IJCRR - 4(18), September, 2012
Pages: 123-128
Date of Publication: 29-Sep-2012
Print Article
Download XML Download PDF
FORMATION OF MEDIAN NERVE BY MULTIPLE LATERAL ROOTS
Author: Sharadkumar Pralhad Sawant, Shaguphta T. Shaikh, Rakhi Milind More
Category: Healthcare
Abstract:Aim: To study the formation of median nerve by multiple lateral roots. Materials and Methods: 50 upper limbs of 25 donated embalmed cadavers (20 males and 5 females) were studied in the department of Anatomy at K. J. Somaiya Medical College, Sion, Mumbai, INDIA, the formation of median nerve by multiple lateral roots were observed. The finding was noted after thorough and meticulous dissection of the upper limbs of both sides (axilla, arm, forearm and palm) of 25 cadavers. The photographs of the variations were taken for proper documentation. Observations: The variations were found in two cases. In the first case the median nerve was formed by multiple roots- three roots from lateral cord and one root from medial cord of brachial plexus. In the second case out of the three roots forming the anomalous median nerve, two were from lateral cord and one from medial cord of brachial plexus. However, the distribution of the anomalous median nerve was normal in arm, forearm and palm. The arterial pattern in the arm (axillary and brachial arteries) was also normal in both the specimens. Conclusion: The presence of such type of variations are clinically important for surgeons, orthopaedicians and anaesthetist performing pain management therapies on the upper limb.
Keywords: Axilla, Brachial Plexus, Median Nerve, Multiple Roots, Pain Management Therapy.
Full Text:
INTRODUCTION
The median nerve is normally formed by the union of lateral root of median nerve arising from the lateral cord (C5, C6, C7) of brachial plexus and medial root of median nerve arising from the medial cord (C8, T1) of brachial plexus anterior to the axillary artery. Some fibres from C7 often leave the lateral root to join the ulnar nerve. Clinically they are believed to be mainly motor to the flexor carpi ulnaris. The median nerve enters the arm at first lateral to the brachial artery. Near the insertion of the coracobrachialis, it crosses in front of the artery, descending medial to it, to the cubital fossa, where it is posterior to the bicipital aponeurosis and anterior to the brachialis. It usually enters the forearm between the heads of the pronator teres, crossing to the lateral side of the ulnar artery and separated from it by the deep head of pronator teres (1). Anomalous pattern of median nerve can be explained on the basis of embryological development The upper limb buds lie opposite the lower five cervical and upper two thoracic segments. As soon as the buds form, the ventral primary rami of the spinal nerves penetrate into the mesenchyme of limb bud. Immediately the nerves enter the limb bud, they establish intimate contact with the differentiating mesodermal condensations and the early contact between nerve and muscle cells is a prerequisite for their complete functional differentiation (2). The growth as well as the path finding of nerve fibres towards the target is dependent upon concentration gradient of a group of cell surface receptors in the environment (1). Several signalling molecules and transcription factors have been identified which induce the differentiation of the dorsal and ventral motor horn cells The high percentage of anomalies as mentioned above emphasizes the complexities and irregularities of this anatomic region with regard to surgical approaches (3). Knowledge of such variations is important for surgeons to perform surgical procedures in the axillary region and arm (4). Considering the high percentage of anomalies in the formation of median nerve and its paramount clinical importance, the present variations are documented.
MATERIALS AND METHODS
50 upper limbs of 25 donated embalmed cadavers (20 males and 5 females) were studied in the department of Anatomy at K. J. Somaiya Medical College, Sion, Mumbai, INDIA, the formation of median nerve by multiple lateral roots were observed. The findings were noted after thorough and meticulous dissection of the upper limbs of both sides (axilla, arm, forearm and palm) of 25 cadavers. Arterial pattern of upper limb was also noted. Photographs of the abnormalities were taken for proper documentation.
OBSERVATIONS
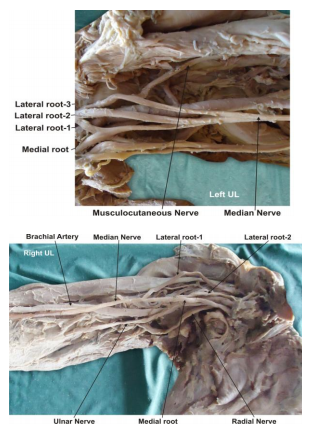
In the present study, the variations related to the formation of median nerve were found in two cases. In the first case the median nerve was formed by multiple roots- three roots from lateral cord and one root from medial cord of brachial plexus. In the second case out of the three roots forming the anomalous median nerve, two were from the lateral cord and one from the medial cord of brachial plexus. However, the distribution of the anomalous median nerve was normal in arm, forearm and palm. The arterial pattern in the arm (axillary and brachial arteries) was also normal in both the specimens.
DISCUSSION
Neural variations of the brachium constitute an important anatomical and clinical entity. Although frequently reported, if accompanied by other anomalies, they deserve special mention in anatomical literature. The nerves of the extremities are especially vulnerable to injury because of their long course and superficial distribution. The variations related to the formation of median nerve were found in literature. The variations related to the formation of median nerve by more than two roots are relatively uncommon as compared to the other types of variations of median nerve. Most of the variations were related to anomalous relationship between median and musculocutaneous nerves. As found in literature, it was documented that the lateral root was small and the musculocutaneous nerve was connected with median nerve in the arm (5). Another study involving dissection of ten cadavers,mentioned failure of separation of musculocutaneous nerve from the median nerve and the latter therefore gave off the branches that should arise from musculocutaneous nerve, namely branches to coracobrachialis, biceps brachii and major part of brachialis (6). The variations related to the formation of median nerve by more than two roots which have been observed in the present study are rare as revealed by survey of literature. These variations can be explained on the embryological basis. The first indication of limb musculature is observed in the seventh week of development as condensation of mesenchyme near the base of the limb buds. With further elongation of the limb buds, the muscle tissue splits into flexor and extensor compartments. The upper limb buds lie opposite the lower five cervical and upper two thoracic segments. As soon as the buds form, ventral primary rami from the spinal nerves penetrate into the mesenchyme. At first, each ventral ramus divides into dorsal and ventral branches, but soon these branches unite to form named peripheral nerves which supply extensor and flexor group of muscles respectively. Immediately after the above mentioned rearrangement of nerves, they enter the limb buds and establish an intimate contact with the differentiating mesodermal condensations and this early contact between the nerve and muscle cells is a prerequisite for their complete functional differentiation (2). Over the years, two principal theories have emerged concerning the directional growth of nerve fibres – the neurotropism or chemotropism hypothesis of Ramon et al (7) and the principle of contact-guidance of Weiss (8). The salient feature of chemotropism is that axonal growth cones act as sensors to concentration gradients of molecules in the environment and grow up the gradient towards the source, i.e. the target. There is no doubt, however that contact guidance mechanisms operate in parallel with neurotropism. Adhesion to the structures with which the growth cone contacts also plays a role. A group of cell surface receptors viz. neural cell adhesion molecule (N-CAM) and L1 and the Cadherins act as transcription factors which recognize and bind to components of the extracellular matrix. Thus, both cell-cell and cellmatrix interactions may be involved in axonal path finding (1). Over or under expression of one or multiple transcription factors as mentioned above have been found to be responsible for the variations in the formation, relation and distribution of the motor nerve fibers (1). Chauhan et al strongly recommend the consideration of the phylogeny and the development of the nerves of the upper limb for the interpretation of the nerve anomalies of the arm (9). The presence of such communications may be attributed to random factors influencing the mechanism of formation of limb muscles and the peripheral nerves during embryonic life. Significant variations in nerve patterns may be a result of altered signaling between mesenchymal cells and neuronal growth cones (10) or circulatory factors at the time of fusion of brachial plexus cords (11). Iwata believed that the human brachial plexus appears as a single radicular cone in the upper limb bud, which divides longitudinally into ventral and the dorsal segments. The ventral segments give roots to the median and the ulnar nerves with musculocutaneous nerve arising from the median nerve. He further kept the possibility of failure of the differentiation as a cause for some of the fibers taking an aberrant course as a communicating branch (12). Chiarapattanakom et al are of the opinion that the limb muscles develop from the mesenchyme of local origin, while axons of spinal nerves grow distally to reach the muscles and/or skin. They blamed the lack of coordination between the formation of the limb muscles and their innervation for appearance of a communicating branch (13). Anastomosis between the musculocutaneous nerve and the median nerve is by far the commonest and frequent of all the variations that are observed among the branches of the brachial plexus (14). Li Minor categorized these communications into following five type: In type I, there is no communication between the median nerve and the musculocutaneous nerve, in type II, the fibers of the lateral root of the median nerve pass through the musculocutaneous nerve and join the median nerve in the middle of the arm, whereas in type III, the lateral root fibers of the median nerve pass along the musculocutaneous nerve and after some distance, leave it to form the lateral root of the median nerve. In type IV, the musculocutaneous nerve fibers join the lateral root of the median nerve and after some distance the musculocutaneous nerve arises from the median nerve. In type V, the musculocutaneous nerve is absent and the entire fibers of the musculocutaneous nerve pass through the lateral root and fibers to the muscles supplied by musculocutaneous nerve branch out directly from the median nerve (15). The most frequent variation is the presence of a communicating branch that emerges from the musculocutaneous nerve and goes distally to join the median nerve, an anastomosis observed in the lower third of arm (16). If this branch is given off in upper third of the arm, it is generally considered as third (double lateral) root of the median nerve (16). In the present case, the musculocutaneous nerve in upper third of the arm, passed medially downwards and joined the median nerve. It can be considered as the double lateral root of the median nerve or in other words the median nerve can be said to be formed by three roots: a) one from the lateral cord; b) one from the musculocutaneous nerve; c) and the third from the medial cord. Similar variation was observed earlier by different authors - The median nerve, instead of having two roots may have three roots - either one each from lateral cord, medial cord and musculocutaneous nerve (9) or two from lateral cord and one from the medial cord (17) or it may have even four roots – three from the lateral cord and one from the medial cord (18). Knowledge of anatomical variations of these nerves at the level of upper arm is essential in light of the frequency with which surgery is performed in the axilla and the surgical neck of the humerus (19). The variations as noted in the present study may be attributed to over or under expression of one or more transcription factors as mentioned above. The variations in the formation and relations of median nerve in the arm bear remarkable clinical significance. Considering these variations Rao advocated that the clinicians and surgeons should be aware of such variations while performing surgical procedure in this region (20). Injury to such a variant nerve in the proximal arm may lead to a galaxy of manifestations including sensory, motor, vasomotor and trophic changes (21). The possible clinical implications of these variations relating either to the surgical approach to the shoulder joint and entrapment syndromes are important (22). Anomalies of axillary or brachial artery are frequently related to unusual pattern of brachial plexus and median nerve (23). However, in the present study no abnormal arterial pattern was detected.
Clinical Significance
The anatomical variation described here has practical implications, since injury to the median nerve in the axilla or arm would, in this case, have caused unexpected paresis or paralysis of the flexor musculature of the elbow and hypoesthesia of the lateral surface of the forearm, in addition to the classical signs that are already well known. Injury to the median nerve could occur in cases of open or closed trauma to the arm, such as bullet and blade wounds or during surgeries on the axilla or arm. The median nerve and its roots are close to the axillary vein, which is used as the most cranial limit for axillary lymph node dissection, a procedure used in treating certain tumors, such as breast carcinoma and melanoma. If the dissection extends more cranially than normal, injury to the median nerve (or to its medial root) may occur, with consequent dysfunction of the flexor musculature of the elbow if the anatomical variation described here is present. It would not be unlikely for such accidents to occur even with the most eminent surgeons, considering that the classical concept is that the median nerve does not give rise to branches in the arm (24).
CONCLUSION
The variations in the formation of median nerve by multiple lateral roots are clinically important for surgeons, orthopaedicians and anaesthetist performing pain management therapies on the upper limb. These variations are compered with the earlier data and it is concluded that variations in branching pattern of cords of brachial plexus are a rule rather than exception. A lack of awareness of variations with different patterns might complicate surgical repair and may cause ineffective nerve blockade.
Competing Interests:
The authors declare that they have no competing interests.
Authors' contributions:
SPS wrote the case report, performed the literature review and obtained the photograph for the study. RMM performed the literature search and assisted with writing the paper. STS conceived the study and helped to draft the manuscript. All authors have read and approved the final version manuscript.
ACKNOWLEDGEMENT
All the authors wish to convey our sincere thanks to Dr. Arif A. Faruqui for his valuable help, support and inspiration. Authors also acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Williams P.L., Bannister L.H., Berry M.M. et al. Gray’s Anatomy. In: Nervous System. 38th ed. London Churchill Livingstone, 1999: 231- 232,1270.
2. Saddler T.W. Langman’s Medical Embryology. In: Muscular system. 10th ed. Philadelphia Lippincott Williams and Wilkins, 2006: 146-147.
3. Edglseder WA JR, Goldman M. Anatomic variations of the musculocutaneous nerve in the arm. Amer J Orthop 1997; 26: 777-80.
4. Uysal II, Seker M, Karabulut AK, Buyukmumcu M, Ziylan T. Brachial plexus variation in human foetuses. Neurosurgery 2003; 53: 676-84; discussion 684.
5. Standring S, Ellis H, Healy JC, Johnson D et al. Gray’s Anatomy. In: General organisation and surface anatomy of the upper limb.39th ed. Philadelphia Elsevier Churchill Livingstone, 2005: 803-4.
6. Guha R, Palit S. A rare variation of anomalous median nerve with absent musculocutaneous nerve and high up division of brachial artery. J Interacad 2005; 9: 398-403.
7. Ramon Y, Cajal S. The neurotropism or chemotropism hypothesis. Trab Lab Invest Biol 1919; 17: 65-8.
8. Weiss P. Nerve patterns: the mechanics of nerve growth. Growth (suppl 5) 1941; 163- 203.
9. Chauhan, R., Roy, TS. Communication between the median and musculocutaneous nerve: A case report. Journal of Anatomical Society of India, 2002, vol. 51, n. 1, p. 72-75.
10. Abhaya, A., Bhardwaj, R., Prakash, R. Dual origin of musculocutaneous nerve. Journal of Anatomical Society of India, 2003, vol. 52, n. 1, p. 94.
11. Kosugi, K. Mortia, T., Yamashita, H. Branching pattern of the musculocutaneous nerve. 1. Cases possessing normal biceps brachii. Jikeakai Medical Journal, 1986, vol. 33, p. 63-71.
12. Iwata, H. Studies on the development of the brachial plexus in Japanese embryo. Republic Department Anatomy Mie Prefect University School of Medicine, 1960, vol. 13, p. 129-144.
13. Chiarapattanakom, P., Leechavengvons, S., Witoonchart, K., Uerpairojkit, C., Thuvasethakul, P. Anatomy and internal topography of the musculocutaneous nerve: The nerves to the biceps and brachials muscle. Journal of Hand Surgery, 1998, vol. 23A, p. 250-255.
14. Venieratos, D., Anagnostopoulou, S. Classification of communications between the musculocutaneous and median nerves. Clinical Anatomy, 1998, vol. 11, p. 327-331.
15. Li Minor, JM. A rare variant of median and musculocutaneous nerves in man. Archives Anatomy Histology Embryology, 1992, vol. 73, p. 33-42.
16. Bergman, RA., Afifi, AK., Miyauchir, RA. Ilustrated encyclopedia of human anatomic variation. In: NERVOUS system - plexuses. 1988. Available from: http://virtualhospital.com. Universityofiowacare.
17. Mohapatra, BB., Chinara, PK., Dutta, BK., Nayak, AK. Variation in the formation and branching pattern of median nerve. Journal of Anatomical Society of India, 2004, vol. 53, n. 1, p. 31-66.
18. Uzun, A., Seelig, LL. A variation in the formation of the median nerve: communicating branch between the musculocutaneous and median nerves in man. Folia Morphologica (Warsz), 2001, vol. 60 , n. 2, p. 99-101.
19. Leffert, RD. Anatomy of the brachial plexus. New York: Churchill Livingstone, 1985. 384 p.
20. Rao PPV, Chaudhary SC. Communication of Musculocutaneous nerve with the median nerve. East Afr Med J 2000; 77: 498-503.
21. Saeed M, Rufai AA. Median and musculocutaneous nerves: variant formation and distribution. Clin Anat 2003; 16: 453-7.
22. Venieratos D, Anagnostopoulou S. Classification of communication between musculocutaneous and median nerves. Clin Anat 1998; 11: 327-31.
23. Basar R, Aldur MM, Celik HH, Yuksel M, Tascioglu AB. A connecting branch between the musculocutaneouos nerve and the median nerve. Morphologie 2000; 84: 25-7.
24. FregnanI, JHTG., Macéa, MIM., Pereira, CSB., Barros, MD., Macéa, JR. Absence of the musculocutaneous nerve: a rare anatomical variation with possible clinical-surgical implications. Sao Paulo Medical Journal, 2008, vol. 126, n. 5, p. 288-90. PMid:19099164.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





