IJCRR - 13(4), February, 2021
Pages: 152-156
Date of Publication: 16-Feb-2021
Print Article
Download XML Download PDF
A Case Study on Management of Complex Renal Calculi (Mutrashmari) by Ayurvedic Formulation
Author: Wairagade SD, Nagrare AV, Wairagade T, Umate K, Lamture Y
Category: Healthcare
Abstract:Introduction: Kidney stone disease should be viewed as a systemic disorder, associated with hypertension, insulin resistance, chronic kidney disease and cardiovascular damage. Mutrashmari (Renal calculi/ Kidney stones) is one among the Ashtamahagada (eight fatal conditions) and is Kaphapradhan Tridoshaja Vyadhi. It is correlated with urolithiasis. The prevalence of symptomatic urolithiasis is approximately 10 per cent in men and 5 per cent in women. Many treatment modalities have been introduced in medical sciences, but it is very costly and even the recurrence of production of stone cannot be prevented. Objectives: To find out easily available, a cost-effective medicine to treat Mutrashmari. The available treatments options for prevention of stone recurrence can be divided into lifestyle interventions and pharmaceutical therapies. Case Presentation: In the first follow-up; the patient informed the stone was expelled out through urine, and he experienced moderate pain and disturbance in the urine flow on 30th day. The patient got moderate relief from pain in the abdomen and did not experience dysuria. Conclusion: Our present findings suggest that Chandraprabha Vati, Ayurvedic Formulation Tablet, Varunadi Kshaya is a safe and effective approach for the management of patients with renal stones.
Keywords: Renal calculi, Mutrashmari, Shaman Chikitsa, Ayurvedic formulation, Urolithiasis
Full Text:
INTRODUCTION
Dietary and lifestyle changes represent an important strategy for the prevention of kidney stone recurrences and cardiovascular damage.1 Stones that grow in the urinary tract (recognized as nephrolithiasis or urolithiasis) form when the urine becomes excessively supersaturated concerning a mineral, leading to crystal formation, growth, aggregation and retention within the kidneys.2 Worldwide, approximately 80% of kidney stones are composed of calcium oxalate (CaOx) mixed with calcium phosphate (CaP). Stones composed of uric acid 9%, struvite 10% and cystine of 1% are common.3
Renal calculi (Kidney stones) are mineral densification in the renal calyces and pelvis that are found free or attached to the renal papillae.4 In our country kidney stone comprise one of the commonest diseases. Pain due to kidney stones is recognized as worse than that of labour pain. The information regarding Ashmari5 is available in almost all Samhita of Ayurveda. In India, approximately 5-7 million patients suffer from stone disease6,7 and at least one from 1000 patients of Indian population needs hospitalization due to kidney stone disease. Thus, the disease is as common as it is old, particularly in countries with hot and dry climate.8 These are “stone belt regions”. The incidence of calculi varies as per geographical distribution, sex and age group. The reappearance rate is 60 to 80%. Males are more commonly affected than the female with their ratio is 4:3.9 The incidence is higher in the age group between30-45 years and incidence diminishes after the age of 50 years.
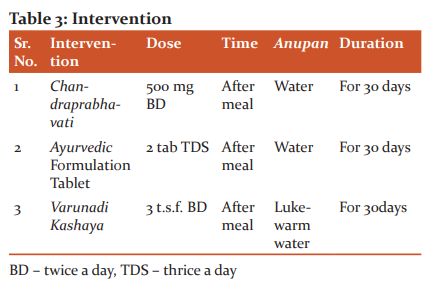
Many medicinal formulations mentioned in Ayurvedic literature for the management of Mutrashmari, are cost-effective, devoid of complications and provide wide scope for the successful treatment of Urolithiasis. Formation of calcium oxalate stones has been found significantly reduced by a small reduction in urinary oxalate. Hence, oxalate-rich foods like cucumber, beetroot, spinach, soya bean, chocolate, popcorn, and sweet potato should be avoided. Many studies have established calcium restriction increase the risk of stone disease; therefore, dietary calcium restriction is not suggested. Fluid consumption and dietary improvements are effective steps in avoiding kidney stone recurrence. Several studies have shown that increasing urine volume to at least 2 L/day OR 2 lit/day will decrease stone disease recurrence by up to 40-50 per cent.10 The consumption of fluids should primarily involve water. As tea and coffee contain oxalate, it is essential to add milk (which binds free oxalate) to them. Increasing the amount of urine, however, has a downside of lowering urinary citrate. The patient is given Chandraprabha vati which promotes strength and immunity, Ayurvedic formulation tablets which are used in urinary retention, dysuria, renal calculi, hematuria, and burning in urination due to acidic urine and Varunadi Kashaya which is capable of lithotriptic action, reducing pain intensity, dysuria and is also capable of reducing haematuria.
MATERIALS AND METHODS
It is a single analysis of a case and the patient's informed consent is taken in his language.
History of Present Illness
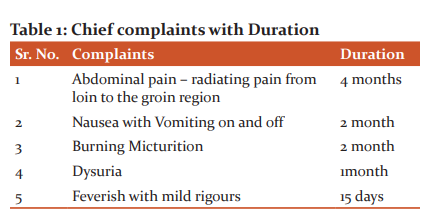
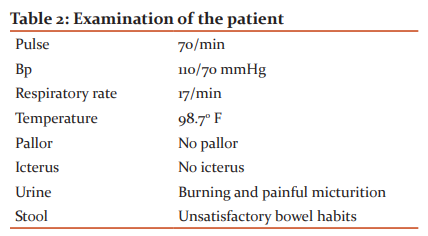
Before 4 months, a 36-year-old man was in a good state, then he started to complain of abdominal pain and it was discovered that the pain was sporadic and colicky and it was present on the right side of the abdomen, which radiated from the loin to the groin area; difficulty urinating normally at the start of pricking type urination; often burning micturition. These chief complaints are briefly mentioned in Tables 1 and 2.
Demographic Details:
The patient aged 36 years (male) visited to our hospital on 05/10/2020.
OPD Registration no. 2010060014
Treatment Advised
By analyzing the above pathogenesis of disease in this patient following Shaman Chikitsatreatment plan was prescribed (Table 3).
Assessment of Patient
Overall assessment of the therapy was made based on the improvement in pain, Mutra Pravrutti and ultrasonography (USG) finding.
Assessment parameter
Objective parameters
USG of KUB was done before (0 days) and after the intervention (30th Day) for the assessment of change in the size of urinary calculi.
Subjective parameter
The assessment was done before (0day) and after the intervention (30thday) based on grading of symptoms as follows.
Assessment of the overall effect of therapy
The overall effect of the therapy was assessed by adopting the following criteria.
-
Complete Remission: 100% relief in Chief complaints and absence of renal calculi in USG of KUB.
-
Marked improvement: >75% and <100% improvements in chief complaints and decrease in size of the stone was recorded as a marked improvement.
-
Moderate improvement: <75% and >50% improvement in chief complaints and decrease in size of the stone was recorded as a moderate improvement.
-
Mild improvement: <50% and >25% improvement in chief complaints and reduction in the size of the stone was considered as a mild improvement.
-
No improvement: <25% improvement in chief complaint sand reduction in the size of the stone was recorded as no improvement.
RESULTS
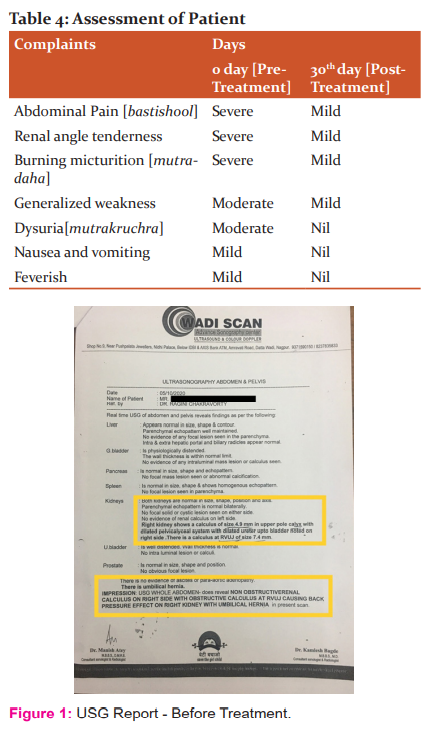
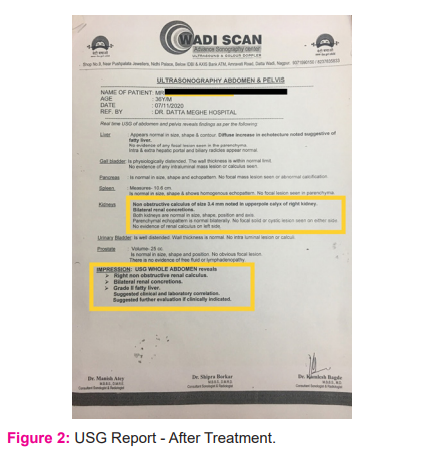
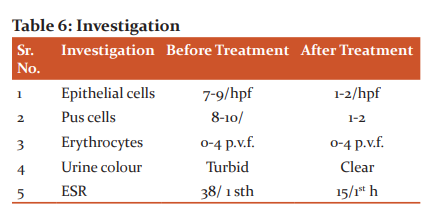
In the first follow-up; the patient informed the stone was expelled out through urine, and he experienced moderate pain and disturbance in the urine flow on 30th day. The patient got moderate relief from pain in the abdomen and did not experience dysuria (Figure 1 and 2). Other assessment of before and after observation is mentioned in Table 4, 5 and 6 and Figure 1 and 2.

DISCUSSION
The intervention was found to be very effective in calculus of about 4.9mm in Right upper pole calyx and dilated ureter upto bladder noted on right side with obstructive calculus of size 7.4mm at RVUJ (Right Vesicoureteric Junction) causing back pressure effect on right kidney with umbilical Hernia. This combination of drugs found to be very effective in reducing the symptoms of mutrashmarii. ebastishoola, mutrakrichrata and mutradahawithin 30 days.
Chandraprabha Vati is a potent anti-inflammatory Ayurvedic remedy used for the treatment of diseases of the urinary tract, kidney, pancreas, thyroid gland, bones and joints. ‘Chandra’ signifying ‘moon’ and ‘Prabha’ denoting ‘glow’, Chandraprabha Vati brings a glow to your body and promotes strength and immunity. Ayurvedic Formulation Tablet contains Shilapuspha (Didymocarpuspedicellata) 130mg, Pasanabheda (Saxifagalgulata Syn. Bergenia ligulata/ciliata) 98 mg, Manjishtha (Rubia cordifolia) 32 mg, Nagarmusta (Cyperus scariosus) 32 mg, Apamarga (Achyranthes Aspera) 32 mg, Gohija (Onosmabracteatum) 32 mg, Sahadevi (Vernonia cinerea) 32 mg, Shilajeet (Purified) 26 mg, Punarnava, Ushira, Shweta Parpati and HajarulyashoodBhasma which is used in urinary retention, dysuria, renal calculi, hematuria, and burning in urination due to acidic urine.11
Varunadi Kshaya12 is capable of lithotriptic action, reducing pain intensity, dysuria and is also capable of reducing haematuria. Many articles from the GBD study reflect on evidence of renal problems.13-16 Several articles on different aspects of renal diseases were reported.17-20 Jain et. al. reported a rare case of Kikuchi’s Disease.21 Few of the related articles were reported by Somani et. al.22, Aryal et. al.23, Aradhey et. al.24, Balwani et. al.25
The result revealed that with ayurvedic Shaman Chikitsa renal calculi can be healed and thus lithotripsy and other surgical procedures can be prevented. As a serious and difficult clinical problem, kidney stones are present. Medical treatment can help avoid recurrence and the expulsion of small (<10 mm) stones when used judiciously in combination with dietary steps. It’s great that Non-Obstructive renal calculus of size 4.9mm in upper pole calyx got reduced to 3.4mm and obstructive calculus of size 7.4mm at RVUJ (Right Vesicoureteric Junction) expelled out within 30 days of with this Ayurvedic Shaman Chikitsa. As it was causing back pressure effect on the right kidney and thus causing umbilical Hernia. So the patient also got relief from Umbilical Hernia. The patient is continued with the same treatment for the next 30 days. Till date, there is no need for patient to undergo any surgical intervention as well as no recurrence of symptoms. This study is the management of a single case study only. An attempt must be made for additional investigation of the effect of this Shaman therapy in a large population for establishing standard treatment protocol.
CONCLUSION
The Chandraprabha Vati, Ayurvedic Formulation Tablet, Varunadi Kshaya can be safely and effectively carried out in patients of Mutrashmari with good results.
SOURCE OF FUNDING: Nil
CONFLICT OF INTEREST: There are no conflicts of interest
References:
-
Alessandro S, Ferraro PM, Cianchi C, Barsotti M, Gambaro G, Cupisti A. Which Diet for Calcium Stone Patients: A Real-World Approach to Preventive Care, Nutrients 2019; 11(5):1182.
-
Finlayson B. Physicochemical aspects of urolithiasis. Kidney Int 1978;13:344–360.
-
Evan A. Physiopathology and aetiology of stone formation in the kidney and the urinary tract. Pediatr Nephrol 2010;25:831–841.
-
Khan SR. Nephrocalcinosis in animal models with and without stones. Urol Res 2010;38:429–438.
-
Shastri K. Charaka Samhita of Agnivesha with Vidyotini Hindi commentary, Chikisasthan 26/59-60. (reprint edition), Chaukhambha Sanskrit Sansthan, Varanasi, 2006.
-
Shastri K. Sushrut Samhita with AyurvedtatvaSandipika Hindi commentary, Nidaansthan 3/7. (12th ed), Choukhambha Sanskrit Sansthan, Varanasi 2001.
-
Williams N Bulstrode. Bailly & Love’s short practice ofSurgery. Chapter 71. (25th ed), Hodder Arnold Publishers, London 2010.
-
Townsend C. SabistonTextbookofSurgery. In editor. Sabiston Textbook of Surgery. Elsevier publications, New Delhi, 2010.
-
Shastri K. Sushrut Samhita with Ayurvedtatva Sandipika Hindi commentary, Nidaansthan¾. (Reprint edition), Choukhambha Sanskrit Sansthan, Varanasi 2001.
-
Borghi L, Meschi T, Amato F, Briganti A, Novarini A, Giannini A. Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: A 5-year randomized prospective study. J Urol 1996;155:839–843.
-
Mishra S. Madhya khanda, chikitsasthana. Verse 70. In: Bhavprakash Samhita. Varanasi, India: ChaukhambaSurbharatiPrakashan; 2012: 383.
-
Sheetprabha tablets: benefits, dosage, side?effects, ingredients. Sheetaprabha Tablet - Benefits, Dosage, Side Effects, Ingredients (ayurmedinfo.com)
-
James A, Spencer L. Global Injury Morbidity and Mortality from 1990 to 2017: Results from the Global Burden of Disease Study 2017. Injury Prev 2020;26(1):i96–114.
-
Christopher J. Five Insights from the Global Burden of Disease Study 2019. Lancet 2020; 396(10258):1135–1159.
-
Christopher J. Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020;396:1223–1249.
-
Vos T. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020;396:1204–1222.
-
Balwani M. Attitude of the Chronic Kidney Disease Patients Toward Xenotransplantation of Organs. Transplantation 2018;102(7):S740.
-
Balwani M. Awareness about Kidney and Its Related Function/Dysfunction in School Going Children: A Survey from Central India. Saudi J Kidney Dis Transpl 2019;30(1):202–207.
-
Balwani M. Minimal Change Disease and Kimura’s Disease Responding to Tacrolimus Therapy. Saudi J Kidney Dis Transpl 2019;30(1):254–257.
-
Goswami J. Scoring Systems and Outcome of Chronic Kidney Disease Patients Admitted In Intensive Care Units. Saudi J Kidney Dis Transpl 2018; 29(2): 310–317.
-
Jain J. Kikuchi’s Disease (Histiocytic Necrotizing Lymphadenitis): A Rare Presentation with Acute Kidney Injury, Peripheral Neuropathy, and Aseptic Meningitis with Cutaneous Involvement. Ind J Path Microb 2018; 61(1):113–115.
-
Somani A. Traumatic Rhabdomyolysis Presenting as Acute Kidney Injury and Acute Respiratory Distress Syndrome in Young Male Athlete. Med Sci 2020;24(102):771–775.
-
Aryal N. Sudden Cardiac Death and Kidney Health Related Problems among Nepali Migrant Workers in Malaysia. Nepal J Epid 2019; 9(3):788–791.
-
Aradhey P. Clinical Profile of Uremic Polyneuropathy in Chronic Kidney Disease Patients. Med Sci 2020;24(102):945–951.
-
Balwani, M. Hepatitis C Virus, Directly Acting Antivirals and Guillain-Barre Syndrome. Saudi J Kidney Dis Transpl 2018;29(5):1237–1239.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





