IJCRR - 4(3), February, 2012
Pages: 93-99
Print Article
Download XML Download PDF
ESTHETIC AND FUNCTIONAL REHABILITATION OF THE PATIENT WITH SEVERELY WORN DENTITION
USING TWIN STAGE PROCEDURE: A CASE REPORT
Author: Naresh HG Shetty, Manoj Shetty, Krishna Prasad D.
Category: Healthcare
Abstract:The form function and pathofunction of the dynamic masticatory system comprises one of the most fascinating, basic and important areas of interest in dentistry. The explosion of technological and procedural advances coupled with improved materials herald a new age in dentistry. In this age of the ?esthetic revolution' and the ?extreme makeover' factors that control occlusal stability are usually overlooked. Even though a full-mouth reconstruction can be relatively complex, it does not have to be a long or complicated process in patient's perspectives. The severe wear of anterior teeth facilitates
the loss of anterior guidance, which protects the posterior teeth from wear during excursive movement. The collapse of posterior teeth also results in the loss of normal occlusal plane and the reduction of the vertical dimension. This case report describes prosthetic rehabilitation using the Hobo and Takayama twin-stage procedure for a patient with esthetically and functionally compromised dentition. The final prosthesis with this twin-stage procedure ensured a restoration with a predictable posterior disclusion and anterior guidance in harmony with the condylar path.
Keywords: Full mouth rehabilitation, Hobo‘s twin stage, Effective cusp angle, Posterior disocclusion.
Full Text:
INTRODUCTION
Though the full-mouth rehabilitation and its philosophies are often intrigue in nature, but the esthetic and functional accomplishment of rehabilitation is always satisfying. The gradual wear of the occlusal surfaces of teeth is a normal process during the lifetime of a patient. However, excessive occlusal wear can result in pulpal pathology, occlusal disharmony, impaired function, and esthetic disfigurement. Tooth wear can be classified as attrition, abrasion, and erosion depending on its cause. A differential diagnosis is not always possible because, in many situations, there exists a combination of these processes.Therefore, it is important to identify the factor that contribute to excessive wear and to evaluate alteration of the vertical dimension of occlusion (VDO) caused by the worn dentition. As teeth are worn, the alveolar bone undergoes an adaptive process and compensates for the loss of tooth structure to maintain the vertical dimension of occlusion. Therefore, vertical dimension of occlusion should be conservative and should not be changed without careful approach. Anterior guidance is crucial in human occlusion because it influences molar disclusion that controls horizontal forces. This case reports the satisfactory clinical outcome achieved by restoring the vertical dimension with an improvement in esthetics and function. In this case Hobo-Takayama method was incorporated for creating molar disclusion using a twin-stage procedure.
CASE REPORT
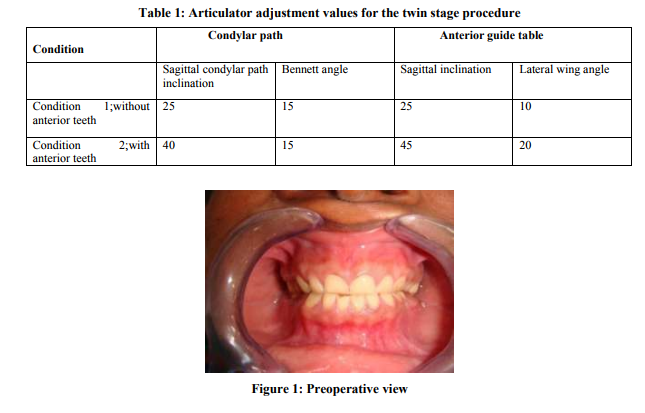
A healthy 44 year-old woman patient was reported to the department of prosthodontics, A B Shetty Memorial Institute of Dental Sciences, Mangalore, Karnataka, India, with a chief complaint of severely worn dentition, unpleasant smile, generalized sensitivity and difficulty in chewing(Fig 1) .The medical history was non-contributory. The patient‘s dental history indicated faulty tooth brushing habit, and extraction of 25,36 due to caries .The patient denied for any symptoms of temporomandibular joint disorder or myofacial pain dysfunction syndrome.
Clinical findings Extra oral findings; The patient had no gross facial asymmetry, muscle tenderness. The temporomandibular joints, muscles of mastication, and facial expressions were asymptomatic Intraoral findings; The maxillary and mandibular arch were partially dentate with tooth 25, 36, 38, missing. No gross abnormalities were noted in the overall soft tissues of the lips, cheeks, tongue, oral mucosa, and pharynx. Occlusion; Generalized severe attrition was noted. The patient presented with bilateral class I molar and the patient‘s lateral excursions showed canine guided occlusion. The patient was diagnosed with severe attrition with loss of vertical dimension. Treatment goals To restore the entire severely worn dentition to function and optimal esthetics Centric relation occlusion with maximum number of tooth contacts with no change in established vertical dimension To develop a canine guided occlusion Twin stage procedure to produce a definite amount of disocclusion during eccentric movements
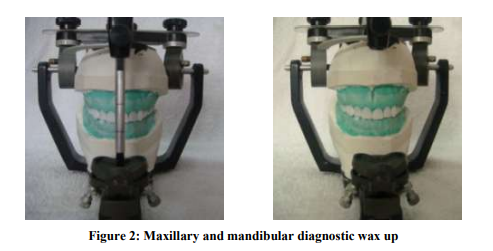
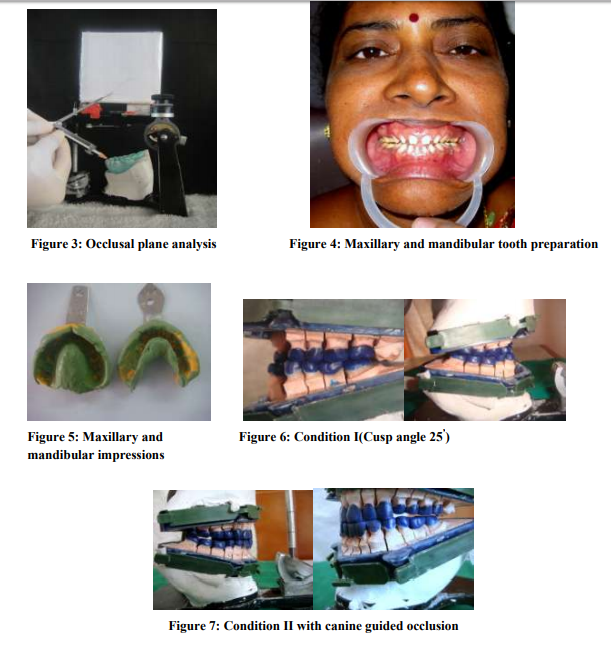
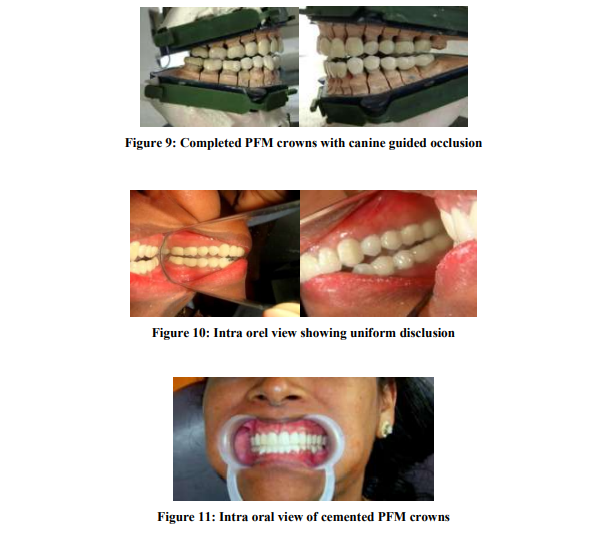
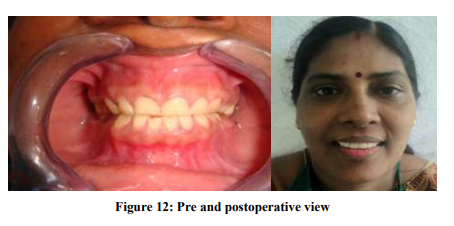
Treatment procedure The patient received oral prophylaxis, and reinforcement of oral hygiene practises. Patient was advised for intentional root canal therapy for 31, 32, 41, and 42 due to decreased tooth structure. As there was clinical evaluation of reduced vertical dimension of occlusion, full mouth rehabilitation with increasing vertical dimension of occlusion was planned. Patient‘s informed consent was taken prior to treatment. Two sets of diagnostic impressions were made using irreversible hydrocolloid and diagnostic casts were obtained. Maxillary casts were mounted using an earpiece facebow (Hanau springbow no. 0103280) onto a Hanau arcon articulator (ALL 182/183 Wide –Vue series, Waterpik, USA) and mandibular cast was mounted using interocclusal aluwax (Aluwax dental products, Michigan, USA) record. Diagnostic wax up was prepared to proper size shape and contour (Fig 2). Mandibular posterior occlusal plane was analysed using occlusal plane analyser (Fig 3). On analysis all mandibular teeth followed the curve of spee. Maxillary left third molar was supraerrupted which required occlusal correction. Mandibular anterior teeth required intentional root canal treatment followed by post and core .Maxillary occlusal wax up was done to maximum intercuspation. Anterior wax up was checked for proper anterior guidance to achieve disocclusion in eccentric movements Meanwhile a maxillary occlusal splint was fabricated at an increased occlusal vertical dimension of 2 mm using heat cured acrylic resin. The occlusal splint was inserted and adjusted. Two weeks later the patient reported with no difficulties in adapting to the new position. Hence full mouth rehabilitation was planned at increased vertical dimension of 2mm. Tooth preparations for metal ceramic crowns were completed for the entire dentition (Fig 4). A final full arch impression for maxillary and mandibular teeth was made using poly vinyl siloxane (Express™ XT ,3M ESPE) impression material with double mix single impression technique (Fig 5). The casts were poured in die stone (Kalrock; Kalabhai Pvt.Ltd, Mumbai, India), which was later secured to a die lock tray. This assembly was mounted on a Hanau arcon articulator using face bow (Hanau springbow).Mandibular die lock tray was mounted using centric interocclusal record made in aluwax at previously determined vertical dimension. Provisional crowns were made (Protemp II, 3M ESPE dental products, St Paul, USA) from diagnostic wax up. Provisional restorations were cemented using zinc oxide non eugenol temporary cement (Temp bond cement, Kerr, USA). Articulator was programmed to condition I twin stage procedure (As in Table 1) maxillary and mandibular anterior segment was removed, and posterior teeth wax build up was completed to achieve balanced articulation, which helped in achieving standard effective cusp angle of 25‘ .(Fig 6)Then anterior wax build up was carried out after the values had been adjusted to condition II of twin stage procedure (Table 1) to achieve an incisal guidance of 40‘which produced a standard amount of disocclusion.(Fig 7) All wax patterns were cast and metal units were tried in and adjusted for proximal contacts and occlusion. Definite restorations with porcelain fused to metal crowns exhibiting vital and natural appearance with proper contour were designed. Completed porcelain fused metal crown showing posterior balanced articulation (Condition I)(Fig 8) and uniform disocclusion Condition II)(Fig 9),and intra orally showing the same(Fig10).Permanent cementation was done with glass ionomer Type 1 (GC Goldlabel, GC Group. Tokyo luting cement). Oral hygiene instructions were reviewed, emphasizing brushing habits and the use of floss for better maintenance of the prosthesis. Follow-up was carried out at regular intervals and the patient's post-operative condition was satisfactory (Fig 11, 12)
DISCUSSION
Aesthetic and functional restoration of the severely worn dentition represents a significant clinical challenge. The complications with severely attrited teeth demand a circumspect treatment plan and proper sequencing of therapy to ensure an optimal result for both the patient and the clinician. Proper treatment sequencing is critical when a patient requires multiple fixed restorations. The vertical dimension, centric relation, and occlusal plane must be determined first, followed by a diagnostic wax up which is essential for fixed prosthesis. An accurate diagnostic and interdisciplinary approach is necessary for obtaining improved, conservative and predictable results. Full mouth rehabilitation seeks to convert all unfavourable forces on the teeth which inevitably induce pathologic conditions, into favourable forces which permit normal function and therefore induce healthy conditions. A variety of techniques may be used in simultaneous constructions to obtain complete arch dies and mounted casts. When all of the prepared teeth are on a single articulator, there is flexibility in developing the occlusal plane, occlusal theme, embrasures, crown contour, and esthetics. The chairside disadvantages include 1 arduous, unpredictable patient visits, 2 full arch anaesthesia,3 full arch chairside treatment restorations,4 multiple occlusal records, and 5,6,7 possible loss of the vertical dimension of occlusion. An alternative approach to the full-mouth simultaneous reconstruction is to complete one quadrant before beginning another. The advantages of this approach are that it is primarily chairside and includes preparation and final impressions of select teeth, maintenance of vertical dimension, quadrant anaesthesia, and shorter, predictable appointments. The disadvantages of the quadrant reconstruction include restrictions for achieving ideal occlusion when altering the vertical dimension, occlusal plane, and embrasure development. The existing opposing dentition limits the reconstruction of an isolated quadrant. Esthetic consistency can be compromised because the porcelain restorations are made in stages. The advantages of the simultaneous and quadrant full-mouth reconstruction are combined in the present technique.8 The mechanism of anterior guidance was reviewed from recent mandibular movement studies to provide a basis for understanding the twin-stage technique, which is a practical method for establishing anterior guidance from the condylar path. 9,10 Hobo and Takayama studied the influence of condylar path, incisal path and the cusp angle on the amount of disocclusion. They concluded that cusp angle was the most reliable and was used as a new determinant of occlusion. Twin stage procedure proposed by Hobo and Takayama was adopted for wax build up because studies have proposed that it is possible to accurately control the amount of disocclusion on the restoration without measuring the condylar path. Anterior guidance and the condylar path previously were considered independent factors. It is an established fact that anterior guidance influences the working condylar path and even changes when the lateral incisal path deviates from the optimal orbit. This supports the hypothesis that anterior guidance and the condylar path are dependent factors. In setting anterior guidance, it is recommended to set the working condyle so that it moves straight outward along the transverse horizontal axis. The angle of hinge rotation produced by the angular difference between anterior guidance and the condylar path assists posterior disclusion but is not solely responsible. The anatomy of the cusps is created by establishing the appropriate form of the posterior cusps aligned to the condylar path; thus it also contributes to posterior disclusion. Posterior disclusion is crucial in controlling harmful lateral forces but the factors that determine the precise amount of disclusion have not been established.10 As followed in this case twin stage procedure helps in achieving a standard disocclusion of 1 mm on protrusion, 1mm on non working side, and 0.5 mm on working side in centric movements at 3mm protrusion from centric relation.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also greatful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Kazis H. Complete mouth rehabilitation through restoration of lost vertical dimension. J Am Dent Assoc 1948; 37:19- 39.
2. Hausman M, Hobo S. Occlusal reconstruction using transitional crowns. J Prosthet Dent 1961; 11:278-87.
3. Braly BV. A preliminary wax-up as a diagnostic aid in occlusal rehabilitation. J Prosthet Dent 1966; 16:728-30.
4. Hobo S. A kinematic investigation of mandibular border movement by means of an electronic measuring system: Part II: A study of the Bennett movement. J Prosthet Dent 1984; 51:642-6.
5. Hobo S. A kinematic investigation of mandibular border movement by means of an electronic measuring system: Part III: Rotation centre of lateral movement. J Prosthet Dent 1984; 52:66-72.
6. Hobo S. Formula for adjusting the horizontal condylar path of the semiadjustable articulator with interocclusal records: Part I: Correlation between the immediate side shift, the progressive side shift, and the Bennett angle. J Prosthet Dent 1986; 55:422-6
7. Hobo S. Formula for adjusting the horizontal condylar path of the semiadjustable articulator with interocclusal records: Part II: Practical evaluations. J Prosthet Dent 1986; 55:582- 8
8. Binkley TK, Binkley CJ. A practical approach to full mouth rehabilitation. J Prosthet Dent 1987; 57:261-6.
9. Hobo S, Takayama H. Effect of canine guidance on the working condylar path. Int J Prosthodont 1989; 2:73-9
10. Hobo S. Twin-tables technique for occlusal rehabilitation: Part I: Mechanism of anterior guidance. J Prosthet Dent 1991; 66:299-303
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





