IJCRR - 13(9), May, 2021
Pages: 71-74
Date of Publication: 07-May-2021
Print Article
Download XML Download PDF
Knowledge and Awareness of Children Towards Parental Tobacco Consumption in Central Maharashtra- An Epidemiological Questionnaire-based Study
Author: Sourabh R Joshi, Gowri S Pendyala, Shridhar Shetty, Gargi S Sarode, Sachin Sarode, Kiran Jadhav
Category: Healthcare
Abstract:Introduction: Changes in an individual's lifestyle, not only affects the individual but also his or her surroundings. Parents are generally not aware of the ill effects of their tobacco consumption on the psyche of the child. The affected children are also not generally aware of the ill effects of the passive habit.
Objective: The present study was designed to determine the knowledge and awareness of children towards parental smoking.
Methods: A total of 500 children, between the ages of 10 and 15 years belonging to a similar socio-economic status, from the rural schools in and around Loni were selected for the present study. Information, from these children, was obtained by giving them a questionnaire in the local Marathi language. A Chi-square test was applied to the data obtained and the results were derived.
Results: The obtained results showed that children were highly influenced by parental tobacco use to the extent that they showed the signs of developing the habit themselves.
Conclusion: This study concludes that parental tobacco chewing and/or tobacco habits have a direct detrimental influence on their children.
Keywords: Children’s attitudes, Parental influence, Tobacco chewing
Full Text:
Introduction
During childhood and adolescence, most people develop and establish lifestyles that determine their future health.1 The influence of parental lifestyles is very great on children, since they are at an impressionable age of their lives. Parental Tobacco Chewing is associated with a higher possibility that the child will chew tobacco as well.2 Usage of tobacco products with alcohol and marijuana have been seen among the adolescents.3,4 Associations between use of either tobacco product and corresponding use amongst peers, siblings and parents has also been reported.4,5 Tobacco Chewing is one habit which is dangerous to the health of a person. Since past three decades there has been increasing interest in the effects of passive smoking on children’s health. As children spend much of their early life in the presence of their parents, children whose parents chew tobacco or have any other tobacco habit will have prolonged exposure to tobacco. More than 4000 different components have been identified in cigarette smoke itself.6 Of these, nicotine is a highly toxic alkaloid that is both a ganglionic stimulant and a depressant. Carbon Monoxide, released in tobacco smoke is known to interfere with oxygen transport and supply.6 Tobacco Chewing not only affects the quality of life but also the social well being of an individual. The International Agency for Research on Cancer (IARC) has reviewed that parental tobacco exposure has been associated with prenatal damage to the fetus, adverse respiratory outcomes like asthma, atopy, and allergies among children, coronary heart disease. It also affects the oral health status of children.7,8 WHO estimates 4.9million deaths are annually attributed to tobacco (WHO report 2002). This figure is expected to rise to 10 million in 2030, with 7 million of these deaths occurring in developing countries, mainly, India and China.9 India is home to one-sixth of the global population. Currently about one-fifth of all worldwide deaths attributed to tobacco occur in India, more than 8,00,000 people die and 12 million people become ill due to tobacco. The death rate due to tobacco are expected to rise from 1.4% in 1990, to 13.3% in 2020.9 It is estimated that 5,500 adolescents, inspired by their parents start using tobacco every day in India, joining the 4 million young people under the age of 15 who already regularly use tobacco. Changes in the lifestyle of an individual affect not only his/ her life but also their respective surroundings. Parents may not be aware of the ill effects of tobacco habits on the child’s health as well as his/her psychological development.10 Children are also not very knowledgeable about the same. Thus, this present study was designed to determine the knowledge and awareness of children towards parental tobacco chewing.
MATERIALS AND METHODS
A total of 500 children, between the ages of 10 and 15 years belonging to the same socioeconomic status, from the rural schools in and around Loni were selected for the study, following a simple random sampling method. The study was approved by the Institutional Ethical Committee (PIMS/IEC/DR/2014/180). The demographics of these children are explained in Table 1. Information, from these children, were obtained by giving them a questionnaire in the local Marathi language. A total of 7 questions were framed out of which 3 questions were framed to assess the Knowledge of the students and 4 questions were framed to assess the Awareness of the students towards parental tobacco chewing. Questions were added to include parental tobacco use in the form of smokeless or smoked tobacco and bidi smoking. The questionnaire was presented among young boys and girls in Loni. Data on age, gender, grade, parent’s education and occupation, current use of tobacco products among students, knowledge, and awareness regarding the use of tobacco and tobacco products were obtained using a semi-structured questionnaire. The sequencing of the questions was logical. The questions were administered without any identifying information, skipping or branching pattern. The contents of the questionnaire were validated by a trained Medical Health Professional. The responses collected were kept confidential to the authors themselves. Informed consent was obtained by the guardians (teachers) of the school.
Statistical analysis
Chi-square test was applied to the data received and the results were formulated.
Results
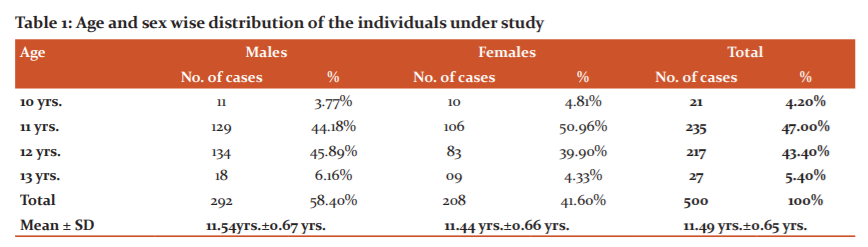
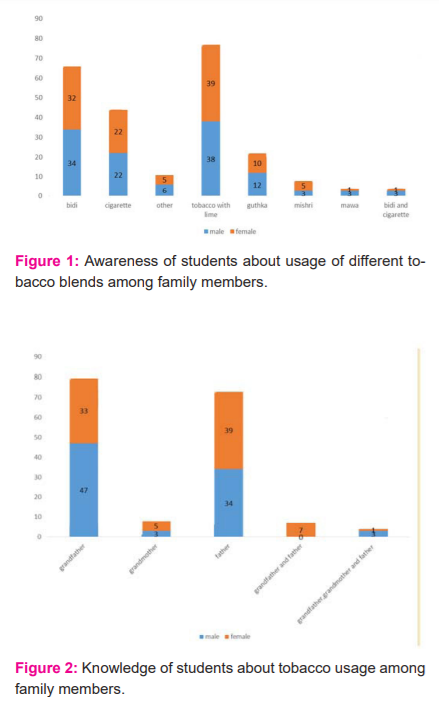
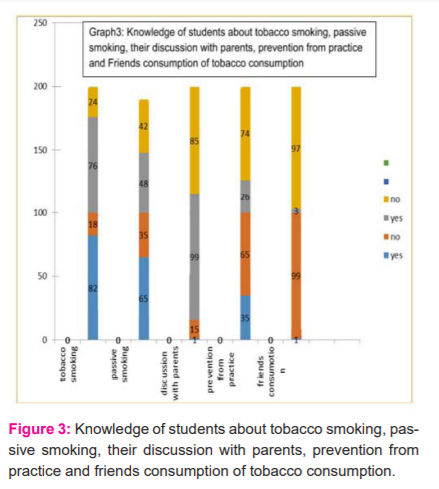
The subjects eligible for the survey were 500 children between the ages of 10 and 15 years. In the following study, all the questionnaires given were returned with the required information (100%). Out of 500, 292 were boys (58.4%) and 208 were girls (41.6%). The mean age of the children was about 11.49 years (Table 1). After obtaining all the required data, the Chi-Square test was applied and the following results were obtained regarding the Knowledge and awareness of the children towards familial tobacco habits. The highest percentage of adults with tobacco habits were the Fathers at 35.8% and Grand Fathers at 42% (Figure 2). The most common type of smoking tobacco in the chosen area was seen to be Bidi at 33% and the most common smokeless form was tobacco with lime at 38.2% (Figure 1). It was seen that about 81.84% of boys and 76.44% of girls knew that a tobacco habit was harmful to health (Figure 3). It was also noted, that around 64.72% of boys and 48.8% of girls knew that passive tobacco inhalation was equally harmful to their health as well. About 98.29% of boys and 95.67% of girls had not discussed the ill effects of tobacco with their parents/guardians (Figure 3). The questionnaire covered the children’s perspective towards familial tobacco habits as well, as the obtained results are as follows;
More than 30% of the children tried to prevent the tobacco habit at home but nearly 70% couldn’t prevent their parents from tobacco consumption (Figure 3). Almost all the children agreed and were aware that public smoking or practising any form of tobacco smoking or smokeless should be banned (Figure 3). Less than 4% of the children also had friends practising the habit (Figure 3).
Discussion
Consistent with previous studies on tobacco use risk factors, this study supports the importance of addressing awareness and, knowledge of children regarding familial tobacco use. From this study, it was clear, that the children were well aware of their parents and relatives have a tobacco habit and were greatly influenced by the same. In our study, most children were heavily and negatively influenced, as it was seen that most have developed the habit themselves due to prolonged exposure passively. Prior research by Murray et al.4 has shown that both general parenting behaviours and smoking-specific parenting practices contribute to adolescent smoking behaviours. A study done by Horn et al. 5 and Chassin et al. 5,11 showed that inadequate knowledge about tobacco and health, tobacco use among family and friends, favourable attitude towards tobacco use were important determinants of tobacco use among adolescents. The 2013 survey done in India also observed that favourable parental tobacco use was a significant risk factor for the uptake of the habit in children.12 In our study, it was clear that the tobacco habit was practised more in front of the boys as compared to the girls. It was also seen that they had more information and were relatively easily influenced by their parents and relatives. A study carried out by Ballal et al. 13 among 13 to 19 years, found knowledge among females to be better than males about tobacco consumption habits. From our study, we could conclude that boys and girls were aware of tobacco chewing habits. One of the positive outcomes of this study was the awareness of the children towards practising the tobacco habit. Almost all of the children agreed that it was imperative to ban public smoking or practising any form of tobacco habit. Children also tried to prevent the habit among their relatives but a very less percentage could attempt it. There was also a visible attempt to prevent and control this habit taken up by the children themselves, which goes to show that the children were better aware of the ill effects of tobacco due to external influences such as school and their peers. It was also clearly seen that there was no significant relationship between the influences of practising tobacco amongst friends.
Conclusion
Many of the parents, guardians and relatives had an excessive habit and the ill- effects were not openly discussed with the children. Despite the children trying to prevent this habit, no clear action was taken in the family to stop or control the habit. This study concludes that parental tobacco chewing and/or tobacco habits have a direct influence on children. Pro-tobacco behaviour of the parents and relatives has a heavy negative influence on the child since the child picks up on the habit and develops the habit for himself/ herself as well. It is thus advisable for parents and guardians to terminate the habit and lead by example to prevent their children from getting addicted to tobacco.
Future Perspectives
The present study highlights the effects of tobacco consumption by parents on children. Though this study highlights childrens’ knowledge and awareness about parental tobacco consumption, more studies are required to understand children's awareness towards parental tobacco consumption.
CONFLICT OF INTEREST: None
FINANCIAL DISCLOSURE: This is a self-funded project.
AUTHORS CONTRIBUTION:
-
Dr Sourabh Joshi helped in carrying out the study by visiting the schools.
-
Dr Gowri Pendyala helped in collecting the data.
-
Dr. Gargi Sarode contributed to creating the concept.
-
Dr. Sachin Sarode contributed by designing the study.
ACKNOWLEDGEMENT: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed."
References:
1. Rossow I, Rise J. Concordance of parental and adolescent health behaviours. Soc Sci Med 1994;38(9):1299–1305.
2. Tyas SL, Pederson LL. Psychosocial factors related to adolescent smoking: a critical review of the literature. Tob Control 1998;7(4):409–420.
3. Simon T, Sussane S, Dent C. Correlates of exclusive or combined use of cigarettes and smokeless tobacco among male adolescents. Addict Behav 1993;18(1):623-634.
4. Murray DM, Roche LM, Goldman AI, Whitebeck J. Smokeless tobacco use among ninth graders in a north-central metropolitan population: Cross-sectional and prospective associations with age, gender, race, family structure, and other drug use. Prev Med 1988;17(4):449–460.
5. Horn KA, Gao X, Dino GA, Kamal-Bahl S. Determinants of youth tobacco use in West Virginia: a comparison of smoking and smokeless tobacco use. Am J Drug Alcohol Abuse 2000;26(1):125–138.
6. Raherison C, Pénard-Morand C, Moreau D, Caillaud D, Charpin D, Kopfersmitt C, et al. In utero and childhood exposure to parental tobacco smoke, and allergies in schoolchildren. Respir Med 2007;101(1):107–117.
7. Barnes DE, Bero LA. Why review articles on the health effects of passive smoking reach different conclusions. J Am Med Assoc 1998;279(19):1566–1570.
8. Fleming P, Blair PS. Sudden Infant Death Syndrome and parental smoking. Early Hum Dev 2007;83(11):721–725.
9. Patel DR. Smoking and children. Indian J Pediatr 1999;66(6):817–824.
10. Rainio SU, Rimpelä AH. Home smoking bans in Finland and the association with child smoking. Eur J Public Health 2007;18(3):306–311.
11. Chassin L, Presson CC, Sherman SJ, Edwards DA. Parent educational attainment and adolescent cigarette smoking. J Subst Abuse 1992;4(3):219–234.
12. Dhawan A, Pattanayak RD, Chopra A, Tikoo VK, Kumar R. Pattern and profile of children using substances in India: Insights and recommendations. Natl Med J India. 2017;30(4):224–9.
13. Ballal K, Kulkarni M, Agrawal A, Kamath A, Kumar M. Knowledge and attitude regarding tobacco and its use among adolescent students. Natl J Community Med 2016;79(5):519-513.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





