IJCRR - 3(10), October, 2011
Pages: 168-176
Print Article
Download XML Download PDF
EFFECT OF CERVICAL SPINE MOBILIZATION IN THE TREATMENT OF MECHANICAL NECK PAIN-A
RANDOMIZED CLINICAL TRIAL
Author: Anupama Prabhu, Ravi Shankar Reddy, Ganesh BM
Category: Healthcare
Abstract:Background: Mechanical neck pain (MNP) is the most common type of neck pain having its occurrence in general population. In mechanical neck pain there is reduction in mobility of either a single segment or
multiple segments of cervical and thoracic spine in association with pain. This study attempted to
determine the effect of cervical mobilization in patients with mechanical neck pain.
Methods: 28 subjects were recruited and randomized into experimental and control group. The subjects in the experimental group received moist heat for 15 minutes, thoracic thrust manipulations and cervical
mobilization and control group received moist heat for 15 minutes and thoracic thrust manipulation. Both
the groups received intervention for a period of five sessions. The outcome measures Visual analog scale
(VAS), cervical range of motion (CROM) and neck disability index (NDI) were measured before the
intervention and following five sessions of intervention in both the groups.
Results: Pre and post comparison within the groups showed a significant difference in all the outcome measures i.e. VAS, NDI and CROM in both experimental and control groups (p< 0.05) but there was no
significant difference between the groups for all the outcome measures (P>0.05).
Conclusion: Both cervical mobilization and thoracic thrust mobilization was effective in the management
of MNP. Cervical mobilization was not superior to thoracic thrust manipulation alone in the management
of MNP.
Keywords: Mobilization, Mechanical neck pain
Full Text:
 NTRODUCTION
NTRODUCTION
Mechanical neck pain (MNP) is the most common type of neck pain having its occurrence in general population, accounting for 25% of all outpatient physical therapy visits, and resulting in considerable economic burden.1-3 It has been estimated that in any six months period 54% of adults will experience neck pain with approximately 5% having substantial activity limitation due to their neck disorder.4 Physical therapy is often the first treatment approach for patients with neck pain.2 MNP is defined as generalized neck pain and/or shoulder pain with symptoms provoked by neck postures, neck movements, or palpation of the neck musculature.2,3 Pathology remains obscure, but has been asserted to involve mechanical dysfunction of the spine, particularly zygapophyseal joints and related mechanical structures with clinical presentation of reduction in mobility of either a single or multiple segments of cervical spine in association with pain.5 Because of the biomechanical relationship between the cervical and thoracic spine, disturbance in joint mobility of one segment can serve as a contributor to the development of disorders in either segments.1 Physical therapy interventions in the management of mechanical neck pain include manual therapy, exercises, massage, thermotherapy and electrotherapy which aim to keep the neck moving as normally as possible.3,6 However, robust evidence to support these strategies is lacking. Spinal manual therapy techniques are commonly used in the management of musculoskeletal pain of spinal origin it has a pain relieving effect and results in more rapid restoration of function.7 Manual therapy interventions are one treatment strategy appropriate for patients with mechanical neck pain.1,2 Possible mechanisms to explain the effects of manual therapy include direct effects on articular/periarticular structures, neurophysiological mechanisms and a nonspecific placebo effect.7 Mobilization is passive movement performed in such a manner that it is at all times within the ability of the patient to prevent the movement if he or she so choose.8 Manipulation is a technique performed at a speed such that it has taken place before the person on whom it is performed is able to prevent it.8 Decreased mobility in the thoracic spine has been shown to be related to the presence of neck pain symptoms.3 Recently, evidence has begun to emerge for the use of manual therapy, specifically, thrust mobilization/manipulation procedures, directed at the thoracic spine in people with MNP.1-3,6 However, there is no literature containing information addressing effect of cervical mobilization with thoracic thrust manipulation in patients with MNP. Therefore, the purpose of this study was to examine the effect of cervical spine mobilization in addition to thoracic thrust manipulation in the management of mechanical neck pain.
METHODOLOGY
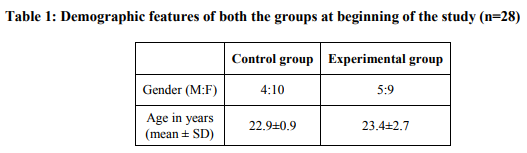
Subjects: A sample of 28 patients with a diagnosis of mechanical neck pain by a primary care physician were recruited from an outpatient clinic and randomly allocated to an experimental group and control group using block randomization method. Patients whose age ranged between 18 and 30 with mean age 23.17 ±0.6 with a diagnosis of mechanical neck pain for more than three months were recruited. Patients who had one or more of the following conditions such as: contraindication to manipulation, history of whiplash or cervical surgery, diagnosis of fibromyalgia syndrome, having undergone spinal manipulative therapy in the previous two months or loss of standing balance were excluded from the current study. Explanation and informed consent were obtained from each subject. This study was approved by the ethical review board of the university.
Outcome measures:
For the baseline examination and the subsequent follow-ups, each subject reported his/her intensity of neck pain by the Visual Analog Scale (VAS). Neck Disability index (NDI) was used to measure the disability of the patient. For objective measurements, subjects‘ cervical range of motion was measured by the cervical range of motion (CROM) device. The neck ranges were measured while patient sitting with feet rested on the ground, their hips and knees positioned at a right angle, and their back against a chair. The CROM device was set on the patients‘ head so that all three inclinometers for 3 cardinal planes read zero. The patients were instructed to perform a maximally active movement in each direction. Six conventional movements of the cervical spine were measured in order from flexion, extension, right lateral flexion, left lateral flexion, right rotation and left rotation.
PROCEDURE ]
Experimental group received cervical mobilization for 5 sessions (2/week), moist heat therapy for 15 min over the painful site and thoracic thrust manipulation. For Cervical mobilization patient was made to lie prone with neck slightly flexed and hands resting below the forehead. Grade III and Grade IV central Posterior-Anterior oscillatory mobilization targeted at spinous process was given as described by Maitland et al. Three sets of mobilization were given with one minute rest between each set. The level of cervical mobilization was determined according to clinical assessment (which includes movement analysis and palpation) by an experienced physiotherapist who had post-graduate training in spinal manipulative therapy and with at least 5 years of clinical experience in the management of neck pain patients with manual procedures. Moist heat was applied to neck and upper back by making the patient sit comfortably on a chair with head resting on a pillow and hands under the forehead for 15 – 20 minutes. For Thoracic thrust manipulation patient was made to lie prone with hands by his/her side manipulative physical therapist stood alongside the patient with right hand between spine and right scapula and left hand between spine and left scapula. Pressure transmission was through lateral surface of hypothenar eminence near pisiform bone. Ulnar border of each hand was placed in a line across the patient‘s back in parallel lines. Therapist‘s forearms were directed across the patient‘s back at right angles to the vertebral column, pisiform bone tucked into the space between paravertebral muscles and the spinous process. Slack was taken in the soft tissues by applying both PA and rotatory pressures. Rotary postero- anterior intervertebral pressure technique described by Maitland et al was used. Maximum of two attempts were performed at each level. Control group and received 5 sessions (2/week) of thoracic thrust together with the moist heat therapy for 15-20 minutes. All subjects were evaluated and assessed at baseline, immediately after 5 sessions of treatment by a blinded assessor.
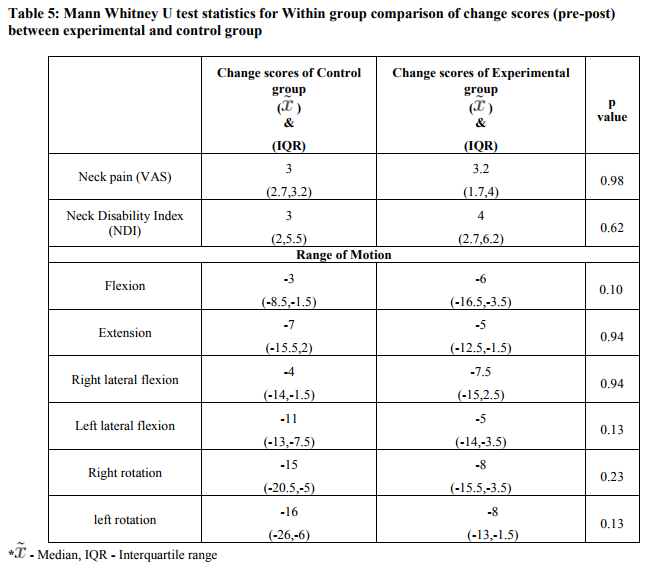
Data analysis: Data was statistically analyzed using SPSS package (version 16.0) software. A normal distribution of quantitative data was assessed by means of the Shapiro–Wilk test. Medians and inter quartile ranges were calculated for each variable. Baseline features were compared between groups by using Mann Whitney U-test. Wilcoxon signed rank test was used to assess Pre-post comparison of NDI, ROM and VAS within the groups.Mann-Whitney U-test was used to analyse the change scores of Pre and post NDI, ROM and VAS between the groups. p value ≤ 0.05 was considered significant.
RESULTS
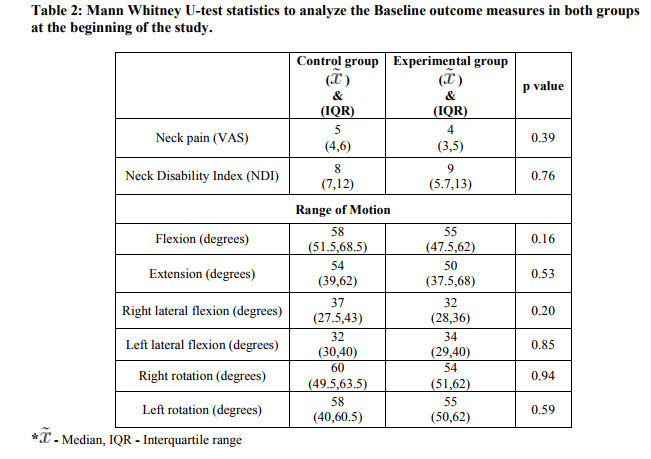
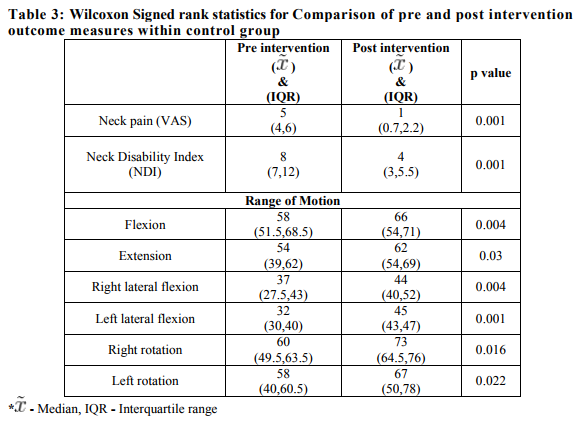
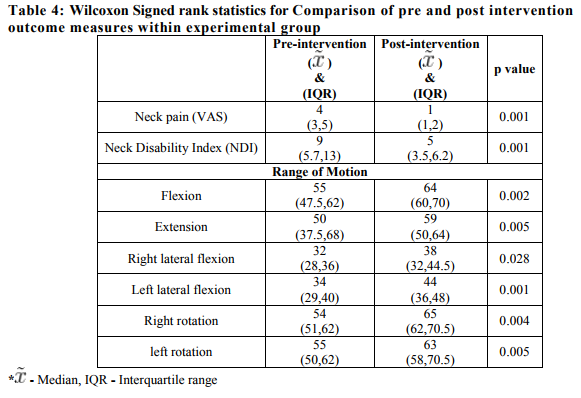
Shapiro-Wilk test for normality was checked and showed that data did not follow normal distribution. Hence, non-parametric tests were used to analyze the outcome variables. Our study mainly comprised of young population (23.17 ±0.6). No significant differences were found for gender and age between groups, so both groups were comparable in all respects at the start of the study (Table 1). Mann Whitney U-test was used to compare the baseline variables. No statistically significant difference in baseline levels of pain, range of motion and disability were detected between the groups (Table 2). Wilcoxon Signed rank test was used to analyze within group significance of outcome variables. There was a statistically significant difference between the pre-intervention and post-intervention scores in both cervical mobilization and thoracic thrust mobilization groups in terms of pain, range and disability (p≤0.05) (Table 3 and 4). Mann Whitney U test was used to analyze statistically significant difference between cervical mobilization and thoracic thrust mobilization groups, no significant difference between the groups was found for any of the outcome measure (p>0.05) (Table 5).
DISCUSSION
The results of our study demonstrated improvement in short term pain, cervical mobility and disability scores in both the groups. There was no significant difference between the groups for any of the outcome measures. Reduction in neck pain from thoracic spine manipulation intervention may be attributed to a restoration of normal biomechanics to this region, potentially lowering mechanical stresses and improving the distribution of forces in the cervical spine.1Decreased mobility in the thoracic spine was found to be associated with subjective complaints of neck pain.1,22 Disturbance in biomechanical link between the thoracic and cervical spine leads to abnormal distribution of forces in the cervical spine.1 Another mechanism could be that the thoracic thrust manipulative procedure was found to induce a reflex inhibition of pain or reflex muscle relaxation by modifying the discharge of proprioceptive group I and II afferents.3 which might have had an effect on improving pain, range and disability in both the groups. Superficial heating provided by moist heat has been found to decrease muscle spasm and improve function. Physiological effects include analgesia, increased flexibility of collagenous tissue, decreased spindle sensitivity and reduction of muscle spasm through selective decrease in excitation of nociceptive nerve endings.13
Range of motion
Biomechanical link between cervico-thoracic spine may be one reason why thoracic spine manipulation is beneficial.3Thrust manipulation reduces pain and spasm while increasing mobility through changes in muscle electrical activity, reducing muscle spasm and increasing inter-segmental joint play.3
Pain
It has been suggested that stimulation of large diameter, low threshold mechanoreceptors by spinal manual therapy may produce inhibition at the spinal cord level as per predictions of the gate control theory.7It has been speculated that immediate hypoalgesia following manual technique is related to the stimulation of descending inhibitory mechanisms.1
Disability
Delay in activation of deep cervical flexors and heightened activity of superficial muscles in MNP has its implications on the muscles capacity to generate torque, which can impair the function of the cervical spine.4 Cervical mobilization and thoracic thrust has shown to facilitate deep neck flexor muscles with a decreased co-activation of superficial neck flexors.7The reduction in disability obtained in this study can also be attributed to the improvement in range of motion and pain observed following treatment in both the groups. It is often believed that manual therapists must accurately identify a segmental impairment through careful palpation of vertebral movement or alignment and, once identified, treat the particular impairment by applying a specific amount of force to a single segment in a specific direction.3 However, all patients in our study received identical central PA cervical mobilization regardless of the clinical presentation. While this may seem counterintuitive to some philosophies, based on substandard levels of reliability with palpation techniques,11and studies suggesting non significant differences between the preferred and random mobilization in neck pain,5 we selected to deliver one specific technique to all patients. In cervical mobilization group there was no additional improvement seen when compared to control group, the reason could be due to the age group recruited in our study consisted of young individuals; problems‘ pertaining to neck pain here is less likely to be due to joint dysfunction and more of muscular dysfunction so cervical mobilization may not have showed an additional effect in experimental group. Recent studies have demonstrated that mobilization/manipulation techniques directed at impaired motion segments were no more beneficial than the treatment of randomly selected segments.1Which is in consensus with our study which shows thoracic thrust manipulation applied remote to the cervical spine have had indirect effect over the cervical area. The mechanism of action of cervical mobilization is similar to that of thoracic thrust manipulation hence the effect must have been neutralized. In this study grade III mobilization was used more predominantly than grade IV due to the lower pain thresholds in subjects, use of grade IV mobilization results in greater improvement in range as it address restriction more than pain. Studies have shown cervical spine manipulation to have immediate effect in reducing pain and increasing cervical ROM when compared to cervical mobilization, which has a delayed effect.5In a longer duration, cervical mobilization yielded similar mean reductions in pain and disability as cervical manipulation.5 A recent study conducted to compare the effect of cervical manipulation versus cervical mobilization has shown that time taken for recovery of neck pain and disability to be more in cervical mobilization group than cervical manipulation group.23Short term follow up in our study would have masked the effects of cervical mobilization.
The limitations of the study were that there was no long term follow up and all patients were recruited at one physiotherapy clinic, so the patients may not be representative of the general population.
CONCLUSION
Clinically meaningful and statistically significant improvement in both groups of patients over time suggests that cervical mobilization, as part of the thoracic spine thrust manipulation treatment did not influence the results of the treatment.
References:
1. Cleland A, Childs D, McRae M, Palmer A, Stowell T. Immediate effects of thoracic manipulation in patients with neck pain: a randomized clinical trial. Man Ther. 2005;10:127–135
2. Iglesias J, Penas C, Cleland J, Vega M. Thoracic spine manipulation for the management of patients with neck pain: A randomized clinical trial. J Orthop Sports Phys Ther. 2009;39:20-27.
3. Iglesias J, Penas C, Cleland J, Sendin F, Cerro L, Sanchez R. Inclusion of thoracic spine thrust manipulation into an electrotherapy/thermal program for the management of patients with acute mechanical neck pain: A randomized clinical trial. Man Ther. 2009;14:306-313.
4. Shaun o‘ L, Falls D, Elliot J, Jull G. Muscle Dysfunction in cervical spine pain: Implications for assessment and management. J Orthop Sports Phys Ther. 2009;39:324-333
5. Kanlayanaphotporn R, Adit C, Vachalathiti R. The immediate effects of Mobilization technique on pain and Range of Motion in patients presenting with unilateral neck pain: International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 10 October 2011 173 RCT. Arch Phys Med Rehab. 2009;90:187- 92.
6. Cleland A, Glynn P, Whitman J, Eberhart S, MacDonald C, Childs J. Short-term effects of thrust versus nonthrust mobilization/manipulation directed at the thoracic spine in patients with neck pain: A randomized clinical trial. Phys Ther. 2007;87:431-440.
7. Sterling M, Jull G, Wright A. Cervical mobilization: Concurrent effects on pain, sympathetic nervous system activity and motor activity. Man Ther. 2001;6:72-81.
8. Maitland D, Hengeveld E, Banks K, English K. Maitland‘s Vertebral Manipulation. 7th ed.2005.
9. Gross R, Haines T, Goldsmith c, Santaguida L, McLaughlin M, Peloso P et al. Knowledge to Action: A challenge for neck pain treatment. Jour of Ortho and Spo Phys Ther. 2009;39:351-363.
10. Cleland JA, Childs JD, Fritz J, Whitman J, Eberhart SL. Development of a clinical prediction rule for guiding treatment of a subgroup of patients with neck pain: use of thoracic spine manipulation, exercise and patient education. Phys Ther. 2007a;87:9- 23.
11. Cleland J, Childs J, Fritz J, Whitman M. Inter-rater reliability of the history and physical examination in patients with mechanical neck pain. Arch Phys Med Rehabil 2006;87:1388-95.
12. French SD, Cameron M, Walker BF, Reggars JW, Esterman AJ. Superficial heat or cold for low back pain. Cochrane database of systematic review.2006.
13. Vasudevan V. Physical rehabilitation in managing pain. International association for the study of pain.1997;5.
14. Bialosky JE, Bishop D M, Price D, Robinson E, George Z. the mechanisms of manual therapy in the treatment of musculoskeletal pain: A comprehensive model. Man Ther.2009;14:531-538.
15. Vernon H. Rehabilitation of the spine. In; John P Butler, editors. Pain and disability questionnaire in chiropractic rehabilitation. 2 nd edition. California: Williams and Wilkins.1996;57-59.
16. Moeti P, Marchetti G. Clinical outcome from mechanical intermittent cervical traction for the treatment of cervical radiculopathy: A case series. J Orthop Sports Phy Ther.2001;3:207-13.
17. Chan Ci, Clair A, Edmondston J. Validity of the Neck Disability Index and Disability Scale for measuring disability associated with chronic, non-traumatic neck pain. Man Ther. 2009;14:433-438.
18. Kelvin J. Assessment of published reliability studies for cervical spine Range of motion measurement tools. J Manipulative Physiol Ther. 2000; 23:180-195.
19. Michel T, Cecile S, Anne-Marie B. Criterion valisity of Cervical Range of Motion (CROM) device for Rotational range of motion on healthy adults: J Orthop Sports Phys Ther. 2006;36:242-248.
20. Tousignant M, de Bellefeuille L, O‘Donoughue S, Grahovac S. Criterion validity of the cervical range of motion (CROM) goniometer for cervical flexion and extension. Spine. 2000;25:324-330.
21. Tousignant M, Duclos E, Lafleche S, et al. Validity study for the cervical range of motion device used for lateral flexion in patients with neck pain. Spine. 2002;27:812- 817.
22. Cheung Lau, Wing Chiu, Hing Lam. The effectiveness of thoracic manipulation on patients with chronic mechanical neck pain International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 10 October 2011 174 – A randomized controlled trial. Man Ther.2011;16:141-147.
23. Leaver M, Maher G, Herbert R D, Latimer J, McAuley H, Jull G et al. A randomized controlled trial comparing manipulation with mobilization for recent onset neck pain. Arch Phys Med Rehabil. 2010;91:1313- 1318.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





