop the further transmission of this virus comprise limitations on travel, quarantines, lockdowns of wide areas, closure of offices, business establishments and educational institutions that have greatly affected the day to day life of populations all over the world.3
Similar epidemics in the past such as the Severe Acute Respiratory Syndrome (SARS) outbreak of 2003 and the Ebola virus disease outbreak of 2009 have shown a higher incidence of several psychiatric manifestations including those of post-traumatic stress disorder (PTSD), depression, stress, insomnia, grief and emotional exhaustion among the affected populations.4-9 In the light of this grave pandemic, initial studies have revealed symptoms of anxiety depression increased stress levels PTSD and insomnia among the general public as well as the health care workers in the affected nations.10-14
Thus, more studies focusing on the psychological consequences of the COVID 19 pandemic as well as planning interventions for their alleviation appear to be the need of the hour. Since very few such studies are currently available from the northeastern states of India, we conducted a study to evaluate the psychological consequences of the ongoing COVID 19 pandemic on health care professionals as well as the general public of Assam by assessing the occurrence of anxiety, depression and post-traumatic stress disorder among them. As only a few cases of COVID 19 had been detected in the study population till the phase of our data collection, the information thus obtained could be of great relevance in the preparedness phase of any future outbreak of this nature.12,13
MATERIALS AND METHODS
After obtaining due permission from the Institutional Ethics Committee via letter no. AMC/EC/1064 dated 06/04/2020, the sample for the study was drawn from the health care workers as well as the general public of Assam by quota sampling. Persons of 18 years and above with a valid email address were identified and subdivided into five groups based on feasibility. The first of these groups consisted of health care professionals including doctors and paramedical workers. The second, third and fourth groups included faculty of higher educational institutions, sales and marketing professionals and employees of the judicial system respectively. The fifth group of students of various fields of study was incorporated, as was a sixth group consisting of business persons and other persons working in commercial enterprises. From each of these six groups, 50 subjects were emailed the questionnaires. The questionnaires included an initial section for obtaining informed consent from the subjects which was necessary for the data collection in the subsequent sections via the various tools.
The tools used for the study included the 21 item version of the self-reporting Depression Anxiety Stress Scales (DASS 21) developed by Lovibond et al. which was used for evaluating the symptoms of depression, anxiety and stress.15 Moreover, the revised version of the Impact of Events Scale, developed by Weiss and Marmar in 1997 for measuring the subjective distress due to traumatic events was used to assess the risk for Post Traumatic Stress Disorder(PTSD) in the subjects.16 The obtained data were kept strictly confidential. Statistical analysis of the data was carried out via the SPSS version 24, and the calculated results were presented in terms of frequencies, percentages and mean ? standard deviation. The statistical significance was tested using the chi-square test or Fisher's exact test, and a p-value of less than 0.05 was considered statistically significant.
RESULTS
A total of 300 subjects were identified and emailed the study questionnaires, and 249 responses were obtained. Two responses with incomplete data were discovered that were rejected by the researchers. Thus, data from 247subjects were available for the final statistical analysis. It was observed that the mean age of the respondents was 35.59 ± 9.42 years, and 97.7 per cent of the respondents consisted of young adults and middle-aged persons between 20 and 49 years of age. Females constituted 43.7 per cent and males made up 56.3 per cent of the respondents. 61.9 per cent of the respondents were married and a majority of them were found to hail from nuclear families (57.1 per cent). For the sake of feasibility, the data from three groups of faculty of higher educational institutions, sales and marketing professionals and employees of the judicial system were analysed together as a single group of non-medical professionals. 23.1 percentages of the responses were from the group of health care professionals, while the groups of non-medical professionals, students and the others made up 51.0, 8.9 and 17 per cent of the responses respectively. The responses from the medical students were shifted to the group of health care professionals for the final analysis.
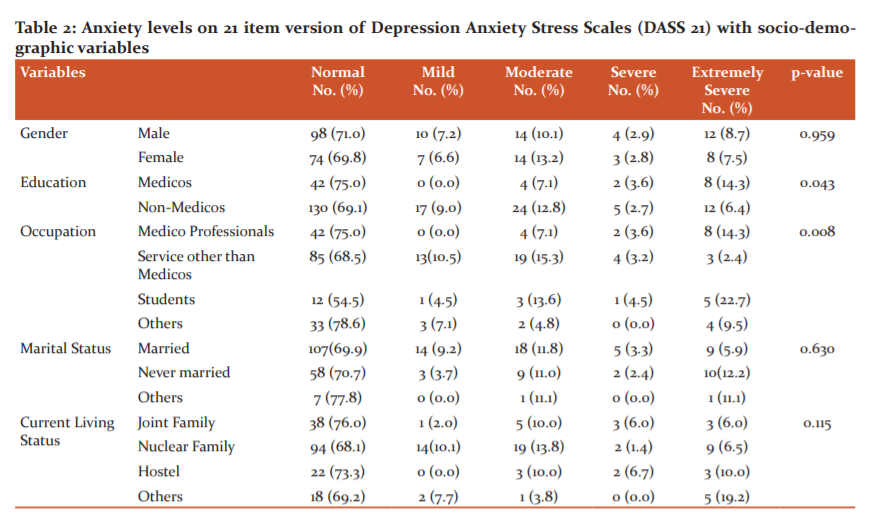
Tables 1-3 show the results of evaluation with the DASS 21. Here, mild depressive features were revealed in 18.9 percent respondents, while severe depression was noted in 10.6 percent of the respondents. A significantly higher rate of these symptoms was seen in the group of students (p value = 0.002).18.5 percent of the respondents were found to have features of mild to moderate anxiety, whereas 11.2 percent reported symptoms of severe anxiety. The overall anxiety levels were significantly higher in the group of non-medical professionals (p=0.043). However, the occurrence of severe anxiety (3.6%) and extremely severe anxiety (14.3%) were observed more frequently in the group of health care professionals as compared to the non-medical professionals. Also, a mild to moderate increase in stress levels was seen in 11.1 per cent of respondents with 8.6 per cent of them being found to be severely stressed as a consequence of the ongoing pandemic. Interestingly, a significantly greater level of stress was noted in the group of students (p=0.001) and the unmarried individuals (p=0.001) among all the groups under study.
Table 4 shows the results on assessment with the revised version of the Impact Of Events Scale Here, 43% of the respondents had a score ≥24, indicating clinical concern for Post Traumatic Stress Disorder (PTSD). These scores were found to be significantly greater in the group of students (p=0.006). On the other hand, 26.6% of the respondents had a score ≥33, which showed a probable diagnosis of PTSD, with significantly higher scores being observed in the group of students under study (p=0.02). 20.1% of the respondents showed a score of 37 or more, indicating a high risk of developing PTSD.
DISCUSSION
During the ongoing coronavirus pandemic, the various global health organisations including the World Health Organisation and the CDC are increasingly laying stress on measures for the prevention and treatment of the infection. These include early detection and segregation of affected individuals, identification of contacts, establishing reliable diagnostic criteria as well as effective interventional strategies for combating this serious illness. The grave impact of the pandemic as well as the ensuing quarantine on the mental health of millions across the globe stands sadly neglected.17,18
On evaluation with the DASS 21, features of depression, anxiety and increased stress levels ranging from mild to severe were noted in a significant fraction of the respondents. Similar findings have been reported in several other studies carried out during this ongoing COVID 19 pandemic. Such a study by Wang et al on the general public in 194 cities of China has revealed a moderate to severe psychological impact of the COVID 19 pandemic in 53.8% of respondents; while moderate to severe levels of depression, anxiety and stress were observed in 16.5%, 28.8% and 8.1% respondents respectively.10
The evaluation with the revised version of the Impact of Events Scale helped to measure the impact of the pandemic on the minds of the subjects, focusing on the presence of symptoms of post-traumatic stress in them. Our study detected the presence of certain symptoms of post-traumatic stress in 43% of the respondents indicating clinical concern for PTSD in them. Meanwhile, 26.6% of the respondents were detected with a probable diagnosis of PTSD, with a need for adequate monitoring and follow up to rule out PTSD. Furthermore, 20.1% of respondents were found with a high risk of having PTSD as an aftermath of the COVID 19 pandemic and required prompt and detailed evaluation and treatment for their condition. In another similar longitudinal study by Wang et al. including the general public from 190 cities of China, the initial mean scores on IES-R revealed PTSD symptoms that persisted in the second survey done four weeks later. Using the DASS, moderate and severe levels of stress, anxiety and depression were observed in 8.1%, 28.8% and 16.5%, of the respondents respectively without any significant changes in their levels longitudinally. (p>0.05).11
Furthermore, a study on 470 healthcare workers in Singapore by Tan et al. has revealed anxiety, depression, stress and clinical concern of PTSD in 14.5 %, 8.9%, 6.6% and 7.7% respondents respectively.13 A multinational, multicentre study by Chew et al. on healthcare workers during the COVID 19 pandemic included 906 respondents.12 Among them, 5.3%, 8.7% and 2.2% reported varying levels of depression, anxiety and stress respectively. Also, 7.4% of respondents had shown a clinical concern of PTSD, among who 34 exhibited moderate to severe levels of psychological distress. In another similar study by Tan et al on 673 working people in China, 10.8% were diagnosed with PTSD following their rejoining the workforce during the COVID 19 pandemic.14 This is consistent with the finding of a study at the time of the Ebola outbreak in Nigeria in 2014 that showed a high level of psychological distress in survivors as well as the persons closely in contact with them. The participants reported various symptoms including difficulties in concentration, insomnia, feeling of unhappiness, feeling constantly under strain as well as the inability to enjoy the activities of their daily life.19 Moreover, several other studies during epidemics like SARS in 2003 and Ebola viral disease in 2014 have revealed greater levels of emotional stress among health care professionals battling these epidemics.20-22 Symptoms of anxiety, depression and stress are persistent in them long after the resolution of the epidemic.22 The occurrence of depression and post-traumatic stress disorder (PTSD) has also been found to be increased among the persons who recovered from SARS.23-25 A similar study on patients under quarantine and undergoing haemodialysis as well as the medical professionals treating the people infected with Middle East Respiratory Syndrome (MERS) detected higher levels of psychological distress and PTSD in the early stage of the epidemic.26 Persons who had been hospitalised with the MERS have also been shown to have a low quality of life after one year of recovery.27
It is pertinent to mention here that in our study, the symptoms of depression and PTSD were found to be significantly greater in the group of students .This is similar to the study by Wang et al, that showed a higher level of anxiety, PTSD, depression and stress levels in the student group during the COVID 19 pandemic.10 This is similar to the study by Wang et al during the COVID 19 pandemic, wherein a higher occurrence of PTSD was noted in the age group with a majority of students.11 This finding could be explained by their isolation from peers and friends ,their academic and career related concerns coupled with the uncertainty caused by the postponement of their classes and exams as an aftermath of the pandemic .
In our study, the non-medical professionals were found to have a significantly higher overall anxiety level. This could stem from the relative lack of adequate knowledge regarding the pandemic and measures to contain it compounded by the major uncertainty and sudden upheaval brought into their lives by this devastating pandemic. The medical professionals were seen to have a higher frequency of experiencing severe and extremely severe levels of anxiety. Interestingly, in a recent study by Tan et al during the COVID 19 pandemic, the scores for anxiety, stress and PTSD were greater in health care workers excluding the physicians and nurses, after adjusting for the various confounders.13 This could be a consequence of being exposed to greater workloads and burnout, increased exposure to suffering and death as well as concerns related to their health and wellbeing while battling this terrible pandemic. It is interesting to note here that the stress levels were found to be significantly greater in the group of students and the unmarried individuals among all the groups under study.
Therefore, the designing of further studies on the psychological effects of this pandemic on these aforementioned high-risk groups and planning strategies targeted at their alleviation appears to be the need of the day. The limitations of our study include a relatively small sample size covering the population of a single state, Assam in India, due to which, the generalizability of the findings might not be as desired. Moreover, the findings of the study are limited to the early phase of the outbreak in the covered geographical area, as only a few cases had been diagnosed in the population here till the phase of data collection. Follow-up studies in this direction are being planned by the researchers for information on the later phases of the pandemic.
Conclusion
Thus we found that the on-going 2019 novel coronavirus pandemic is leaving a deep psychological impact on the health care professionals as well as the general public. These include features of anxiety, depression and post-traumatic stress disorder. Students, as well as non-medical professionals, was found to be affected to a greater degree by the pandemic, while health care professionals were found to be exhibiting more severe levels of anxiety.
Future studies designed in this area of research with a larger sample size and focused on the high-risk groups could be beneficial in planning interventions to mitigate the psychological impact of the COVID19 pandemic.
Acknowledgements: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Financial support: There are no funding sources or source of financial support to be declared by any of the authors.
Conflict of interest disclosures: There is no conflict of interest to be declared by any of the authors.
Author contribution: Concept and design: Bhuyan, Goswami and Saikia
Acquisition, analysis, interpretation of data: All authors
Drafting of the manuscript: Bhuyan, Goswami, Ahmed
Critical revision of the manuscript for important intellectual content: All authors
Statistical analysis: Saikia
Supervision: Bhuyan, Goswami and Saikia



References:
1. Coronavirus disease 2019. [Cited 2020 May 26]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
2. Coronavirus disease 2019 (COVID-19) Situation Report –73. [Cited 2020 May 26]. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200402-sitrep-73-covid-19.pdf
3. Q&A on coronaviruses (COVID-19)[Internet]. [cited 2020 May 26]. Available from:https://www.who.int/news-room/q-a-detail/q-a-coronaviruses
4. Wu P, Fang Y, Guan Z, Fan B, Kong J, Yao Z et al. The psychological impact of the SARS epidemic on hospital employees in China: exposure, risk perception, and altruistic acceptance of risk. Can J Psychiatry 2009;54(5):302-311.
5. Hawryluck L, Gold WL, Robinson S, Pogorski S, Galea S, Styra R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg Infect Dis 2004;10(7):1206-12.
6. Bai Y, Lin CC, Lin CY, Chen JY, Chue CM, Chou P. Survey of stress reactions among health care workers involved with the SARS outbreak. Psychiatr Serv. 2004;55(9):1055-1057.
7. Blendon RJ, Benson JM, DesRoches CM, Raleigh E, Taylor-Clark K. The public's response to severe acute respiratory syndrome in Toronto and the United States. Clin Infect Dis. 2004;38(7):925-31.
8. Wang Y, Xu B, Zhao G, Cao R, He X, Fu S. Is quarantine related to immediate negative psychological consequences during the 2009 H1N1 epidemic? Gen Hosp Psychiatry. 2011;33(1):75-77.
9. Caleo G, Duncombe J, Jephcott F, Lokuge K, Mills C, LooijenE,et al. The factors affecting household transmission dynamics and community compliance with Ebola control measures: a mixed-methods study in a rural village in Sierra Leone. BMC Public Health. 2018;18(1):248.
10. Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS et al. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int J Environ Res Public Health. 2020;17(5):1729.
11.Wang C, Pan R, Wan X, Tan Y, Xu L, McIntyre RS et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun. 2020;0889-1591(20):30511.
12.Chew NWS, Lee GKH, Tan BYQ, Jing M, Goh Y, Ngiam NJH, et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav Immun. 2020:1591(20):30523-30527.
13.Tan BYQ, Chew NWS, Lee GKH, Jing M, Goh Y, Yeo LLL et al. Psychological Impact of the COVID-19 Pandemic on Health Care Workers in Singapore. Ann Intern Med. 2020:M20-1083.
14.Tan W, Hao F, McIntyre RS, Jiang L, Jiang X, Zhang L et al. Is returning to work during the COVID-19 pandemic stressful? A study on immediate mental health status and psycho-neuroimmune prevention measures of the Chinese workforce. Brain Behav Immun. 2020;1591(20):30603-30606.
15. Lovibond S, Lovibond P. Manual For The Depression Anxiety Stress Scales. Sydney. Psyc Found Aust;1996;12(4): 52-58.
16. Weiss D. The Impact of Event Scale: Revised. Cross-Cultural Assessment of Psychological Trauma and PTSD. Psyc Found Aust .1996; 11(5):219-238.
17. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). [cited 2020 May 26]. Available from: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf.
18. Rubin GJ, Wessely S. The psychological effects of quarantining a city. Br Med J. 2020;368:m313.
19. Mohammed A, Sheikh TL, Gidado S, Poggensee G, Nguku P, Olayinka, et al. An evaluation of psychological distress and social support of survivors and contacts of Ebola virus disease infection and their relatives in Lagos, Nigeria: a cross-sectional study-2014. BMC Public Health. 2015;15:824.
20. Tam CW, Pang EP, Lam LC, Chiu HF. Severe acute respiratory syndrome (SARS) in Hong Kong in 2003: stress and psychological impact among frontline healthcare workers. Psychol Med. 2004;34(7):1197-204.
21. Maunder RG, Lancee WJ, Rourke S, Hunter JJ, Goldbloom D, Balderson K et al. Factors associated with the psychological impact of severe acute respiratory syndrome on nurses and other hospital workers in Toronto. Psychosom Med. 2004;66(6):938-42.
22. Lancee WJ, Maunder RG, Goldbloom DS; Coauthors for the Impact of SARS Study. Prevalence of psychiatric disorders among Toronto hospital workers one to two years after the SARS outbreak. Psychiatr Serv. 2008;59(1):91-5.
23. Hong X, Currier GW, Zhao X, Jiang Y, Zhou W, Wei J. Posttraumatic stress disorder in convalescent severe acute respiratory syndrome patients: a 4-year follow-up study. Gen Hosp Psychiatry. 2009;31(6):546-54.
24. Wu KK, Chan SK, Ma TM. Posttraumatic stress after SARS. Emerg Infect Dis. 2005;11(8):1297-300.
25. Mak IW, Chu CM, Pan PC, Yiu MG, Chan VL. Long-term psychiatric morbidities among SARS survivors. Gen Hosp Psychiatry. 2009;31(4):318-26.
26. Lee SM, Kang WS, Cho AR, Kim T, Park JK. The psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Compr Psychiatry. 2018 ;87:123-127.
27.Batawi S, Tarzan N, Al-Raddadi R, Al Qasim E, Sindi A, Al Johni S et al. Quality of life reported by survivors after hospitalization for the Middle East respiratory syndrome (MERS). Health Qual Life Outcomes. 2019;17(1):101.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





