IJCRR - 10(6), March, 2018
Pages: 43-48
Date of Publication: 28-Mar-2018
Print Article
Download XML Download PDF
Spectrum of Non-neoplastic Skin Lesions: A Histopathological Study based on Punch Biopsy
Author: Vivek Kumar, Hansa M. Goswami
Category: Healthcare
Abstract:Introduction: Accurate diagnosis of skin is of utmost importance for management of different skin disorders presenting with the similar clinical signs and symptoms. Therefore to confirm the diagnosis and start treatment biopsy becomes inevitable and for obtaining diagnostic full-thickness skin specimens Punch biopsy is the primary method.
Aims & Objective: The present study was to analyse the incidence and age & sex distribution of dermatological disorders presenting to B.J. Medical College, Civil Hospital Ahmedabad (tertiary care centre), Gujarat and access their histopathological profile
Materials & Methods: This was a retrospective study carried out at the department of Pathology B.J. Medical College & Civil Hospital, Ahmedabad for a period of 1 year (1st January 2016 to 31st December 2016). With necessary clinical details obtained in a proforma, punch biopsy specimen is sent to the histopathology section for final diagnosis. Formalin fixed, paraffin embedded sections were prepared & slides were routinely stained with H & E and special stains applied wherever necessary. Data obtained was tabulated and analysed
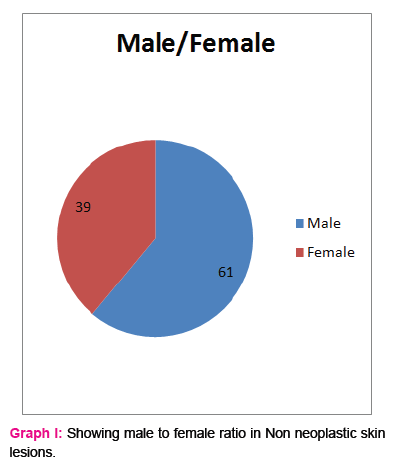
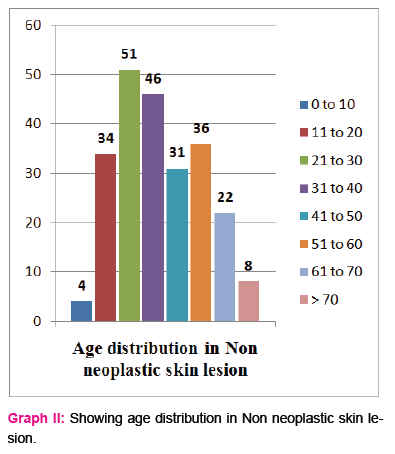
Results: Total 232 cases were analysed. 21-30 years age group constituted 22% of the total cases. Male/Female ratio is 61/39. Hypopigmented patch/plaque was the most common clinical lesion (27%). Hansen's disease was the most common histopathological diagnosis reported (30%) followed by vesiculobullous lesions (12%).
Conclusion: Punch biopsy is a very simple outdoor procedure and very useful for skin lesions. Hansen's disease is still most common skin disease for which biopsy is done followed by vesiculobullous lesion. Tattoo induced granuloma is also a common lesion along with lichenoid lesion.
Keywords: Accurate diagnosis, Punch biopsy, Non-neoplastic skin lesions
DOI: 10.7324/IJCRR.2018.1069
Full Text:
INTRODUCTION:
Several Studies conducted over a period of time have shown high prevalence of skin disorders in developing countries, the histopathological spectrum of which has been highly variable but the clinical presentation is restricted to only a few changes such as hyperpigmentation, hypopigmentation, macules, papules, nodules and a few others1. So the separation of each of these becomes important because the treatment and prognosis tends to be disease specific2. The punch biopsy is generally the most useful procedure as it is quick to perform convenient, and only produce a small wound. It create a full thickness sample of skin that allows the pathologist to get a good overview of epidermis, dermis and most of the time the subcutis also3. The aim of the present study was to classify the various skin disorders prevalent in the surrounding community and determine their demographic distribution.
AIMS & OBJECTIVES:
The present study was to analyse the incidence and age and sex distribution of dermatological disorders presenting to B.J. Medical College, Civil Hospital Ahmedabad (tertiary care centre), Gujarat and access their histopathological profile and also gives knowledge and understanding about usefulness of punch biopsy in skin lesion.
MATERIALS & METHODS:
This was a retrospective study carried out at the department of Pathology B.J. Medical College & Civil Hospital Ahmedabad for a period of 1year (1st January 2016 to 31st December 2016). Punch biopsy taken and necessary clinical details were obtained in a proforma, and sent to the histopathology section for final diagnosis. Formalin fixed, paraffin embedded sections were prepared & slides were routinely stained with H and E and special stains applied wherever necessary. Data obtained was tabulated and analysed.
Case selection and exclusion criteria:
Clinically diagnosed cases of non-neoplastic skin disorders were included.
Cases with tumorous histology were not included in our study.
Inadequate and autolysed skin biopsies were excluded from our study.
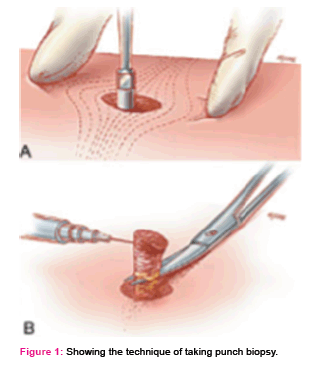
Punch biopsy technique4:
A. First we keep the punch biopsy instrument perpendicular to the surface of the lesion then we press it down into the lesion while it is rotated clockwise and anticlockwise, cutting down till the subcutaneous fat. After this the punch biopsy instrument is removed.
B. Then we gently lift the biopsy specimen with the help of needle to avoid crush artifact. At the level below the dermis we cut the specimen with help of a scissor. In case of small punch biopsy defects (2 to 3 mm) no need to suture it, but larger wounds (4 to 5 mm) must be closed to reduce healing time and scarring.
Punch biopsy can be kept from curling during fixation by placing them on a piece of file card prior to immersion. When the specimen is 0.3 mm or less in diameter, it is best processed into Paraffin in one piece. It may then be sampled at various levels in the block. It prevents loss of tissue during the facing up of the block and allows more adequate sampling.
Tissue processing5:
Paraffin embedding and block making, trimming, sectioning and staining.
Hematoxylin and Eosin Staining Procedure5:
- Sections were dewaxed in 2 jars of Xylene, each for 2 min.
- Slides were kept in 2 jars of absolute alcohol, each for 2 mins to remove xylene.
- Put the slides for 1 min. in 90% alcohol
- Put the slides for 1 min. in 70% alcohol
- Rinsed in water.
- Put the sections in Harris Hematoxylin for 7-10 min.
- Wash in running water and the sections turn blue.
- Then Sections were kept in 1% acid alcohol solution just for 5-10 sec.
- Washed with the tap water for 5-6 mins.
- Dipped in saturated solution of lithium carbonate till the section is completely blue.
- Washing with the tap water for 5-6 mins.
- Put the sections in 50% alcohol for 2 mins. Followed by 70% alcohol for 2 mins. And finally in 90% alcohol for 2 mins.
- Then sections were kept in 1% Eosin Y for 60 seconds.
- Rinsed for 2 min. in 95% alcohol 2 times each
- Dehydrated with absolute alcohol for 2 mins. for 3 times.
- 3 changes in Xylene each for 2 mins. is done for clearing.
- DPX. Mount.
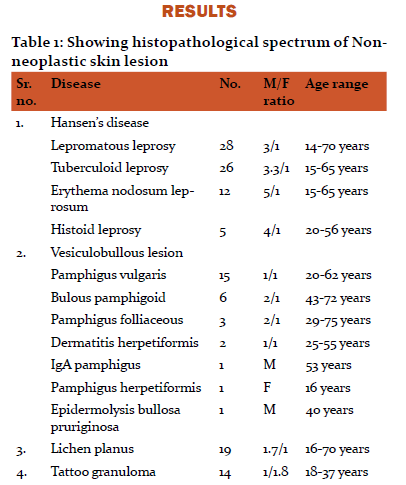
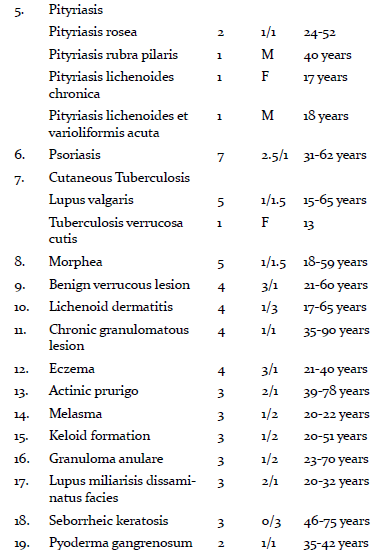
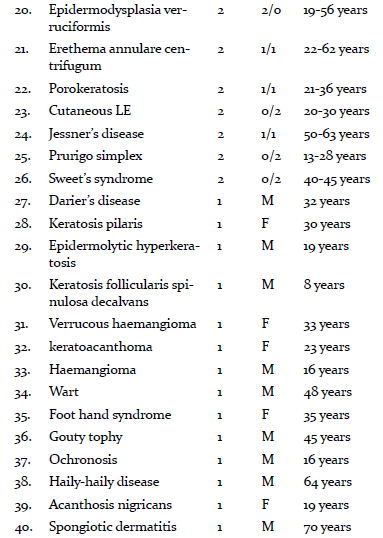
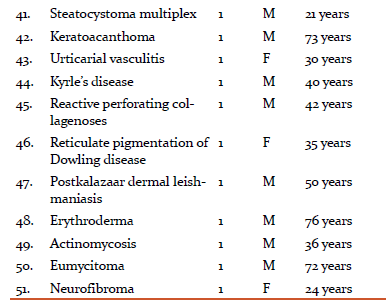
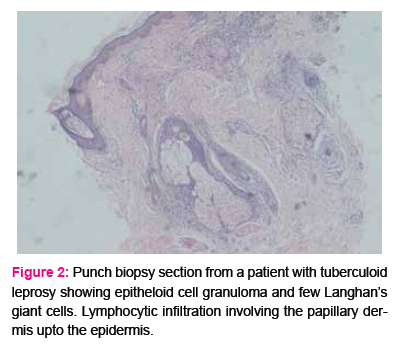
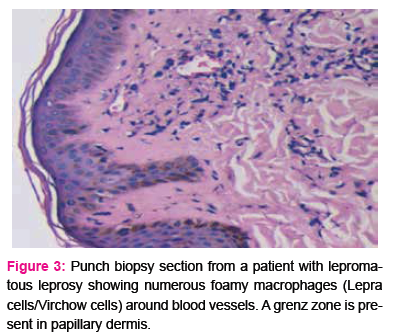
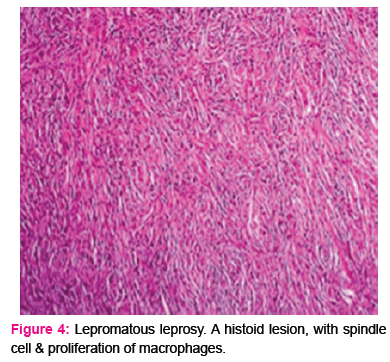
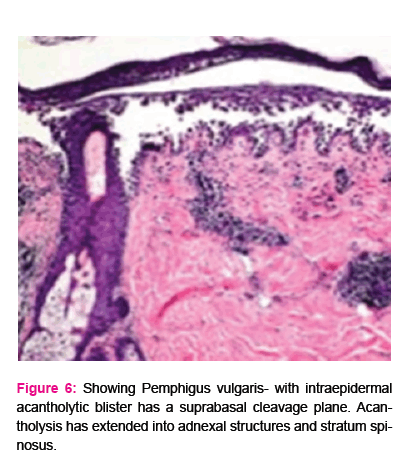
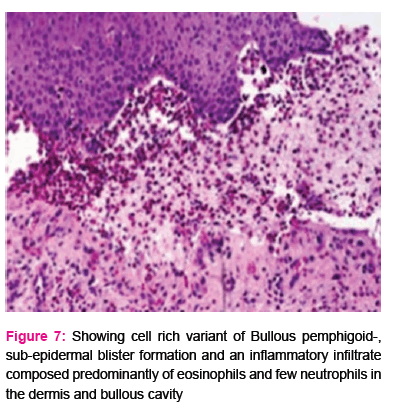
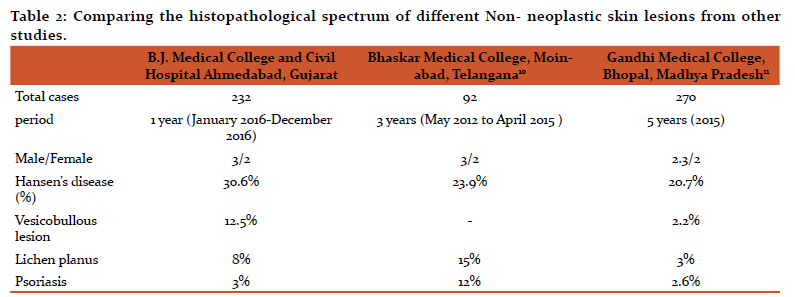
Histopathological examination results of punch biopsy show the wide range of diagnosis even though the clinical features are similar in different patients. Total 232 cases were taken for a period of 1 year (1st January 2016 to 31st December 2016). Results show the male predominance with male to female ratio is 3/2. Patient with younger age group (< 40 years) are 59% with 22% of patients are between 21-30 years age group. With 30.6% of patients most common diagnosis in our study is Hansen's disease followed by vesicobullous lesions with 12.5% of cases. Within vesicobullous lesion pemphigus vulgaris is most common. Lichen planus consist of 8% of cases and Psoriasis consist of 3% of cases. Tattoo granuloma is also a major problem with 6% of total case studied. 5 cases of Histoid leprosy was also seen which is a rare form of Lepromatous Leprosy.

DISCUSSION:
This was a retrospective study carried out at the department of Pathology B.J. Medical College and Civil Hospital Ahmedabad for a period of 1year (1st January 2016 to 31st December 2016). In our study total 232 cases are analysed. 80 patients were analysed in the study by Rajasekhar et al6. 112 cases were analysed in the study by Singh et al.7. In the present study, 22% of the patients were in the age group of 21 to 30 years and 19.8% of the patients were in the age group of 31-40 years. 25% of the patients were in the age group of 21 to 30 years in the study by Yonus et al8. 23.75% of the patients were in the age group of 31 to 40 years in the study by Rajasekhar et al.
With 30.6% of patients most common diagnosis in our study is Hansen's disease followed by vesicobullous lesions with 12.5% of cases. In the study by Bharambhe et al.9 lichenoid lesions were most common (46.57%) followed by psoriasis (19.88%). Most common histopathological diagnosis was Psoriasis (42.5%)followed by Lichen planus in the study by Rajasekhar et al
CONCLUSION:
Histopathological spectrum of skin lesions have been highly variable but the clinical presentation shows very few changes such as hyperpigmentation, hypopigmentation, macules, papules, nodules and a few others. Therefore for confirmation of diagnosis and initiation of treatment biopsy becomes inevitable in various skin disorders.
Punch biopsy is the basic technique for obtaining diagnostic full-thickness skin specimens and can be performed in OPD set up. It is very simple technique to learn and perform. Supervision is rarely needed after a physician has performed two or three procedures. when suture closure of the wound is performed only general surgical and suture-tying skills are required.
It is important to perform the skin biopsy at appropriate phase of the disease, from proper site, of proper thickness especially in cases of non infectious inflammatory dermatoses.
In diseases in which expected changes are quantitive rather than qualitative ( hyperkeratosis, acanthosis, increase in dermal thickness), the evaluation of these changes are best made by taking a punch biopsy also of clinically normal skin nearby, which represents the best possible control.
Hansen's disease is still most common skin disease for which biopsy is done followed by vesiculobullous lesion. Tattoo induced granuloma is also a common lesion along with lichenoid lesion.
ACKNOWLEDGEMENT:
I express my sense of deep gratitude towards my PG guide Dr. Hansa M Goswami Prof. and Head department of Pathology for her co-operation and help to prepare this paper for publication.
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
- Burns T, Breathnach S, Cox N, Griffiths C; Rook's Textbook of Dermatology. 2010.
- Lever's histopathology of skin; Devid E Elder, Bernett Johnson Jr., Rosalle Elenltsas; 9th Edition
- Rosai and Ackerman's Surgical pathology 10th edition
- Brown JS. Minor surgery: a text and atlas. 3d ed. New York: Chapman and Hall, 1997
- Bancroft JD, Stevens A; Theory and Practice of histological Techniques. 5th edition. Chruchill Livingstone, Edinburgh, 1990.
- Reddy R, Krishna N. Histopathological spectrum of non-infectious erythematous, papulo-squamous lesions. Asian Pac J Health Sci. 2014;1(4S):28–34.
- R. Singh, K. Bharathi, R. Bhat, C. Udaya Shankar. The Histopathological Profile Of Non-Neoplastic Dermatological Disorders With Special Reference To Granulomatous Lesions – Study At A Tertiary Care Centre In Pondicherry. Internet Scientific Publications/ Internet Journal of Pathology. Vol 13(3)
- Younas M, Haque A. Spectrum of histopathological features in non-infectious erythematous and papulosquamous diseases. Int J Pathol. 2004;2(1):24–30.
- D'Costa G, Bharambhe BM. Spectrum of NonInfectious Erythematous, Papular and Squamous lesions of the skin. Indian J Dermatol. 2010;55: 225-8.
- Veldurthy VS, Shanmugam C, Sudhir N, Sirisha O, Motupalli CP, Rao N, Reddy SR, Rao N. Pathological study of non-neoplastic skin lesions by punch biopsy. Int J Res Med Sci 2015:;3(8):1985-8.
- Neetu Goyal et al., Sch. J. App. Med. Sci., 2015; 3(1F):444-449
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





