IJCRR - 13(4), February, 2021
Pages: 08-12
Date of Publication: 16-Feb-2021
Print Article
Download XML Download PDF
The Impact of Laparoscopic Versus Open Ovarian Cystectomy on Ovarian reserve
Author: Ahmed L Aboul Nasr, Ahmed Soliman Nasr, Amr H Wahba, Reham Zeyada, Nadia M Helmy
Category: Healthcare
Abstract:Introduction: Ovarian cysts are a frequent finding in reproductive-aged women. Compared to laparotomy, laparoscopic cystectomy is increasingly gaining acceptance for ovarian cystectomy1 , but there is still no consensus on which approach is better regarding ovarian reserve2 . Objective: To determine and compare the impact of the approach of ovarian cystectomy whether laparoscopic or open on ovarian reserve parameters. Methodology: This prospective randomized study was conducted on 40 patients of reproductive age (range, 18\?35 years) with benign ovarian cysts who underwent either laparoscopic ovarian cystectomy (n=20) or open ovarian cystectomy(n=20). Serum anti-M\?llerian hormone (AMH), antral follicle count (AFC), and follicular stimulating hormone (FSH)were measured preoperatively and 3 months postoperatively in all patients. Results: Serum AMH decreased significantly at 3 months postoperatively in both laparoscopic and open ovarian cystectomy groups. The AFC increased significantly at 3 months postoperatively in both laparoscopic and open ovarian cystectomy groups. On the other hand, no significant difference in FSH was found between the preoperative and 3 months postoperative levels in both groups. Conclusion: No significant difference was found between both approaches of ovarian cystectomy whether laparoscopic or open regarding the change in ovarian reserve parameters postoperatively.
Keywords: Anti-Müllerian hormone, Antral follicular count, Laparoscopy, Ovarian cystectomy, Ovarian cysts, Ovarian reserve
Full Text:
Introduction
Benign ovarian cysts such as endometriomas, mature cystic teratomas, serous or mucinous cystadenomas are a common finding in young women in their reproductive age. It is assumed that about 7% of women worldwide experience asymptomatic cyst during their lifetime.1 Functional or simple ovarian cysts measuring less than 5 cm maximum diameter mostly resolve over 2–3 menstrual cycles without the need for intervention.2 Minimally invasive techniques of ovarian cystectomy whether laparoscopic such as fenestration and drainage of the cyst and stripping of the cyst wall, or mini-laparotomy have become increasingly common approaches for the surgical removal of benign ovarian cysts. However, the safety of these techniques in terms of ovarian damage to the operated ovary has been questioned.3
Ovarian reserve refers to the functional potential of the ovary, which is determined by the number and quality of the remaining primordial follicles at any given time. A great variety of tests and markers for ovarian reserve are available, none of which has yet been shown to be ideal.4 A large body of evidence has demonstrated greater clinical value of AMH and AFC compared to FSH. They have been used as the best predictors for ovarian response before proceeding with ovarian stimulation in assisted reproductive technologies (ARTs).5
The anti-Mullerian hormone is produced by the granulosa cells of primary, preantral and small antral follicles. AMH level represents a reliable and useful marker of ovarian reserves supported by its gradual decline with increasing age preceding changes in AFC, FSH, or estradiol. It is also menstrual cycle-independent unlike FSH and is unaffected by the use of oral contraceptive pills or gonadotropin-releasing hormone agonists.6 Compared to laparotomy, laparoscopic cystectomy is increasingly gaining acceptance for ovarian cystectomy6, but there is still no consensus on which approach is better regarding ovarian reserve.7
This study aimed to determine and compare the impact of the approach of ovarian cystectomy whether laparoscopic or open on ovarian reserve parameters including anti-mullerian hormone, antral follicular count and follicular stimulating hormone.
MATERIALS AND METHODS
This prospective randomized study was conducted at the Department of Obstetrics and Gynecology, Kasr El-Ainy Hospital, Cairo University, in the period from April 2016 to August 2018. Forty patients with benign ovarian cysts were recruited from the gynaecology clinic. Informed written consent was taken from each participant before enrollment in the study. Women aged from 20-35 years with benign ovarian cysts, were randomized into 2 groups; group A in which patients underwent laparoscopic cystectomy(n=20)and group B(n=20) in which patients underwent open cystectomy through laparotomy. Randomization was done using computer-generated random numbers and sealed envelopes.
Inclusion criteria included unilateral ovarian cyst(≥5 cm), with no clinical signs or ultrasound evidence suspicious of ovarian malignancy. Patients included had regular menstrual cycles (cycle length between 21 and 35 days). Patients on hormonal therapy or using oral contraception in the past 3 cycles, with endocrine diseases e.g. thyroid disease or hyperprolactinemia, with history of previous ovarian surgery or evidence of premature ovarian failure or premature menopause were excluded.
For all patients, full history was taken followed by complete physical examination & laboratory investigations in form of (AMH, FSH& routine preoperative investigations). Each patient underwent transvaginal ultrasonography using the 7.5 MHz vaginal probes of the X6 ultrasound machine (Medison X6, Korea) preoperatively on day 2 of the menstrual cycle to determine the size of the ovarian cyst, its location; and the AFC, which was defined as the total number of 2 to 10 mm antral follicles in the affected ovary.
Serum FSH was assayed on day 2 of the menses on IMMULITE 2000 Automated Immunoassay Analyzer. Serum AMH was assayed using AMH Gen II enzyme-linked immunosorbent assay(ELISA) kits purchased from Beckman Coulter, Inc., the USA with expected values: 0.9–9.5 ng/ml. The ovarian reserve was reassessed (AMH, FSH and day 2 AFC) 3 months following the cystectomy. The initial pre-operative and post-operative ultrasounds were done by a single investigator.
Twenty patients underwent laparoscopic ovarian cystectomy by use of a stripping technique. It was performed by the incision of the ovarian cyst using cold scissors, identification of the cystic wall, and then stripping off the cyst wall from the surrounding healthy ovarian tissue was achieved using traction and counter traction with two atraumatic grasping forceps. After excision of the cyst wall, selective coagulation was done using bipolar diathermy for hemostasis and the residual ovarian tissue was not sutured. Ovarian cystectomy by laparotomy through Pfannenstiel incision was performed on 20 patients. Cleavage plane was developed by using microsurgical techniques and instruments. After excision of the cyst wall, meticulous reconstruction and hemostasis of the ovarian tissue were achieved by the use of 2–0 polyglactin sutures (Vicryl; Ethicon Endo-Surgery, Cincinnati, OH, USA). All specimens obtained were sent for histopathological examination.
Statistical analysis
Data were coded and entered using the statistical package SPSS version 25. Data were summarized using mean and standard deviation for normally distributed quantitative variables or median and interquartile range for non-normally distributed quantitative variables and frequencies (number of cases) and relative frequencies (percentages) for categorical variables. Comparisons between groups were done using one-way ANOVA or unpaired t-test in normally distributed quantitative variables while Kruskal-Wallis and Mann-Whitney tests were used for non-normally distributed quantitative variables. Comparison between before and after in each group was done using paired t-test. For comparing categorical data, Chi-square (c2) test was performed. Exact test was used instead when the expected frequency is less than 5. P-values ?0.05 were considered as statistically significant.
Results
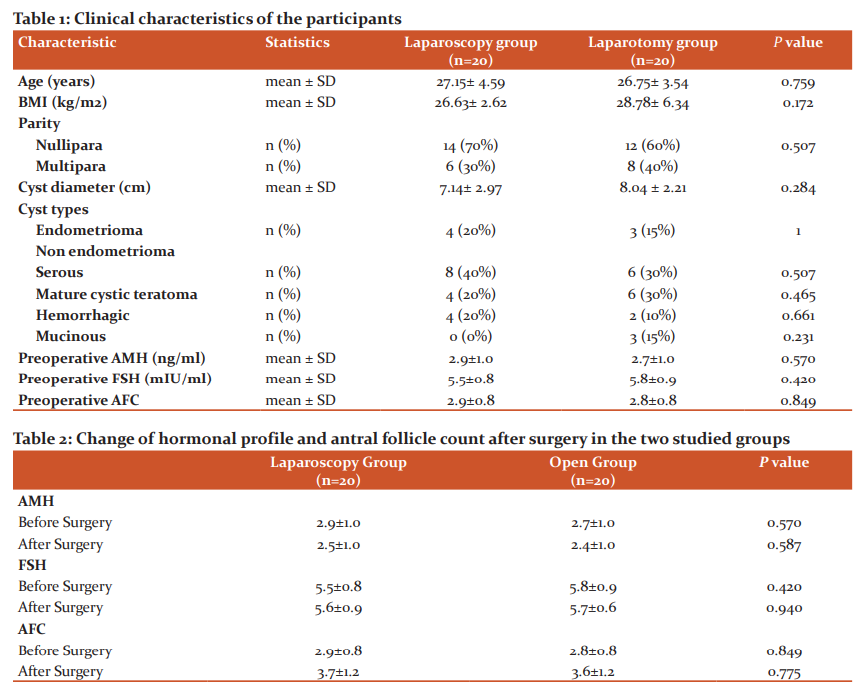
Of the 40 patients included in the study, 20 women were allocated to undergo laparoscopic ovarian cystectomy and 20 women were allocated to undergo open laparotomy. Both groups were comparable in age, BMI, parity and cyst size. The cysts were classified as simple serous cysts, mature cystic teratomas, endometriomas, hemorrhagic, and mucinous with each cyst type occurring at the comparable frequency in the 2 groups. Preoperative serum FSH, AMH and AFC were normal and comparable in both groups (Table 1).
Both the laparoscopic and open ovarian cystectomy groups showed a significant drop of AMH (p<0.001), with no significant difference between the two groups (p = 0.587). There was no significant change of FSH in the two groups (p = 0.940).AFC in the affected ovary increased significantly in the two groups, with no significant difference between the two groups (p = 0.775)(Table 2).
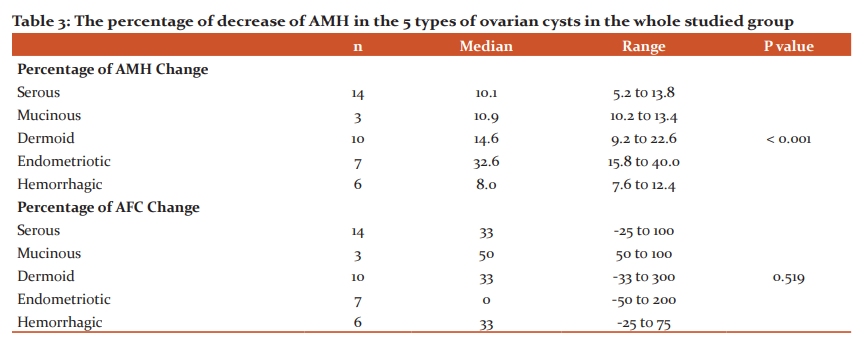
The percentage of decrease of AMH was significantly higher in patients with endometriomas compared to serous and hemorrhagic cysts (p<0.001). On the other hand, the percentage of increase of AFC was comparable in the different types of cysts (p = 0.519) (Table 3).
Discussion
Several surgical modalities can be performed to manage benign ovarian cysts; the appropriate route for the surgical management of ovarian masses whether laparoscopic or open, depends on several factors related to the woman, the mass and the setting.2 Although cystectomy offers an ovarian-sparing procedure, there has been growing evidence suggesting a decline in ovarian reserve as a result of ovarian cystectomy with the possible compromise to fertility potential.8 In the current study, our main concern was to compare the effect of laparoscopic and open ovarian cystectomy on the ovarian reserve which was tested by serum AMH, FSH and AFC.
Regarding the impact of ovarian cystectomy on ovarian reserve, our study showed that regardless of the approach used in ovarian cystectomy whether it’s open or laparoscopic, the AMH showed a statistically significant decrease, while the AFC of the operated ovary showed a statistically significant increase and the FSH showed no change postoperatively, with no significant difference between both groups, as shown in Table 2.
As regards the decline in serum AMH, Kostrzewa et al.9 revealed a significant decrease in serum AMH concentration 3 months after laparoscopic cystectomy (P<0.001) in concordance to our study. Moreover, a meta-analysis done in 201610 to investigate the impact of excision of benign non-endometriotic ovarian cysts on ovarian reserve showed a marked decline (38%) in circulating AMH after ovarian cystectomy. Owczarek and his co-workers11alsoreported a statistically significant reduction of AMH 3 months after laparoscopic cyst enucleation of endometriomas, teratomas and simple cysts regardless of the applied haemostasis technique.
Several mechanisms underlying the post-operative reduction of the ovarian reserve have been proposed. First, the damage may precede surgery, i.e. the cyst itself may cause negative effects on the surrounding tissue. Secondly, it has been proposed that a consistent amount of ovarian tissue containing follicles is unintentionally removed during cystectomy, which leads to a decrease in ovarian reserve. The removal of any benign cyst inadvertently leads to the removal of ovarian tissue, but the effect is more significant in endometriomas3,6. Another possible reason for the post-surgical reduction of ovarian reserve is the damage inflicted on the vascularization due to surgery-related local inflammation and electrosurgical coagulation.10 The vascular system of the ovary might also be injured during adhesiolysis, thus possibly resulting in poor blood supply to the post-surgical ovary.1
As regards the change in the AFC, several studies showed a postoperative increase of AFC similar to our results.11-14 The increase in AFC postoperatively in our study could be explained by the underestimation of the AFC preoperatively which would be technically difficult due to the compression of the benign ovarian cysts, and the calculated AFC might be lower than the actual number in the preoperative period.13 Another hypothesis is that the loss of pressure to the cortex after excision of endometrioma leads to the resolution of inflammation and the progressive recovery and rearrangement of the follicle cohort, especially when pericystic healthy ovarian tissue removal is minimal.15
There was no significant change in serum FSH in the two groups. In concordance with our results, several studies have revealed that there was no significant change in the FSH value after ovarian cystectomy in comparison with preoperative levels after ovarian cystectomy.3,13 We agree with their opinion that basal FSH has low sensitivity in detecting the early decrease in the ovarian reserve. Similar to our results several studies revealed that there were no statistically significant differences at any time point between the laparotomy and laparoscopy groups regarding the decrease in AMH postoperatively.16,17 Unlike our study, Zaitoun et al. 2showed that a statistically significant decrease of the mean AMH value and basal AFC, and a statistically significant increase of serum FSH occurred in laparoscopic group compared to open laparotomy group. However, their study was conducted on endometriomas only and they repeated the serum AMH, FSH and AFC at 6, 12 and 18-month postoperatively.
In our study patients with ovarian endometriomas showed a more significant decrease in AMH after cystectomy compared to serous and hemorrhagic cysts (P< 0.001), compared to serous cysts (P< 0.001), as shown in Table 3. In concordance with our results, Kostrzewa et al.9 showed that the AMH decline was considerably higher after cystectomy of the endometrioma (45.4%) in comparison to other benign ovarian cysts (14.9%). Chun and his co-workers found that the AMH decline after cystectomy was much greater in the endometrioma and teratoma groups compared with the other benign cyst group.18 Also, Henes et al.1 revealed that endometriotic cysts and follicular cysts showed a significant drop in the AMH levels; whereas other types of cysts showed no significant reduction in AMH postoperatively.
The greater damage to the ovarian reserve caused by cystectomy of endometriomas compared with other benign ovarian cysts might be attributed to the intrinsic characteristics of endometriomas themselves, suggesting lack of a histologic plane between the endometriotic cyst wall and the ovary unlike the boundary in other benign ovarian cysts leading to destruction and removal of healthy ovarian stroma.19 Mircea et al.20 detected ovarian parenchyma in 40% of the specimens of patients with endometriomas who underwent cystectomy. Urman et al.21 also found primordial follicles embedded in the cortical tissue adjacent to the cyst capsule in 61.5% of endometrioma cystectomy specimens.
Conclusion
Ovarian cystectomy for benign ovarian cysts was found to affect ovarian reserve parameters causing a decline in serum AMHand increase in AFC-possibly apparent- postoperatively, with no change of FSH. No significant change was found between laparoscopic and open ovarian cystectomy regarding the change in ovarian reserve parameters.
Acknowledgements
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references to this manuscript. The authors are also grateful to authors, editors, publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflict of interest
The authors have no conflicts of interest.
Source of funding
Personal fund.
Ethical Clearance
Ethically approved by the department.
References:
-
Henes M, Engler T, Taran FA, Brucker S, Rall K, Janz B, et al. Ovarian cyst removal influences ovarian reserve dependent on histology, size and type of operation. Women's Health (Lond). 2018;14:1745506518778992.
-
Royal College of Obstetricians and Gynecologists. Management of Suspected Ovarian Masses in Premenopausal Women. Green-top Guideline No. 62. London: RCOG; 2011.
-
Jang WK, Lim SY, Park JC, Lee KR, Lee A, Rhee JH. Surgical impact on serum anti-Müllerian hormone in women with benign ovarian cyst: A prospective study. Obstet Gynecol Sci 2014 Mar;57(2):121-127.
-
Ding Y, Yuan Y, Ding J, Chen Y, Zhang X, Hua K. Comprehensive Assessment of the Impact of Laparoscopic Ovarian Cystectomy on Ovarian Reserve. J Min Invas Gynecol 2015;22(7):1252-1259.
-
Fleming R, Seifer DB, Frattarelli JL, Ruman J. Assessing ovarian response: antral follicle count versus anti-Mullerian hormone. Reprod Biomed Online 2015 Oct;31(4):486-96.
-
Alammari R, Lightfoot M, Hur HC. Impact of Cystectomy on Ovarian Reserve: Review of the Literature. J Min Invas Gynecol 2017 Feb;24(2):247-257.
-
Zaitoun MM, Zaitoun MM, El Behery MM. Comparing long term impact on the ovarian reserve between laparoscopic ovarian cystectomy and open laparotomy for ovarian endometrioma. J Ovarian Res 2013 Nov;6(1):76.
-
Pergialiotis V, Prodromidou A, Frountzas M, Bitos K, Perrea D, Doumouchtsis SK. The effect of bipolar electrocoagulation during ovarian cystectomy on ovarian reserve: a systematic review. Am J Obstet Gynecol 2015 Nov;213(5):620-628.
-
Kostrzewa M, Wilczy?ski JR, G?owacka E, ?y?a M, Szy??o K, Stachowiak G. One-year follow-up of ovarian reserve by three methods in women after laparoscopic cystectomy for endometrioma and benign ovarian cysts. Int J Gynaecol Obstet 2019 Sep;146(3):350-356.
-
Mohamed AA, Al-Hussaini TK, Fathalla MM, El Shamy TT, Abdelaal II, Amer SA. The impact of excision of benign nonendometriotic ovarian cysts on ovarian reserve: a systematic review. Am J Obstet Gynecol 2016 Aug;215(2):169-176.
-
Owczarek D, Malinowski A, Wilczy?ski M. Ovarian reserve evaluation after laparoscopic cyst enucleation, depending on applied haemostasis technique and with particular consideration of endometrial cysts. Prz Menopauzalny 2018 Mar;17(1): 22–27.
-
Georgievska J, Sapunov S, Cekovska S, Vasilevska K. Effect of Two Laparoscopic Techniques for Treatment of Ovarian Endometrioma on Ovarian Reserve. Med Arch 2015 Apr; 69(2): 88–90.
-
Saliho?lu KN, Dilbaz B, C?r?k DA, Ozelci R, Ozkaya E, Mollamahmuto?lu L. Short-Term Impact of Laparoscopic Cystectomy on Ovarian Reserve Tests in Bilateral and Unilateral Endometriotic and Nonendometriotic Cysts. J Min Invas Gynecol 2016;23(5):719-725.
-
Candiani M, Ottolina J, Posadzka E, Ferrari S, Castellano LM, Tandoi I, et al. Assessment of ovarian reserve after cystectomy versus 'one-step' laser vaporization in the treatment of ovarian endometrioma: a small randomized clinical trial. Hum Reprod 2018;33(12):2205-2211.
-
Kitajima M, Dolmans MM, Donnez O, Masuzaki H, Soares M, Donnez J. Enhanced follicular recruitment and atresia in cortex derived from ovaries with endometriomas. Fertil Steril 2014 Apr;101(4):1031–1037.
-
Sugita A, Iwase A, Goto M, Nakahara T, Nakamura T, Kondo M, et al. One-year follow-up of serum antimullerian hormone levels in patients with cystectomy: are different sequential changes due to different mechanisms causing damage to the ovarian reserve. Fertil Steril 2013 Aug;100(2):516–22.
-
Abdel–Maksoud MD, Samy N, Hashim M, Elkhayal A, Fathy H, Gomaa I. Assessment of Ovarian Reserve After Ovarian Cystectomy by Laparotomy Versus Laparoscopy. Int J Pharm Clin Res 2015; 7(1): 23-28.
-
Chun S, Cho HJ, Ji YI. Comparison of the early postoperative decline of serum antiMullerian hormone levels after unilateral laparoscopic ovarian cystectomy between patients categorized according to histologic diagnosis. Taiwan J Obstet Gynecol 2016 Oct;55(5):641–645.
-
Shaltout MF, Elsheikhah A, Maged AM, Elsherbini MM, Zaki SS, Dahab S, et al. A randomized controlled trial of a new technique for laparoscopic management of ovarian endometriosis preventing recurrence and keeping ovarian reserve. J Ovarian Res 2019;12(1):66.
-
Mircea O, Puscasiu L, Resch B, Lucas J, Collinet P, von Theobald P, et al. Fertility Outcomes After Ablation Using Plasma Energy Versus Cystectomy in Infertile Women with Ovarian Endometrioma: A Multicentric Comparative Study. J Min Invas Gynecol 2016;23(7):1138-1145.
-
Urman B, Alper E, Yakin K, Oktem O, Aksoy S, Alatas C, et al. Removal of unilateral endometriomas is associated with an immediate and sustained reduction in ovarian reserve. Reprod Biomed Online 2013 Aug;27(2):212-6.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





