IJCRR - 5(1), January, 2013
Pages: 95-99
Print Article
Download XML Download PDF
CAFFEY'S DISEASE - A DIAGNOSTIC DILEMMA
Author: Soundarya Mahalingam, Kamalakshi Bhat, Gopakumar, Basavaprabhu Achappa
Category: Healthcare
Abstract:Fever in infancy can imply a wide spectrum of illnesses that range from an innocuous upper respiratory infection to life threatening systemic infection. Hence fever without a focus in an infant has been, is and will be a diagnostic dilemma for the paediatrician. Here we present a case who presented similarly with fever without focus, however the cause finally elucidated was the rare Caffey's disease. Caffey's disease is a rare disorder whose etiology is yet to be clearly elucidated. It is characterised by cortical hyperostosis with inflammation of adjacent fascia and at times the overlying muscle is also involved. It most often presents in infancy with sudden irritability, soft tissue swelling visible over the involved bones having a woody induration with no suppuration, fever and anorexia. The disease is also known to have an unpredictable course with remissions and relapses. A high index of suspicion with a good radiology and laboratory backup is thus necessary to make a diagnosis and plan treatment.
Keywords: Caffey’s disease; Fever; Infantile Cortical Hyperostosis
Full Text:
CASE REPORT
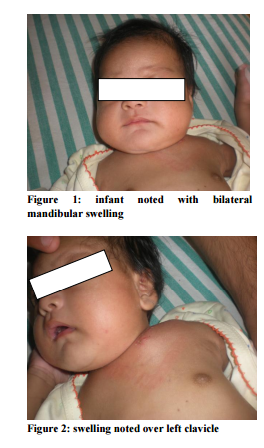
A 56 day old male baby, born to nonconsanguineous parents was referred with low grade continuous fever of ten days duration, and minimal upper respiratory infection with nasal block since the last two days. He was treated elsewhere with oral and parenteral antibiotics for eight days and referred to us for persistence of fever. He was immunised to date and was on breast feeds and top feeds. On examination, he was irritable, had significant pallor, short neck, with diffuse swelling in mandibular and sub mandibular regions bilaterally and no obvious facial dysmorphism. He was febrile (102 degree F), tachycardic ( 158 / min) and tachypnoeic (62/ min).
His anthropometric measurements were appropriate for age. On auscultation, a short systolic murmur was heard at the apex. Liver was enlarged 3cm below Rt. costal margin. Initial blood investigations revealed anemia (Hb – 8.1g %), neutrophilic leucocytosis (TLC 34, 480 cells/cu. mm with 72 % neutrophils, 5% band forms) and thrombocytosis (12, 07,000 cells/cu. mm). CRP was elevated (84 mg/L). Liver function tests, renal function tests and serum electrolytes were normal. Malarial test was negative. Urine and stool routine was normal and urine and Blood culture and sensitivity also yielded no growth. Our initial diagnosis was sepsis with anemia in congestive cardiac failure, hence he was started on intravenous piperacillin / tazobactam and packed RBCs were transfused.
After 48 hrs of admission, the fever was still present, CRP was further elevated (236 mg / L), hence ECHO was done to rule out infective endocarditis, which was normal. During these two days he was noticed to have severe nasal block and assumed a hyperextended neck posture hence CT scan head-neck and lumbar puncture were done, which were normal except for few enlarged cervical lymph nodes. Nasal secretion from suction catheter was sent for culture and sensitivity which grew Staphyloccus aureus and Escherichia coli, hence antibiotics were changed appropriately. On the 7th day of admission, he continued to have fever and developed paucity of movement of left arm with swelling and tenderness over the left clavicular region. X ray and USG of local area over clavicle showed cortical irregularity and adjacent periosteal thickening and osteomyelitis could not be ruled out, hence anti-inflammatory drugs were started and antibiotics continued.
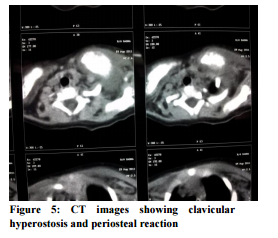
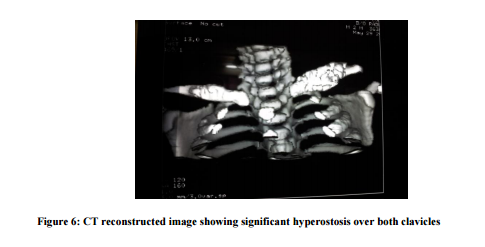
There was gradual symptomatic improvement and the baby became less irritable and started moving the limb. Repeat investigations showed total count (26,850 cells/cu. mm), platelet count (7,73, 000 cells/cu.mm),elevated ALP (843IU/L) and ESR (65mm/ hr). Over the next few days in hospital, a similar swelling over the right clavicular region and fever persisted. CT scan of bilateral clavicular region was done that showed B/L clavicular periosteitis with adjacent soft tissue inflammation. In search for the etiology the following tests were ordered - VDRL (Negative), serum ferritin (698ng/ml), IgM CMV (negative), HIV (negative), Central line culture (sterile), all of which were normal. Immunoglobulin profile showed elevated IgE – 475 IU/mL and IgM 1.05 IU/mL with normal IgA and IgG levels. In view of persisting fever with increasing clavicular inflammation despite appropriate antibiotic treatment, bone biopsy was done by orthopaedic surgeon which revealed periosteal inflammation composed of neutrophils, eosinophils, occasional focal lymphoplasmacytic infiltrates with fibrosis and hyperostosis.
On review of literature, these clinical findings along with anemia, thrombocytosis, elevated inflammatory markers, the typical imaging studies and biopsy were found to be consistent with the diagnosis of Caffey’s Disease. In the following days of hospital stay, on antiinflammatory measures, baby became symptomatically better with no fever, less irritability, weight gain, hand movements improved, though the swelling over the clavicles remained. At discharge, investigations showed Hb – 10.7 gm%, total count – 14,500 cells / cu mm, DC - N34 L55 E2 M9, platelet count – 1, 70,000 cells / cu mm.
On follow up visits, baby has normal development with good weight gain and there was no evident clavicular or mandibular swelling. Hematological parameters had improved with normal haemoglobin, platelet count and decreasing ESR. He is one year old now and has not had recurrence of symptoms.
DISCUSSION Fever in infancy has always been a diagnostic dilemma, more so when there are no localising signs at the outset. Caffey’s disease is one such situation wherein the search for the diagnosis can mislead without a good clinical suspicion and multidisciplinary approach to the diagnosis. It was first reported as a disease entity by Caffey and Silverman in 1945 and is also known as Infantile Cortical Hyperostosis. It is a self limiting disorder characterized by a triad of systemic symptoms like irritability, fever, soft tissue swelling and underlying cortical bone thickening. The exact aetiology of this condition is still unknown [1].
Most cases are sporadic, but a few familial cases with autosomal dominant and recessive patterns have been described [2]. The existence of two forms of Caffey disease has been suggested, a classical mild infantile form delineated by Caffey and Silverman and a severe form with prenatal onset [1,3,4,5]. The classic form has an onset within the first 6 months of life, usually with symptoms of irritability, swelling of the overlying soft tissue that precedes the cortical thickening of the underlying bones, fever and anorexia. The swelling is painful with induration but with no redness or warmth, thus suppuration is absent. Mandible is the most commonly involved site followed by scapula, clavicle, ribs and long bones. There are usually no other signs and symptoms.
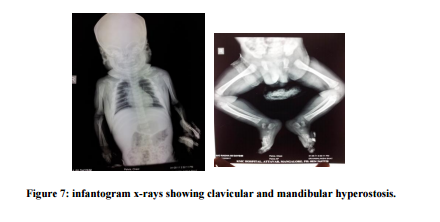
Isolated cases of facial nerve palsy and Erb’s palsy following nerve entrapment have been reported in the literature [6, 7]. The pain can be severe and can also result in pseudo paralysis. Laboratory findings include elevated ESR, and in some patients high alkaline phosphatase, thrombocytosis, anaemia and raised immunoglobulin levels [8]. Radiography is the most valuable diagnostic study in ICH. Cortical new bone formation (Cortical Hyperostosis) beneath the regions of soft tissue swelling is the characteristic feature. While no laboratory tests are specific, the important differential diagnosis that are to be excluded are osteomyelitis, chronic hypervitaminosis A, bone tumour, scurvy, child abuse and prolonged PGE1 infusion [9,10].
Complications have been seen with usually the severe prenatal disease, include pseudoparalysis, torticollis, pleural effusions, mandibular asymmetry and bony fusions when adjacent flat bones are involved. Caffey disease is mostly self-limiting and resolves within six months to one year and may not need any treatment [4]. However, Indomethacin or Naproxen could be used in really symptomatic cases. Steroids (prednisolone) can be administered if there is poor response to Indomethacin, and in cases without thrombocytosis [9].
CONCLUSION Caffey’s disease, though a rare and self limiting condition, may mimic common childhood illnesses. The disease may present, as in our case, with only fever and evolve over the following days with the typical features of fever, soft tissue swelling and irritability. Awareness of this condition, a good history, clinical examination, basic laboratory studies and plain radiographs are sufficient for diagnosis in most cases. Counselling the parents is important as this disease is known to relapse and remit throughout childhood and complications can occur if the disease stays untreated.
ACKNOWLEDGEMENTS Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Restrepo S, Sánchez AM, Palacios E. Infantile cortical hyperostosis of the mandible. Ear Nose Throat J 2004 Jul; 83(7):454-455.
2. Bernstein RM, Zaleska DJ. Familial Aspects of Caffey Disease. Am J Orthop 1996; 24:777-778.
3. Susan S, Rabih C, Comelia T, Katharina L, Stephan M, Sigrid T. Antenatal onset of cortical hyperostosis. Am J Med Genet 2003; 120:547-552.
4. Mohammed ALF. Caffey Silverman Disease: Case Report and Literature Review. Kuwait Medical journal 2006; 38(1):49-52.
5. Harris VJ, Ramilo J. Caffey’s disease: a case originating in the first metatarsal and review of a 12 year experience. Am J Roentgenol 1978 Feb;130(2):335-337
6. Challapalli M, Cunningham DG, Varnado SC. Infantile cortical hyperostosis and facial nerve palsy. Int J Pediatr Otorhinolaryngol 1998 Mar; 43(2):175-178.
7. Holtzman D. Infantile cortical hyperostosis of the scapula presenting as an ipsilateral Erb’s palsy. J Pediatr 1972 Oct; 81(4):785-788.
8. Kumar TS, Scott JX, Mathew LG. Caffey disease with raised immunoglobulin levels and thrombocytosis. Indian J Pediatr 2008 Feb; 75(2):181-182.
9. Varma R, Johny VF. Infantile cortical hyperostosis. Indian Pediatr 2002 Nov; 39(11):1057.
10. Almada Rodriguez Hugo D. Non accidental injuries in Children-common pit falls Online ISSN: 0972-8074, published on 2005 July 1, accessed on 4th April 2009.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





