IJCRR - 4(17), September, 2012
Pages: 181-187
Date of Publication: 14-Sep-2012
Print Article
Download XML Download PDF
VIBRATION THRESHOLD OF UPPER LIMB DURING ULNT1 IN INDIVIDUALS WITH TYPE II DIABETES MELLITUS AND NON DIABETIC INDIVIDUALS
Author: Mamta Mohan, Ravi Shankar Reddy, Ganesh BM
Category: Healthcare
Abstract:Background: Type II diabetes mellitus patients have been shown to affect the multimodal sensory, reflex and motor systems in distal extremities. Studies have examined the mechanosensitivity and vibration threshold in type II diabetes mellitus patients in the lower limb and compared it with normal individuals. There is scanty literature available in comparison of the vibration threshold in the upper limb in type II diabetes mellitus patients with non diabetic individuals. Methods: Thirty type II diabetic individuals were included in the diabetic group and thirty asymptomatic age matched individuals were taken to match the group. Vibration threshold (VT) was measured by tester 1 at the baseline for both the groups using a bioesthesiometer capable of deriving a vibration of 100 Hz. After the VT was taken at three levels 1) at the baseline, the tester performed the upper limb neurodynamic test 1(ULNT1) for each individual. During the sequence of the ULNT1, 2) vibration threshold was measured at initial onset of pain i.e. P1 and 3) short of maximal pain i.e. P2. Results: Repeated measures ANOVA was used to compare the VT differences within group and between groups. There was a statistical significant difference between the vibration threshold of diabetic and non diabetic group at the three levels with a p value < 0.001. Conclusion: Vibration threshold of the upper limb is higher in individuals with type II diabetes mellitus as
compared to non diabetic individuals.
Keywords: Vibration threshold, ULNT1, Diabetes mellitus
Full Text:
INTRODUCTION
Diabetes mellitus is a group of metabolic diseases characterized by hyperglycaemia resulting from defects in insulin secretion, insulin action, or both. Type II diabetes mellitus is most common form which is a disease of insulin resistance that usually has relative (rather than absolute) insulin deficiency1 . Earliest change in diabetic nerve function is alteration in axonal excitability due to changes in ion conductance of axon membrane due to metabolic processes directly affecting the nerves, microvascular abnormalities of the endoneurium and auto immune inflammation. Four main mechanisms have been postulated to underlie the pathogenesis of nerve pathology in diabetes mellitus, which are metabolic processes directly affecting nerve fibres, endoneurial microvascular disease, autoimmune inflammation and deranged neurotrophic support.2 It is due to these effects of hyperglycemia that peripheral nerve involvement is highly frequent in type II diabetes mellitus and it has been documented that one third of type II diabetic patients have peripheral neuropathy3 . Among the nerves, there is a tendency of the large diameter nerve fibers that mediate sense of vibration to get involved first in diabetes mellitus.2 Neurodynamic tests involve sequential limb movements that are employed to include the link between mechanical and physiological types of mechanisms. An aim of using these tests in assessment of a nerve is to stimulate mechanically and move neural tissues in order to gain an impression of their mobility and sensitivity to mechanical stresses so as to evoke the physiological responses.4 In order to assess the upper limb nerve function, the standard upper limb neuro dynamic test 1 (ULNT1) is usually used as it evokes symptoms of distribution of the median nerve because the forces generated by the test are biased towards this structure.4 There are various techniques of assessing the conductivity of nerve such as NCV that basically assesses the motor and sensory aspects of the nerve whereas the vibration threshold (VT) reflects particular function of the peripheral nervous system especially the somatosensory pathway.5 Type II diabetes mellitus patients have been shown to affect the multimodal sensory, reflex and motor systems in distal extremities. Mechanosensitivity in diabetes mellitus patients should be considered as an essential inclusion in the assessment to predict the extent of involvement of the nerve.6 Studies have also been done to determine the vibration threshold in lower limb in normal individuals but there is scanty literature available in comparison of the vibration threshold in the upper limb in type II diabetes mellitus patients with non diabetic individuals.
METHODOLOGY
Study Design
This study took place in department of physiotherapy, Manipal University, Manipal, India. A cross –sectional 2-group design was used. Completion of questionnaires and all measurement procedures were conducted in the same room on each occasion.
Subject Selection
Type II diabetic subjects in the study were selected from all patients presenting for the first time to physiotherapy outpatient and inpatient clinic over a one year period. 30 subjects with mean age of 55.60 ± 9.79 were included in the study. All new patients completed a simple questionnaire as part of the inclusion-exclusion procedure. On daily review of these first stage questionnaires, the clinical records of patients who provisionally met the inclusion criteria were subjected to secondary detailed screening by an experienced member of the physiotherapy faculty who is experienced the in the field of musculoskeletal physiotherapy and diabetic neuropathy. The Diabetic subjects with clinical signs of neuropathy were excluded from the study. After this screening, subjects who met inclusion criteria invited to participate in the study and were given further verbal and written information about the study, and were asked to read and sign a consent form. For controlled age matched normal subjects an advertisement was given in physiotherapy department and Manipal University for their voluntary participation in the study. To be considered for inclusion, the subjects must have been aged between 30 to 70 years, have had no history of diabetes, upper limb disorders, Cervicobrachial pain syndrome, Acute inflammatory/ demyelinating diseases, Any recent surgeries in upper limb. Finally, eligible 30 control subjects were selected by age to ensure a similar distribution to the patient group. The mean age of the subjects was 53.43±9.96. The subjects first session were to familiarize them with the equipment and vibration threshold testing tasks. All participants signed a written consent form prior to participating in the experiment. Ethics approval was obtained from the Manipal University Ethics Committee.
Measurement of Vibration Threshold (VT)
VT was measured by tester 1 at the baseline for both the groups using a bioesthesiometer capable of delivering a vibration of 100 Hz. The subjects were made to sit comfortably on a chair with hand and arm completely on the pillow. The probe of the Vibrometer was placed at the pulp of the distal phalanx of the thumb.7 Either right or left hand was tested. The subjects were shielded from the Vibrometer display during testing. At baseline, tester 1 first increased the vibration to a point where the subject perceived the stimulus. This was taken as appearance of vibration. Then the intensity was further increased and slowly reduced till they identified the disappearance of the stimulus. This measurement was done thrice and the average of the six values was taken as the vibration threshold. After the VT was taken at the baseline, the tester performed the ULNT1 (adopted from M.Shacklock)6 for each individual. For this a pressure biofeedback inflated to 50 mm Hg was used to prevent shoulder elevation. Then the shoulder was abducted to 90-110 degrees followed by complete external rotation, forearm supination, wrist and finger extension. The last component of ULNT1 was elbow extension and elbow extension value was recorded using universal goniometer as a measure of mechanosensitivity. During the sequence of the ULNT1, the occurrence of the first response of elbow extension i.e. pain considered as P1 was noted. The angle of its occurrence was measured with the universal Goniometer and VT at this position in the same manner as that of baseline was taken for both the groups by the tester 2. The next occurrence of the symptom i.e. P2 at which any further movement was intolerable was noted. The corresponding elbow extension angle of P2 was measured. The range of elbow extension was reduced until the feeling of discomfort disappeared and VT was measured at this point for both the groups by the tester 2. The reduction of elbow extension was adopted to avoid the masking of pain for perception of vibration. The measurement of vibration threshold was measured for both diabetic individuals and age matched normal individuals.
Data Analysis
The statistical analysis was done using the SPSS 14.0 for Windows software. The statistical significance value was set at 0.05 with 95% confidence interval and p value less than or equal to 0.05 would be considered as significant. Repeated measures ANOVA were used to compare the VT differences within group and between groups.
Results
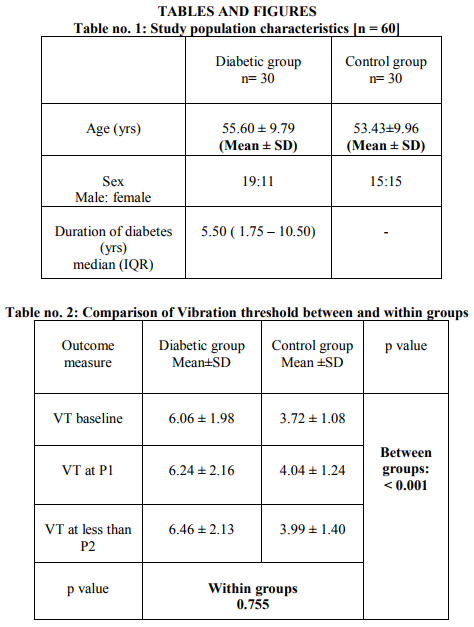
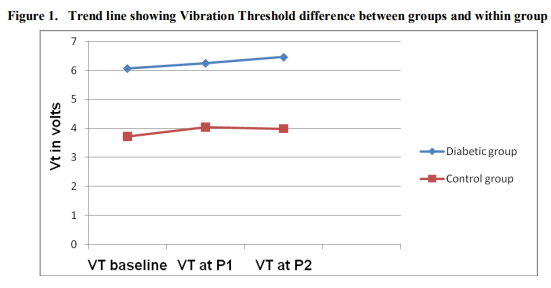
Demographic data regarding the age (yrs), sex and duration of individuals with type II diabetes mellitus and non diabetic individuals are shown in table no. 1 Analysis of repeated measures ANOVA shows the comparison of the vibration threshold between the diabetic and the non diabetic group at 3 levels i.e. VT at baseline, VT at P1 and VT at less than P2. There was a statistical significant difference between the vibration threshold of diabetic and non diabetic group at the three levels with a p value < 0.001. This states that the vibration threshold was found to be raised in the diabetic group at all the three levels compared to the non diabetic group. There was no statistical significant difference between the three levels within each group with a p value of 0.755.This states that there was no difference in vibration threshold during the ULNT1 procedure within each group (Table no. 2 and Figure 1) Thus vibration threshold of the upper limb is higher in individuals with type II diabetes mellitus as compared to non diabetic individuals. However, vibration threshold did not change within subjects of each group during the ULNT1 testing.
Discussion
Our study aimed at comparing the vibration threshold of the upper limb during ULNT1 in individuals with type II diabetes mellitus and non diabetic individuals. As per the results, the vibration threshold was found to be increased in the individuals with type II diabetes mellitus as compared to the non diabetic individuals. Vibration threshold is a measure of conductivity i.e. a function of the axon in conducting the impulse from the external receptor. Thus, alteration of the vibration threshold in type II diabetic individuals may be due various reasons. Studies in human and animal models with diabetes mellitus have shown reduced nerve perfusion and endoneurial hypoxia. Investigations on biopsy materials from patients with mild to severe neuropathy show graded structural changes in nerve microvasculature including basement membrane thickening, pericyte degeneration and endothelial cell hyperplasia. Arterio-venous shunting also contributes to the reduced endoneurial perfusion. These vascular changes strongly correlate with clinical defects and nerve pathology. Early vasa nervorum functional changes are caused by metabolic insults of diabetes, the balance between vasodilator and vasoconstrictor are altered.8 The findings of our study regarding the vibration threshold are in contrast with the study done by David A Gebler et al. They conducted a study to check the vibratory and thermal thresholds in normal and diabetic individuals using an Optacon Tactile Tester (OTT) and Thermal Sensitivity Tester. They did not find the vibratory and thermal threshold of diabetic subjects to be different from the normal individuals. But in diabetic individuals with neuropathy, the thermal and vibratory thresholds were found to be increased.9 .
Conclusion
Vibratory threshold of the upper limb in type II diabetic individuals is higher than the non diabetic individuals. Vibration threshold and Mechanosensitivity in diabetes mellitus patients should be considered as an essential inclusion in the assessment to predict the extent of involvement of the nerve.
References:
1. Fazan V, Vasconcelos C, Valença M, Nessler R, Moore K. Diabetic Peripheral Neuropathies: A Morphometric Overview. Int J Morphol 2010;28:51-64.
2. Raymond AA. Management of Diabetic Neuropathy. Malaysian Journal of Medical Sciences 2003;10:27-30.
3. Comi G, Corbo M. Metabolic neuropathies. Curr Opin Neurol 1998;11:523-9.
4. Shacklock M. Clinical Neurodynamics - A new system of musculoskeletal treatment. London: Elsiever 2005.63-65
5. Lise H, Jepsen JR, Sjogaard G. Vibrotactile sense in patients with different upper limb disorders compared with a control group. Int Arch Occ Env Hea 2006;79:593-601.
6. Boyd BS, Wanek L, Gray AT, Topp KS . Mechanosensitivity during lower extremity neurodynamic testing is diminished in individuals with Type 2 Diabetes Mellitus and peripheral neuropathy: a cross sectional study. BMC Neurology 2010;10:75.
7. Colette R, Jane G, Nicola J. P. Effect of straight leg raise examination and treatment on vibration thresholds in the lower limb: a pilot study in asymptomatic subjects. Man Ther 2005;10:136-143.
8. Cameron NE, Eaton SE. Vascular factors and metabolic interactions in the pathogenesis of diabetic neuropathy. Diabetologia 2001;44:1973-1988.
9. Gelber DA, Pfeifer MA, Broadstone VL, Munster EW, Peterson M, Arezzo JC. Components of variance for vibratory and thermal threshold testing in normal and diabetic subjects. J Diabetes Complications 1995;9:170-176.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





