IJCRR - 12(20), October, 2020
Pages: 95-97
Date of Publication: 27-Oct-2020
Print Article
Download XML Download PDF
Ultrasonography Guided Fine Needle Aspiration Cytology as a Valuable Tool for Management of Solitary Thyroid Nodule
Author: Meenakshi Kekre, Anant Kekre
Category: Healthcare
Abstract:Background: Ultrasonography (USG) in today's scenario is extremely crucial for detection of the dimensions of the tumour, for the diagnosis of multinodular goitres, and more importantly the nature of the solitary thyroid nodule whether it is solid or cystic. Very rarely cystic nodule is associated with malignancy. Aims & Objectives: Our study on solitary thyroid nodules will try to corroborate the pre-operative cytological diagnosis obtained by USG guided Fine Needle Aspiration Cytology with the postoperative histopathological diagnosis. Methods: We have studied 60 patients taken from a tertiary care hospital for one year. We have considered to only the patients with solitary thyroid nodule of both sexes and all age groups. The type of operation was planned as per the report of USG guided fine needle aspiration cytology (FNAC). Results: Patients were aged between 15-75 years. 83 % of the patients in our study were females. Commonly associated symptoms were of hoarseness of voice, lymph node involvement & those nodes are fixed to the underlying structures & all these symptoms strongly suggestive of malignancy. Conclusion: When properly done by an expert cytopathologist, we can reliably diagnose the benign cases, that can be managed reasonably by conservative approach rather than subjecting all patients to operations.
Keywords: Multinodular goitre, Solitary thyroid nodule, USG, FNAC
Full Text:
INTRODUCTION
A solitary thyroid nodule is the commonest presentation of thyroid carcinoma & studies suggest that only 10% of them are cancerous. After doing proper examination & investigation, most of them looking solitary thyroid nodules will be as a part of a multinodular goiter1-2. On radiological investigation, if the nodule turns out to be truly solitary then the chances of it being malignant rises by 20%. Hence it is extremely crucial to find out these cases so that we can plan safe & effective surgical intervention. Rest of the patients can be managed by a conservative approach along with judicious follow-up so that unnecessary operations can be avoided. In the general population, the chances of having solitary thyroid nodule may be up to 3%. It may be a simple adenoma or carcinoma3-5.
Whereas if adenoma is there then simple excision will solve the purpose but if it turns out to be a carcinoma then surgical intervention differs as per the type of carcinoma. USG is very convenient and extremely proficient for the detection of the dimensions of the tumour, for the diagnosis of multinodular goitres, and more importantly the nature of the solitary thyroid nodule whether it is solid or cystic. Very rarely cystic nodule is associated with a malignancy6-7. Its accuracy of detection by USG is directly proportional to its resolution.
Similarly, if FNAC is carried out under the guidance of USG then the specificity and sensitivity of the procedure increase. Most importantly. This procedure is free from radiation exposure8-9.
Aims and objectives: Our study on solitary thyroid nodules will try to corroborate the pre-operative cytological diagnosis obtained by USG guided FNAC with the postoperative histopathological diagnosis.
MATERIAL AND METHODS
Study type: Observational study.
Study Period: one year
Place of study: tertiary care hospital
Sample size: We have studied 60 patients. We have considered only the patients with solitary thyroid nodule of both sexes and all age groups ( Table 1).
Study design: The modules which were small, difficult to palpate and deeply seated were particularly chosen. The cases of multinodular goitres were excluded from our study. The detailed history of the patient’s illness, any history of radiation exposure, the familial background particularly in respect of thyroid carcinoma was taken which was followed by thorough clinical examination & local examination. We clinically assessed the functional status of the thyroid. Routine blood tests, chest X-Ray, urine and stool examination, ECG was done to assess the general condition of the patient. Then we proceed to the specific investigation of the disease proper. We checked the functional status of the thyroid gland by examining blood for T3, T4 and TSH. We consider the patients with a normally functioning thyroid status for our study. We then performed USG guided FNAC in all patients to detect the size of the lesion and more importantly the consistency of the nodule. The material obtained by USG guided FNAC was subjected to cytological examination to diagnose the nature of the lesion. We have done Radionuclide uptake and thyroid scan in selective patients.
After a thorough evaluation, we did operative intervention under general anaesthesia whenever required, after taking consent and following the norms of medical ethics. The type of operation was according to the report of USG guided FNAC. The post-operative specimen was sent for histopathological examination. The results were compared with the pre-operative USG guided FNAC report.
RESULTS
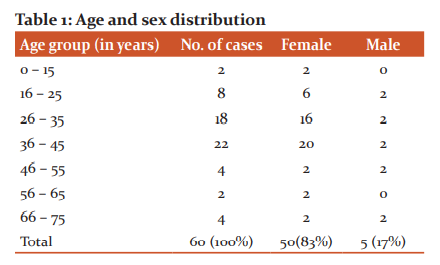
As per table no. 1, Most of our study subjects were middle-aged females.
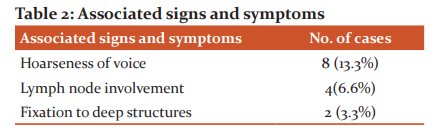
As per table no. 2, all the three associated symptoms of Hoarseness of voice, Lymph node involvement & Fixation to deep structures are in favour of malignancy.
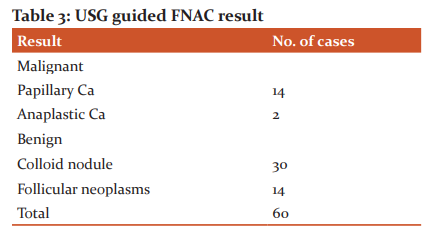
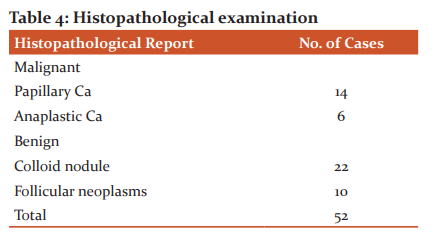
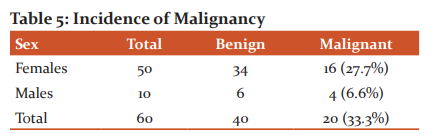
As per table no. 3, on USG guided FNAC, 16 cases were diagnosed as the clear malignant lesion, out of this 14 were papillary Ca and 2 were anaplastic Carcinoma. As per table no. 4, 30 cases out of 60 were diagnosed as a colloid nodule.
As per table no. 5, eight cases were managed conservatively.
DISCUSSION
In our study, the age of the patients was between 15-75 years. According to Russel, the majority of patients with solitary thyroid nodules present in between 30-55 years and 80% are females. Watkinson noted that a solitary thyroid nodule is more likely to be malignant if the patient is male. We also noted that male patients are more prone to develop a malignant thyroid nodule10. Apart from swelling in the neck, there were symptoms such as hoarseness of voice, fixity to the deeper structures and lymph node enlargement. All the above symptoms correlate with malignancy. We have selected the cases with small thyroid nodules. Out of 60 patients in our study, 58 patients (96.6%) were clinically and biochemically euthyroid11-12. Only 2 patients were seen to have hypothyroidism on biochemical examination though they both were clinically euthyroid. We did not encounter any case of hyperthyroidism. As almost all patients of solitary thyroid nodule are euthyroid, it is not necessary to do all thyroid function tests (T3, T4 and TSH) in every patient. One parameter is enough and according to Russel, that parameter is T4. The FNAC is a very simple, rapid procedure that can be done on OPD basis and is devoid of any complication and radiation exposure. It does not require any anaesthesia and hospitalization. The procedure is economical and inflicts minimal trauma. When this procedure is done under the guidance of USG the sensitivity and specificity are increased and the chance of complications is also minimized. For better results, the aspiration should be done by the person who will interpret the result. To get adequate samples, multiple punctures at different sites should be done. The cytopathologist should have a view of all relevant clinical and radiological data. Proton magnetic resonance spectroscopy may be used on FNAC smears to help to differentiate benign from malignant follicular neoplasms13-15. In this technique, the spectral ratio of resonance from amino acid lysine and lipid is used to differentiate normal follicular cell from cancerous follicular cells in FNAC smears. In our study, we have operated 52 cases out of 60 patients and all the specimens were sent for histopathology. 8 cases of a small solitary thyroid nodule, reported as colloid goitre in USG guided FNAC, were not subjected to operation and they have been managed conservatively with regular follow up. We have operated those patients which were benign on cytology but have a strong suspicion of malignancy clinically. We also emphasized regular follow up with repeat USG guided FNAC whenever required16.
CONCLUSION
All patients were clinically euthyroid. Among the associated symptoms there were hoarseness of voice, lymph node involvement and fixity to deeper structures go in favour of malignancy. All patients were subjected to USG guided FNAC. We found this technique very simple, safe, practically atraumatic. Due to low false-negative report of USG guided FNAC, it would be easy to plan the conservative management of solitary thyroid nodule. When compared with postoperative histopathology report, it can be concluded that USG guided FNAC can guide the course of management of “Solitary Thyroid Nodule”.
References:
-
Watkinson J et al. Tumors of the thyroid and parathyroid glands; Stell and Maran’s Head and Neck Surgery; 4th edition:; Butterworth Heinemann: 459-485.
-
Taksande A et al. Study of Motor Nerve Conduction Velocity in Patients of Thyroid Dysfunction in Central India.” Journal of Datta Meghe Institute of Medical Sciences University. 2017; 12(4): 229–33.
-
C F J Russel; Recent Adv in Surg; 17th edition; 1994; 4- 16.
-
Raniwala A, et al. Study and Correlation of Clinical, Radiological, Cytological, and Histopathological Findings in the Diagnosis of Thyroid Swellings. Journal of Datta Meghe Institute of Medical Sciences University 2017; 12(2): 138–42.
-
Abdullaeva M, et al. The Influence of Dysfunction of the Autonomic System and the Thyroid Gland on the Course of Bronchial Asthma (BA) in Children IJCRR. 2020, 12(14): 36-39
-
Robertson M, et al; Otolaryngol Head Neck Surg. 2004; 131: 596-600.
-
Agrawal D, et al. “Role of Bethesda System for Reporting Thyroid Lesion and Its Correlation with Histopathological Diagnosis.” Journal of Datta Meghe Institute of Medical Sciences University. 2019, 14(2): 74–81
-
Russell CF, Recent Adv. In Surg; 17th ed; 1994; 4-16.
-
Wagh S, et al. Relationship between Hypothyroidism and Body Mass Index in Women: A Cross-Sectional Study. IJCRR. 2020;12(12): 48-51.
-
Sutapa D, et al. Fine Needle Aspiration Cytology of Cervical Lymph Nodes with Special Emphasis on Different Cytomorphological Presentation of Tuberculous Infection. IJCRR. 2020;12(16), 108-114.
-
Matheson N, The diagnosis of thyroid swelling; in Russell RCG (ed) Recent Adv in Surg; 12th ed; Ch. Livingstone; Edinburgh; 179-197.
-
Zajicek J, Kargar S, Basel R. Aspiration Biopsy Cytology 1 & 2. 1974; 384-389.
-
Wong TH, et al; Ann Acad Med Singapur; 22(4); 1993.
-
Gulve S, et al. “Parathyroid Adenoma: Ultrasonography, Doppler, and Elastography Imaging.” Journal of Datta Meghe Institute of Medical Sciences University. 2019; 19(1): 47–49.
-
Gurbani N, et al. To Study the Histopathological Forms of Thyroid Lesions Observed in Tertiary Care Hospital International Journal of Current Research and Review. 2020 12(14): 109-112
-
Ramaciotti CE et al; Diagnostic accuracy and use of aspiration biopsy in the management of thyroid nodules; Arch. Intern Med. 144(6): 1169-1640.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





