IJCRR - 4(6), March, 2012
Pages: 81-88
Print Article
Download XML Download PDF
CHANGES IN PHYSICAL PERFORMANCE AMONG HEALTHY PRE AND POST- MENOPAUSAL FEMALES - A CROSS SECTIONAL STUDY
Author: Bimali I, Narayan A
Category: Healthcare
Abstract:Purpose: To compare changes in physical performances (strength, flexibility and balance) between healthy Pre-Menopausal (40-45 years) and Post-Menopausal females (45-55 years) with natural history of menopause. Methods: Sixty pre and postmenopausal females were included. Strength was measured by hand held dynamometer, Flexibility with flexometer and Balance through postural sway. Results: Analysis of Variance (ANOVA), student paired t-test and Bonferroni test were used for the analysis. Level of significance < 0.05 was considered statistically significant with 95% CI. No significant difference was found for strength (p=0.081) and flexibility (p=0.116). But, loss of Balance (p=0.000) was found to be highly significant among the Post Menopausals. Conclusion: Lower limb muscles flexibility and upper limb strength did not show any significant changes among immediate Post Menopausal females; but static balance was significantly affected among the Post Menopausals causing diminished Physical Performance with age advancement.
Keywords: Balance, Flexibility, Menopause, Physical Performance, Strength.
Full Text:
INTRODUCTION
Menopause refers to the natural end of women years of having a regular monthly period, which also implies the end of her ability to get pregnant.1 It is a transition period characterized by physiological, psychosocial, and sociological changes that accompany the depletion of ovarian function.1-3 Acceleration in the loss of muscle mass and strength has been observed in women during Post Menopausal years.2-4 Although the underlying mechanism is still controversial, a growing body of evidence suggests that estrogen acts directly on the skeletal muscles through estrogen receptors in regulation of Physical Performance.5-7 Physical Performance is an ability to perform a physical task at a desired level.1 Muscular strength, Flexibility, and Balance are key components of Physical Performance. Poor Physical Performance predicts frailty, disability and loss of independence among elderly.1-3,8,9 Physical Performance is lower in women when compared to men and it increases with age beyond 55.4 This suggests that gender specific factors across life may influence maximum level of Physical Performance achieved and performance rate declines with age. One factor that has been implicated for this is ?Menopause‘. Decreased muscular strength has been proven to be the predictive of health deterioration in general; while limited flexibility and impaired balance are related to an increased risk of falls in older adults.4 Studies indicates that diminished muscular strength after menopause have a relation with hypoestrogenism. In a study, author had opined that ankle dorsiflexor torque plays important role to maintain static balance in the first years of menopause.7 The average Menopausal age of Indian female is 45 years and the western female is 51 years.10 Available literatures had analyzed the changes in Physical Performance due to menopause compared to Pre-Menopausal subjects.2,3,4 But subjects in these studies were of varying etiology of menopause i.e. hormonal therapy, hysterectomy, oophorocystectomy, natural ageing etc. and were in late menopausal age. Therefore this study aims to analyze the changes in Physical Performances due to natural menopause at an early age. The differences in Physical performance are analyzed by measuring the strength, flexibility and balance between Pre-Menopausal (40 – 45 yrs) and immediate Post-Menopausal females (45 – 55 yrs) with history of natural menopause.
MATERIALS AND METHODS
The subjects were selected randomly from Kasturba Medical college hospital and the local community around Mangalore city through the community screening camps. Among the 75 females participated for screening, 60 fulfilled the inclusion criteria and were included in the study. 15 subjects excluded through screening had osteoarthritic knee (OA), low back ache (LBA), vertigo, history of fall etc. A written informed consent was obtained after explaining the study procedure. Institutional ethical approval was obtained (IEC/KMC/03/2010–2011). The subjects were recruited in the study based on following inclusion and exclusion criteria:
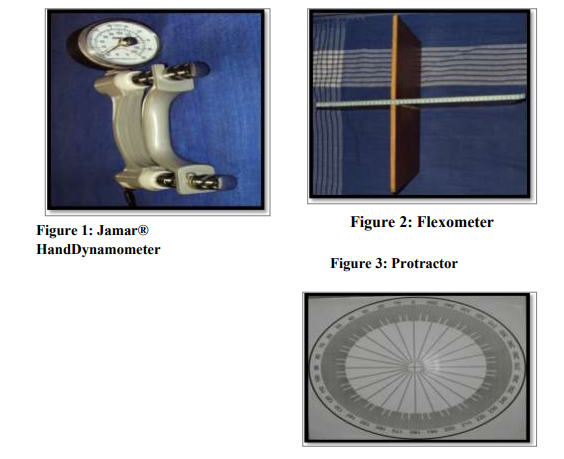
The outcome measures for physical performance were done for; a) Strength- by Jamar® Hand Dynamometer 1-3 ; ( refer figure:1) b) Flexibility- by Flexometer1,2,16 and, ( refer figure:2) c) Static balance- analyzed through time taken (in seconds) for the appearance of postural sway (1st and 2nd sway) using protractor with eyes open/closed for Left/Right legs individually (refer figure: 3). Data was documented for each of the outcome measures.
Testing Procedure
The testing procedure adopted for each outcome measures are as follows;
Strength: Subjects were made to sit on a chair with arms at right angle and elbow by the side of the body with forearm supported. Jamar® Hand Dynamometer 1-3 was held in the dominant hand and directions given to squeeze the Dynamometer with the maximum isometric effort and maintain the same for about 5 seconds.
Flexibility: Subjects were asked to keep the back and head against a wall with the legs straight ahead and knees flat against the floor (i.e. long sitting). Then, a flexometer was placed against the subjects‘ feet. While keeping the back straight, subjects were asked to stretch their arms out towards the box. Subjects were instructed not to jerk or bounce to reach further and hold the full reach position for two seconds, and score (i.e. reach distance) was recorded.
Balance:
Protractor drawn on a flex paper was placed on the wall and subjects were asked to stand in front of it without shoes. Axis of the protractor was aligned along the vertex of subject‘s head. Then subjects were made to stand on right and left leg alternately with arms across their chest and hands touching the shoulders. They were asked to look straight ahead with the eyes open and focus on an object about 3 feet in front. The therapist stood in front of the subject at 5 feet distance. Tests were terminated when the leg touched the floor, or the arms moved from their start position or when the subject swayed more than 15? . Reading (in seconds) was taken on first sway and then on 15? sway.
Data analysis
Statistical Package for Social Science (SPSS) version 13.0 used for the statistical analysis. The level of significance < 0.05 was considered to be statistically significant with 95% confidence interval. Analysis of Variance (ANOVA) and student paired t-test were used to compare the values between the two groups. Bonferroni test was used for the multiple analyses of the Sways.
RESULTS
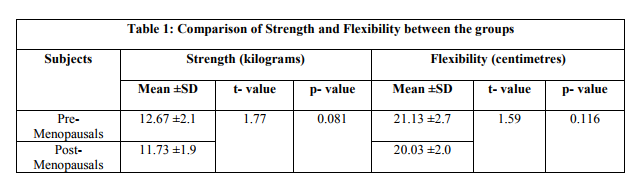
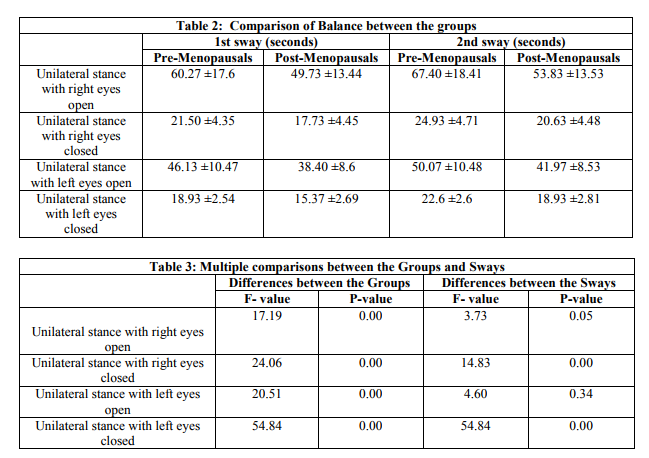
In this study, 60 female subjects participated from Dakshina Kannada district of Karnataka state. Participated subjects mean age was 42.13 ±1.73 years for Pre-Menopausals (n= 30) and 52.10 ±2.02 years for Post-Menopausals (n= 30). I. Hand Grip Strength (refer table: 1) In the Pre-Menopause groups the mean strength was 12.67 ±2.0 kilograms and for Post-Menopause groups the same was 11.73 ±1.9 kilograms having p value of 0.081. It suggests similarities in hand grip strength between the pre- and postmenopausal subjects. II. Flexibility (refer table: 1) The mean flexibility range for Pre and Post menopause groups were 21.13 ±2.7 and 20.03 ±2.0 centimeters respectively with p value of 0.116. It shows that flexibility differences between the two groups were not significant, suggesting that both groups carry similar flexibility ranges. III. Balance (refer table: 2,3) a. Unilateral Right Leg Stance with Eyes Open and Closed: In Pre Menopause group the mean unilateral 1 st sway with eyes open was observed at 60.27 ±17.6 seconds and for 2 nd sway at 67.40 ±18.41. While with eyes closed the 1 st sway was seen at 21.50 ±4.35 and 2 nd sway at 24.93 ±4.7 seconds. But among the Post-Menopausals, the mean unilateral 1 st sway with eyes open occurred at 49.73 ±13.44 seconds and 2nd sway at 53.83 ±13.53. With eyes closed the 1 st sway was at 17.73 ±4.45 and 2 nd sway occurred at 20.63 ±4.48 seconds. The results indicates that differences in 1 st and 2 nd sways between the two groups (p=0.00) were highly significant. But, differences were non-significant between the two sways within both the groups with eyes open, while highly significant differences were found between the 1 st and 2 nd sway (p=0.00) within the groups with eyes closed.
b. Unilateral Left Leg Stance with Eyes Open and Closed:
Among Pre Menopausals with eyes open the 1st and 2nd sway occurred at 46.13 ±10.47 and 50.07 ±10.48 seconds respectively; but for Post-Menopausals the mean unilateral 1 st sway were seen at 38.40 ±8.6 and 2 nd sway at 41.97 ±8.53 seconds. With eyes closed 1st sway occurred at 18.93 ±2.54 seconds and 2 nd sway at 22.6 ±2.6 among the Pre-Menopausals; but 1 st sway was seen at 15.37 ±2.69 and 2 nd sway at 18.93 ±2.81 seconds in the PostMenopausals. The result shows highly significant differences in1st and 2nd sways between the two groups (p=0.00) and also within the group (p=0.00). Multiple comparisons between the groups also demonstrated significant differences for the 1st sway; and highly significant for the 2nd sway. Between the two groups, results demonstrated highly significant differences (p=0.00) between 1st and 2nd sways.
DISCUSSION
The findings of this study suggest that balance ability, but not the Hand Grip Strength and flexibility is affected among early Post-Menopausals; as the Hand Grip Strength and Flexibility were almost similar between the two groups. This could be because of narrow age differences among the subjects. Since reduction in muscle strength/flexibility secondary to aging occurs rapidly after 65 years of age (i.e. especially of lower limb muscles12,13,19 ) and accelerated drop in muscle strength of hand grip muscles occurs after 55 years age.4 But static balance was reduced significantly among the Post-Menopausals. The most optimal reason for this outcome can be attributed to the three strategies adopted by an individual to maintain the upright posture and to recover the balance: hip, ankle, and stepping strategy. One rely on ankle strategy when displacements are in small ranges within the limit of stability.21 But when oscillations are more and frequency is high, or when the supporting weight bearing surface is small than the foot area; then one shifts to encompass the hip strategy in order to maintain the balance. Also, if the body perturbation is greater, than more people tend to decrease the ankle response leading to increase in hip strategies. In such situation postural sways increases automatically. This condition probably would have been the reason among PostMenopausal females that would have facilitated the activation of other muscular groups to maintain the body posture.15,22 Muscles closest to the base of support are particularly important to maintain the balance. In a study correlation were reported between the static balance and the ankle dorsiflexor strength among PostMenopausal females, and suggestions were made about the importance of ankle dorsiflexors strength in maintaining the balance.20 Therefore, decrease in balance leading to the appearance of early sway among Post-Menopausal females. Other reason could be the age related decline in muscle strength of lower limb that would have lead to the occurrence of second sway faster than the first sway among the PostMenopausal females.14 But, since in this study we analysed only the upper limb strength (i.e. Hand Grip strength) and not the lower limb; therefore, this observation cannot be conclusively justified. The sharp increase in the incidence of falls due to loss of balance in women around the time of menopause has been attributed to the menopause-related reductions in serum estradiol level (component of estrogen hormone).20 This study found improvement in postural sway after hormonal therapy among Post-Menopausal females20 indicating that reduction of estrogen hormone would cause increase in postural sway among such subjects. Thus the findings of our study indicate that Balance, but not flexibility and strength, deteriorate during the transition through natural menopause. Since compromised Physical Performance can have substantial impact on the quality of life, which is inevitable with increased life expectancy; therefore, one need to be free of illness in order to function efficiently and effectively in old age. The findings also suggest that Hand Grip Strength and Muscle flexibility may not directly impact the balance quality. So, as healthcare professional we need to develop appropriate preventive measures to improve the balance among early Post-Menopausal females. The limitations of this study was the nonconsideration of the trunk and lower limb muscle strength and flexibility of the muscles anterior to the hip joints, since these muscles plays major role in maintaining the posture and balance. Based on the study findings, we opined that future research should involve trunk and lower limb muscle strength and flexibility as they play important role for posture in general and balance in particular.14 Also one can apply Posturography23 to assess the dynamic balance with focus on various functional life style situations.
ACKNOWLEDGEMENT
The authors would like to acknowledge all the females who participated in this study, Chetana Child development Center and Lions Club, Mangalore. We are also grateful to the authors‘ /editors /publishers of all the articles that have been used as a reference for this study.
References:
1. Cheng HM, Wang SH, Yang FY, Wang HP, Fuh LJ. Menopause and Physical performance. Menopause 2009;16:892-96.
2. Cooper R, Mishra G, Clennell S, Guralnik J, Kuh D. Menopause status and physical performance in midlife: findings from british birth cohort study. Menopause 2008;15:1079-85.
3. Sowers M, Tomey K, Jannausch M, Eyvazzadeh A, Nan B, Randolph J. Physical functioning and menopausal states. Obstet Gynecol 2007;110:1290- 96.
4. Samson M. et al. Relationships between physical performance measures, age, height and body weight in healthy adults. Age and Ageing 2000;29:235- 42.
5. Speroff L, Fritz M. Clinical Gynaecologic Endocinology and Infertility. 7 th ed. Lippincott Williams and Wilkins; 2005. p. 621-88.
6. Berek SJ. Gynecology. 14th ed. Lippincott and Wilkins; 2007. p. 1323- 42.
7. Pinto NS et al. Postmenopausal/menopause, bone mineral density and whole body vibration: a short review. Journal of Medicine and Medical Sciences 2010;1:516-25.
8. Owers MF, Pope S, Welch G, Sternfeld B, Albrecht G. The association of menopause and physical functioning in women at midlife. JAGS 2001;49:1485-92.
9. Cesar ADS, Santos, Samaria A, Cader, Estelio HM, Dantas, Maria HR, Moreira. Physical fitness of postmenopausal women submitted to a physical activities programme. Biomedical Human Kinetics 2010;2:93-96.
10. Bharadwaj JA, Kendurkar SM, Vaidya PR. Age and symptomatlogy of menopause in Indian women. Journal of post graduate medicine 1983;29:218-22.
11. Armstrong L.et al. ACSM‘s guidelines for exercise testing and prescription. 7 th ed. Lippincott Williams and Wilkins; 2006. p. 55-89.
12. Greeves JP, Cable NT, Reilly T, Kingsland C. Changes in muscle strength in women following the menopause: a longitudinal assessment of the efficacy of hormone replacement therapy. Clinical Science 1999;97:79– 84.
13. Kurina LM et al. The effect of menopause on grip and pinch strength: Results from the chicago, Illinois, site of the study of Womens health across the nation. American Journal of Epidemiology 2004;160:484-91.
14. Gustavo DLD et al. Static balance, quadriceps strength and ankle dorsiflexor torque in fertile and postmenopausal women. Fisioter Mov 2010;23:585-91.
15. Fu S, Choy NL, Nitz J. Controlling balance decline across the menopause using a balance-strategy training program: a randomized, controlled trial. Climacteric 2009;12:165-76.
16. Wells KF and Dillon EK. The sit and reach. A test of back and leg flexibility. Research Quarterly 1952;23:115-18.
17. Springer B. et al. Normative values for the unipedal stance test with eyes open and closed. Journal of Geriatric Physical therapy 2007;30:8-14.
18. Umphered D. Neurological Rehabilitation. 5 th ed. Mosby; 2007. p. 739, 879.
19. Ozgocmen S, Karaoglan B, Cimen OB, Yorgancioglu ZR. Relation between Grip Strength and Hand Bone Mineral Density in Healthy Women Aged 30- 70. Singapore Med J 2000;40:268-70.
20. Ekblad S, Lonnberg B, Berg G, Odkvist L, Ledin T, Hammar M. Estrogen effects on postural balance in postmenopausal women without vasomotor symptoms: a randomized masked trial. Obstet Gynecol 2000;95:278-83.
21. Callisaya ML et al. A population-based study of sensorimotor factors affecting gait in older people. Age and Ageing 2009;38:290–95.
22. Park S, Horak FB, Kuo AD. Postural feedback responses scale with biomechanical constraints in human standing. Exp Brain Res 2004;154:417- 27.
23. Zammit G, Sherry WW, Peng X. Use of computerized dynamic posturography to assess balance in older adults after nighttime awakenings using zolpidem as a reference. BMC Geriatrics 2008;8- 15
24. Hunter SK, Thompson MW, Adams R. Relationships among Age- Associated strength changes and physical activity level, limb dominance, and muscle group in women. The journal of gerontology: Biological Sciences 2000;55:264-73.
25. Pradhan GP, Srivastava SK. Menopause and Other Correlates. Indian J. Prev. Soc. Med. 2003;34:1-2.
26. Sirola J, Rikkonen T. Muscle performance after the menopause. Menopause Int 2005;1:45-50 27. Guccione AA. Geriatric Physical Therapy. 2 nd edition, Mosby; 2000. p. 265-80
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





