IJCRR - 13(7), April, 2021
Pages: 132-137
Date of Publication: 12-Apr-2021
Print Article
Download XML Download PDF
Efficacy of Maitland Mobilization and Conventional Treatment in Patients of Osteoarthritis of Knee
Author: Subrat Samal, Shweta Panchbudhe, Snehal Samal, Mohini Dixit, Vasant Gawande
Category: Healthcare
Abstract:Background: Osteoarthritis (OA) of the knee is the most common type of arthritis and the leading cause of disability that impacts the elderly and middle-aged worldwide. Maitland mobilization reduces pain, improves range of motion and functional disability. Conventional treatment reduces pain and improves the range of motion of the knee joint. Objective: To study the effects of Maitland mobilization and Conventional treatment on Pain, Range of Motion and function dis�ability inpatient with osteoarthritis with a knee. Method: 72 subjects (36 in each group), Interventional study Sample and Sampling Method: 72 subjects were randomly se�lected and assigned in two groups, Group A (Maitland mobilization) and Group B (Conventional) in equal numbers. A total num�ber of 72 subjects were included in the study as per the inclusion and exclusion criteria. Kellegren and Lawrence grade 1 and 2 radiographic evidence of osteoarthritis, BothGenders, Age between 40 to 60years, Knee osteoarthritis with duration ≥ 1 year, Average knee pain ≥3 on Visual AnalogScale,Subjects with Unilateral knee joint, Tibiofemoral and Patellofemoral knee joint, Tenderness over kneejoint. Acute exacerbation in or around kneejoints, Traumatic injury to knee joints within 6 months of study, Any surgical intervention to the kneejoints, Intra-articular steroid injection in knee joints within 3months, Subject with Psychiatric disorders/Illness, Peripheral vascular disease, Tumors/malignancies/infections associated with kneejoint. lower limb metallic implants, Impaired thermal sensation over the knee. Results: Results showed statistically significant improvement in both groups for VAS, ROM and functional disability by using student's Paired and unpaired t-test. Group A showed more significant improvement than Group B. Conclusion: In conclusion, Maitland Mobilization and Conventional therapy are more effective than conventional treatment alone in relieving pain, improving range of motion and functional well-being in subjects with knee osteoarthritis.
Keywords: Osteoarthritis, Maitland Mobilization, Conventional treatment, Knee joint
Full Text:
INTRODUCTION
Osteoarthritis (OA)is the most common type of arthritis and the leading cause of disability that impacts the elderly and middle-aged worldwide.1 OA is a multifactorial entity that includes several causative factors such as Trauma, Mechanical forces, Inflammation, Biochemical responses and Metabolic disturbances.2,3 The incidence of OA knee in rural and urban India is 3.9% and 5.5%.4 It is recorded to be 5.78% and 10.20% respectively in Bangladesh and India. According to research in Pakistan, 28% of the metropolitan population and 25% of the rural population have knee arthritis.5 The meta-analysis also revealed that women tend to be graphically evaluated with more serious knee OA radiographically than men, and sex differences boost with age > 55 years.6
Osteoarthritis is a complex disease whose pathogenesis involves the contribution of biomechanical and metabolic variables that alters articular cartilage and subchondral bone homeostasis of the tissue and determine the predominance of destructive over productive procedures. The end products of cartilage emerge out and the cell lining the joint will attempt tore move them. The small bony formation “spur” will be formed in the lining of the articular surface. The physical findings of Osteoarthritis of the knee include: bony enlargement, crepitus, decreased range of motion, joint-line tenderness, and pain on passive range of motion.7
The cause of osteoarthritis is repetitive mechanical loads and aging.Decreased strength in the muscle group involving the joints which it causes significant progressive loss of function.There are two terms of Mobilization and Manipulation, but they have the same meaning and can be changed. The variable speeds and amplitude can vary from a small- amplitude force applied at quick velocity to a big amplitude force applied at slow velocity, a continuum of intensities and velocity could be applied to the method.8,9
Gentle Joint mobilization can be used by stimulating neurophysiological and mechanical effects to treat pain and muscle guarding. In neurophysiological effects, small oscillatory amplitude and distraction motion are used to boost mechanoreceptors which can prevent the transmission of nociceptive stimuli at the level of the spinal cord or brainstem.10-13
This study is carried out to find out that which treatment is effective i.e.Maitl and Mobilization or Conventional treatment in reducing Pain, ROM, functional impairment in OA knee patients.
MATERIALS AND METHODS
Materials used are treatment table, universal half-circle goniometer, Hydro collateral packs, stellium, cotton and talcum powder.
Collection of data
Seventy-two (72 subjects) of 40 to 60 years of age with a history of pain, tenderness and diagnosed with knee osteoarthritis were taken and screened by the inclusion criteria in the study and assessed for pain, range of motion and functional activity using the visual analogue scale, universal Goniometer, WOMAC Scale. Patients were randomly divided into two groups. Group A(36 subjects will receive Maitland Mobilization with conventional therapy) and Group B(36 subjects will receive conventional therapy alone).14,15
72 healthy subjects(16 male and 56 female) with osteoarthritis of the knee participated in the study. The subjects were recruited from the Department of Musculoskeletal Sciences, Ravi Nair Physiotherapy College, Sawangi (Meghe), Wardha after approval from the Institutional Ethics Committee of Datta Meghe Institute of Medical Sciences, Deemed to be University.
Study Design: Interventional study.
Study Setting: OPD of Musculoskeletal Sciences, Ravi Nair Physiotherapy College, Sawangi, Wardha.
Sample size: Total of 72 subjects.
Study Duration: 6 weeks
Sampling Technique: Subjects were selected Randomly Allocated by chit method and assignedin2groupssuchasGroupA(Experimental group)andGroupB(Control group) in equal number (36 subjects in each groups).
Inclusion Criteria
-
Kellegren and Lawrence grade 1 and 2 radiographic evidence of osteoarthritis
-
Both Genders
-
Age between 40 to 60years
-
Knee osteoarthritis with duration ≥ 1 year.
-
Average knee pain ≥3 on Visual Analog Scale.
-
Subjects with Unilateral knee joint.
-
Tibiofemoral and Patellofemoral knee joint
-
Tenderness over kneejoint
-
Patient with tightness in Quadriceps, Hamstring, and Iliotibial band.
Exclusion Criteria
-
-
-
Acute exacerbation in or around kneejoints.
-
Traumatic injury to knee joints within 6 months of study.
-
Any surgical intervention to the kneejoints.
-
Intra-articular steroid injection in knee joints within 3months.
-
Subject with Psychiatric disorders/Illness.
-
Peripheral vascular disease.
-
Tumours/malignancies/infections associated with kneejoint. lower limb metallic implants.
-
Impaired thermal sensation over the knee.
Procedure
The institutional ethics committee clearance DMIMS(DU)/IEC/2018-19/7193was obtained to conduct the study. Initially the patient was thoroughly evaluated. After satisfying inclusion and exclusion criteria the patient was allowed to participate in the study. The patients who willingly volunteered for the study were included and the purpose was explained. Total 76 OA knee subjects were screened for the inclusion and exclusion criteria of the study, out of which 4 subjects were not willing to continue treatment. Therefore 72subjects were included in this study. The procedure was well explained to all the eligible subjects and they were given informed consent (n=72) before allocating them into two groups. After randomization, they were divided into two groups- Group A (n=36) and GroupB(n=36)The preassessment were take non(0Day)and post-assessment was taken at the end of 6thweek for all outcome measures such as the Visual Analog Scale (VAS) for pain, Goniometer for ROM, WOMAC Scale for functional activities test.
In Group A subjects (Experimental) received Maitland mobilization along with conventional treatment. In Group B subjects (Control) received Conventional treatment alone. Patients were instructed to perform a home exercise program which was taught to them on the first assessment day.
Group A subjects received Grade I, II and III Maitland Mobilization.
Maitland mobilization for tibio femoral joint
-
Tibio femoral Distraction
-
Tibio femoral Posterior Glide (To increase flexion)
-
Tibio femoral Anterior Glide (To increase the extension)
-
Patello femoral Joint, DistalGlide
To maintain patellar mobility for normal knee flexion
Group B- Conventional Therapy
In conventional physiotherapy, subjects were receiving physical modalities such as Hydro collateral packs to reduce pain.
-
StaticQuadriceps
-
Static Hamstringcontraction
-
VMO (strengthening of vastus medialis)
-
Dynamic quadriceps
-
Wall slides
-
Partial lunges
-
One leg standing16,17
Home Exercise Programme
-
Self-stretching of Quadriceps muscle
-
Self- stretching of Hamstring muscle
-
Self -stretching of Calf muscle
Outcome Measures
-
Visual analogue scale
-
Knee flexion range of motion on universal Goniometer
-
WOMAC scale for functional disability. 18,19
RESULTS
The data was coded and entered into a Microsoft Excel spreadsheet. Descriptive statistics included computation of means and standard deviation. Inferential statistics using student’s paired ‘t’ test (for the quantitative data to comparepre and post observation)and unpaired t-test (for quantitative data to compare within two groups) were used for comparis on of all clinical indicators.SoftwareusedintheanalysiswasSPSS22.0version. The results were concluded to be statistically significant with p < 0.05, very significant < 0.001 and highly significant p < 0.0001 (Table 1).
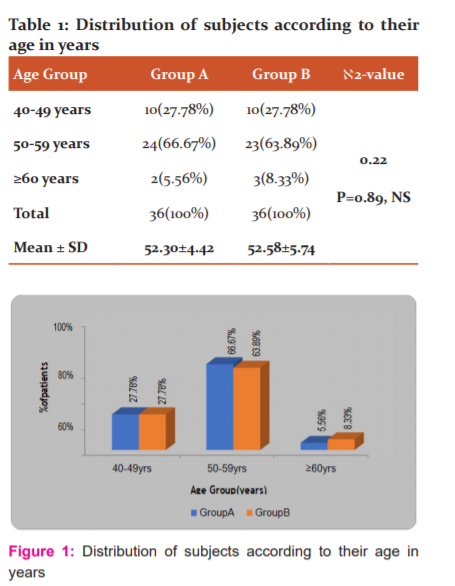
Table 1 and Graph 1 shows age wise distribution of subjects. 10(27.78 %) in group A and 10(27.78%)ingroupBsubjectswereintheagegroupof40-49years,24(66.67%)ingroup A and 23(63.89%) subjects in group B were in the age group of 50-59 yrs. Less than 60 years,2(5.56%) in group A and 3(8.33%) in Group B .The mean age of the subjects in groupAwas52.30 ±4.42andin groupBitwas52.58±5.74. Byusingchi-squaretestno significant difference is found in the ages of subjects of in all threegroups
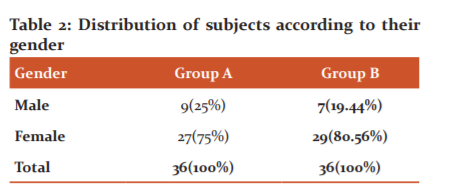
Table 2 Shows gender-wise distribution of subjects. There were 9(25%) in group A and 7(19.44%) male subjects in group B, 27 (75%) in Group A and 29(80.56%)female subjects in Group B. By using chi-square test no significant differences in found among the gender of both the group.
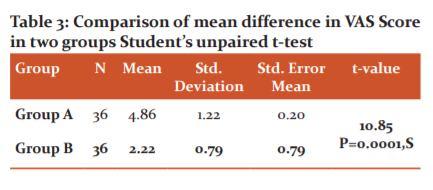
Table 3 shows the comparison of pain on VAS in both group A and group B.Mean pain on VAS in Group A was 4.86±1.22 and in Group B was 2.22±0.79. By using student’s unpaired t-test showing a significant difference in both groups but Group A shows more reduction of pain than Group B. Hence, Group A shows a significant improvement in pain reduction than Group B.
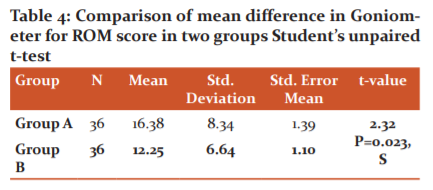
Table 4 shows the comparison of pain ROM on the Goniometer in both groups A and group B. Mean ROM on the goniometer in Group A was 16.38±8.34 and in Group B was 12.25±6.64. By using student’s unpaired t-test showing a significant difference in both groups.(t=2.32,P= 0.023) but Group A shows a mean increase in range of motion as compared to Group B. Hence Group A is showed a more significant result in knee flexion as compared to Group B.
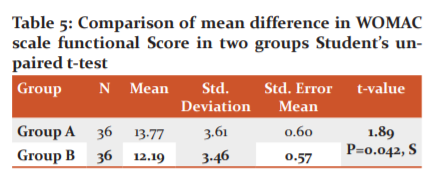
Table 5 shows the comparison of the functional disability scale on the WOMAC scale score in both groups. Mean of functional disability scale on WOMAC scale score Group A was 13.77±3.61and in Group B was 12.19±3.46. By using students unpaired t-test showing a significant decrease in functional disability scale on WOMAC scale (t=1.89, P=0.062) but Group A shows a significant decrease in functional disability than Group B. Hence, Group A shows significant improvement than Group B.
DISCUSSION
The current research was conducted to determine whether Maitland Mobilization and Conventional treatment are efficient in knee osteoarthritis subject in the Department of Musculoskeletal Physiotherapy.20,21 The outcome of this research shows that Maitland Mobilization with conventional therapy is more efficient in knee osteoarthritis. The mean data values from this research indicate that group A treated with Maitland Mobilization showed better improvement in Visual Analog Scale Pain relief, increased range of motion, WOMAC scale Physical functional ability.22,23
Table 1. showed age-wise distribution of topics in the current research. No important difference is discovered in the age of participants in both the group by using the chi-square test. The same number of subjects were affected by both the group and the maximum age group was 50-59 years in the study. Mathur et al.15 revealed that 15-40% of people over 40 years of age affected by degenerative joint disease, so it can be predicted that the most prevalent age group with the degenerative joint disease between 40 and 60 years of age.
Table 2 illustrates the wise gender distribution of subjects. By using the chi-square test, there is no significant difference between the two groups. In this research, Zakir et al.24 found that both male and female OA knee subjects but observed that the percentage of male subjects (40.7 per cent) was small than female subject (59.3percent).Because of multiple factors,owing to its greater prevalence in the female population, this study had a big amount offemalesubjects (59.3).the female bony structures around the knee are different from the malecounter parts.
Analysis of pain relief was ended by subjective visual analogue scale (VAS) by statistical mean. When Intragroup comparison was done there is a significant difference in both groups i.e. Group A and Group B. When intergroup comparison was done within both groups there was a significant difference, where group A showed significant improvement in terms of VAS.25,26
Mathur et al.15 studied the effectiveness of Maitland mobilizationin decreasing the knee joint pain.In earlier research,pain-decrease following passive joint mobilization has been already been stabilized.Mobilization may trigger local physiological processes and may also involve extra main procedures. These key mechanism could include activating the local inhibitory pathway in the spinal cord or lowering the inhibitory pathway from the brainstem.
Analysis of knee flexion was completed by subjective Goniometer by statistical mean. When Intragroup comparison was performed there is a significant difference in both groups i.e. Group A and Group B. When intergroup comparison was done within both groups there was a significant difference, where group A showed significant improvement in terms of the range of motion for knee flexion.
Analysis of Functional Disability was conducted by subjective WOMAC scale by statistical mean. When Intragroup comparison was done there is a significant difference in both groups i.e.groupAandgroupB.Whenintergroupcomparisonwasdone within both groups there was a significant difference, where group A showed significant improvement in terms of the WOMAC scale. Syed et al. 201427 showed a 56 per cent increase in complete WOMAC results in disability after administering manual physical therapy and knee osteoarthritis. However, in this study, the myofascial mobilization group and Conventional treatment group respectively noted 56.35% and 52% improvement in WOMAC scores and reported the effectiveness of Myofascial mobilization at the knee joint in reducing knee OA pain and disability.Dueto mechanical power during mobilization, including breaking Adhesions, Realigning collagen, or growing fibre glide, the efficacy of two therapy protocols can be reasonable when a particular motion stresses the particular component of the capsule. Ahmad et al.5 researched that manual techniques and exercises generated an average 56 per cent rise in self-reporting functional capacity of 54 per cent, stiffness of 54 per cent, and pain of 60 per cent as measured by the (WOMAC) scales.
Knee osteoarthritis presents a serious health issue and a huge burden on society. Simple, safe, physical treatment procedures like Maitland Mobilization and conventional exercises could be of great value. This provides low-cost, easy means of treatment in subjects with knee osteoarthritis.
CONCLUSION
In conclusion, the present study provided evidence to support the use of physical therapy regimen in the form of Maitl and Mobilization with Conventional therapy is more effective than conventional treatment alone in relieving pain, improving range of motion and functional well-being in subjects with knee osteoarthritis.
Conflict of Interest: Nil
Source of Funding: Nil
References:
-
Xu Q, Pang J, Zheng Y, Zhan H, Cao Y, Ding C. The effectiveness of manual therapy for relieving pain, stiffness and dysfunction in knee osteoarthritis: A systematic review and meta-analysis. Osteoarthr Cartil 2015;23:A387.
-
Mora JC, Przkora R, Cruz-Almeida Y. Knee osteoarthritis: pathophysiology and current treatment modalities. J Pain Res 2018;11:2189–96.
-
Kiran A, Ijaz M, Qamar M, Basharat A, Rasul A, Ahmed W. Comparison of the efficacy of mulligan’s mobilization with movement with Maitland mobilization along with conventional therapy in the patients with knee osteoarthritis: A randomized clinical trial. Libyan Int Med Univ J 2018;3(1):26.
-
Rangey PS, Sheth MS, Vyas NJ. Comparison of Immediate Effect of Two Different Maitland Mobilization Protocols on Pain and Range Of Motion in Subjects with Osteoarthritis of Knee. Int J Med Health Res 2019; 3:124-127.
-
Ahmad A. A Comparative Study between Joint Mobilization and Conventional Physiotherapy in Knee Osteoarthritis. Int J Physiother 2016;3(2):542-546.
-
Hafez AR, Mohammed A, Kachanathu SJ, Alroumi M, Mohamed ES. Knee Osteoarthritis: A Review of Literature. Int J Physiother 2018;5(2):81-84.
-
Arshad S, Rizvi SHA, Nisar M. To Evaluate the Effectiveness of Maitland Technique in Treatment of Knee Osteoarthritis in Female Patients. Int J Health Sci Res 2017;5(2):30.
-
BD Chaurasia’s Human Anatomy, Volume 2 – Lower Limb, Abdomen and Pelvis, 6th Edition.pdf.
-
Levangie PK, Norkin CC. Joint structure and function: a comprehensive analysis. 4th ed. Philadelphia. 2005;4:588.
-
Kisner C, Colby LA. Therapeutic exercise: foundations and techniques. 5th ed. Philadelphia.2007;2: 928.
-
Bennett R. Myofascial pain syndromes and their evaluation. Best Pract Res Clin Rheum 2007 Jun;21(3):427–445.
-
Rickards LD. The effectiveness of non-invasive treatments for active myofascial trigger point pain: A systematic review of the literature. Int J Osteopath Med 2006;9(4):120–136.
-
Mathur DMK. Comparison Between Passive Joint Mobilization And Manual Therapy Knee Protocol On Pain, Function And Quality Of Life In Patient With Chronic Osteoarthritis of Knee. Int J Osteopath Med 2018;8(2):58-62.
-
Shukla M, Goyal M, Effect of maitland mobilization and conventional physiotherapy exercises in osteoarthritis knee: a comparative study. Int J Physiother Res 2018;6(6):2952–2958.
-
Jung J, Choi W, Lee Y, Kim J, Kim H, Lee K, et al. Immediate effect of self-myofascial release on hamstring flexibility. Phys Ther Rehabil Sci 2017;6(1):45–51.
-
Vaishnavi KS, Rajeeva A. A comparative study of Maitland's mobilization along with ultrasound versus proprioceptive exercises along with ultrasound in stage ii and iii osteoarthritides of the knee joint. Int J Physical Edu.2017; 4(6):211-215.
-
Muhammad N, Noreen A. GRADE 1-2 Osteoarthritis Of Knee Joint; Outcome Of Combination Of Grade 1-2 Knee Joint Mobilization With Quadriceps Isometrics In Patients. Profess Med J 2017;24(7):986-991.
-
Ganesh B. Short term effects of instrument-assisted soft tissue mobilization on pain and activities of daily living in subjects with patellofemoral joint osteoarthritis – A randomized controlled trial. Int J Curr Res Med Sci. 2017 Nov 30;4(11):55–63.
-
Shah JP, Thaker N, Heimur J, Aredo JV, Sikdar S, Gerber L. Myofascial Trigger Points Then and Now: A Historical and Scientific Perspective. Int J Curr Res Med Sci 2015;7(7):746–761.
-
Zakir A. Effectiveness of Manual Therapy Versus Exercise Therapy for the Management of Knee Osteoarthritis in Karachi Pakistan. Int J Physiotherapy 2016;3(1):57-62.
-
Hhabar, P. Sathya HKC. Effect of Conventional Exercises with Balance Training & amp; Only Conventional Exercises in Patients with Osteoarthritis of Knee. Int J Innov Res Sci Eng Tech 2015;04(07):5048–5056.
-
Ebtessam Fawzy G, Lilian Albert Z. Effect of iliotibial band myofascial release on flexibility and patellar alignment in patients with knee osteoarthritis. Int J Adv Res 2015;3(4): 399-410.
-
Syed S, Wani S. Effect of Two Different Manual Therapy Protocols On Osteoarthritic Knee Pain & Functional Disability: A Comparative Study. Int J Adv Res 2014;20(34):10.
-
Jansen MJ, Viechtbauer W, Lenssen AF, Hendriks EJM, de Bie RA. Strength training alone, exercise therapy alone, and exercise therapy with passive manual mobilisation each reduce pain and disability in people with knee osteoarthritis: a systematic review. J Physiotherapy. 2011;57(1):11–20.
-
Swati K, Subhash K. Effectiveness between supervised clinical exercise with Maitland manual therapy and home exercise program in treating osteoarthritis of the knee: a comparative study. Ind J Basic and App Med. 2013;3(1): 105-112.
-
Harish S, Kashif R. Effect of Maitland Mobilization and Myofascial Release Technique in Patients with Knee Osteoarthritis. Indian J Physiother Occup Ther Int J 2013;7(4):181.
-
Maher S, Creighton D, Kondratek M, Krauss J, Qu X. The effect of tibio-femoral traction mobilization on passive knee flexion motion impairment and pain: a case series. J Man Manip Ther 2010 Mar;18(1):29–36.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





