IJCRR - 5(1), January, 2013
Pages: 32-35
Print Article
Download XML Download PDF
DONOR PROFILE AND BLOOD SAFETY: COMPARISON BETWEEN FIXED (INSTITUTE) AND MOBILE SITE (CAMP) BLOOD COLLECTIONS
Author: B.Abhishekh, K.C.Usha
Category: Healthcare
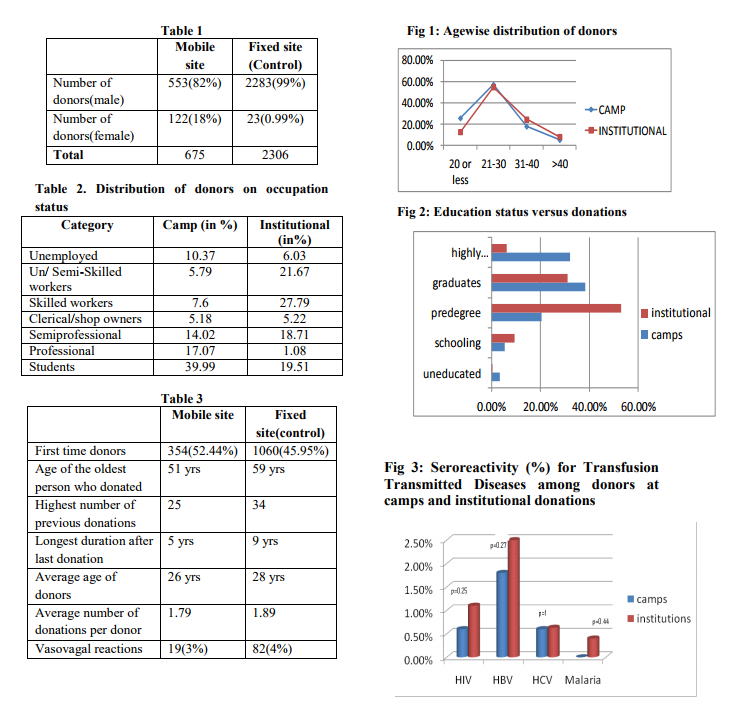
Abstract:Background: The importance of blood safety in public health was recognized long ago and data are essential to plan strategies to improve its status. Ability to ensure an adequate blood supply depends on knowing and understanding donor demographics and characteristics and their impact on collections. Objectives: To explore and compare the demographic profile and seropositivity among donors donating whole blood at fixed and mobile donation sites. Methods: The information of all the donors registered and donated blood was collected from the donor registration forms. Serological results of the donors were obtained from the Transfusion Transmitted Disease Screening division of the department. Data were entered into Microsoft excel sheet and results analyzed on SPSS software version 10. Results: In fixed site female donors contributed for about 1% of donations while at the mobile site their participation attributed to 18% of donations. Seropositivity was slightly higher among donors at fixed site (HBV-2.5%, HIV-1.1%) when compared to donors at the mobile site (HBV-1.8%, HIV-0.6%). The vasovagal reactions among donors were around 4% in fixed site and around 3% at mobile sites.
Keywords: fixed site, mobile site, donor profile
Full Text:
INTRODUCTION
Fixed site is a widely used term for a permanent or freestanding blood collection center. The fixed site may be located in a hospital based donor room or in a community blood center building. In mobile blood drives the donor room is essentially transported to the donor. The mobile blood collection team generally arranges mobile blood drives with a sponsoring organization often a business, school, hospital, public service organization, trusts, NGO’s, religious group, or military installation etc. It is generally easier and more cost effective to run a fixed site1, 2. The convenience of a mobile drive brings in new and voluntary donors into donor pool. Mobile blood drives should be set up along the same basic principles as fixed sites, although a certain amount of flexibility is often in order in terms of cleanliness, ventilation, space, temperature, privacy to discuss the many personal questions on the donor-screening questionnaire etc3, 4 . Ability to ensure an adequate blood supply depends on knowing and understanding donor demographics and characteristics and their impact on collections5 . Aim: This study was aimed to explore and compare the demographic profile and seropositivity among donors donating whole blood at fixed and mobile donation sites.
RESEARCH METHODOLOGY This was a cross sectional study with the study setting being the department of transfusion medicine of Trivandrum Medical College which is a major referral and tertiary care centre of south Kerala. Camps are conducted regularly every week in and around Trivandrum in both urban and rural areas within 60 km from the college collecting on average 30-50 whole blood donations. The information like age, sex, education status, occupation, donation status(first time/repeat) of all the donors registered and donated blood at various camps conducted during the year 2009 were collected from the donor registration forms. All the donors who registered and donated blood at the department on the same day of the camps were included as comparison group. At the department the whole blood collection ranges 80-120. The donors from the camps wherein the venue was college premises were excluded to avoid homogeneity among the study population. Serological results of the donors were obtained from the TTD Screening division of the department. The tests used were antibody detection ELISA for HIV (double sandwich 3rd generation anti HIV 1 / 2) and HCV (3rd generation anti Hep C virus), HBsAg detecting solid phase micro plate direct sandwich ELISA for HBV, single step rapid immunochromatographic test for detection of P. Falciparum, P.Vivax antigens for malaria and non Treponemal macro agglutinin rapid slide method for Syphilis reagin antibodies in serum. Data were entered into Microsoft excel sheet and results analyzed on SPSS software version 10.
DEFINITIONS6 Voluntary Blood Donor: A voluntary blood donor donates blood out of his/her free will without expecting anything of monetary value from the blood bank or patients” relatives or any other source at the time of donation or in future.
Replacement Blood Donor: Replacement blood donor is a member of the family (familial) or a friend of the patient who donates blood in replacement of blood needed for the particular patient without involvement of any monetary or other benefits from any source. Directed Donation: When blood is donated by a relative (donor) for a particular patient.
RESULTS In fixed site female donors contributed for about 1% of donations while at the mobile site their participation attributed to 18% of donations (p<0.001). It was seen that highly qualified7 and official class preferred to donate at their doorstep/work environment rather than at the hospitals as shown in Fig 2 and Table 2. Seropositivity was slightly higher among donors at fixed site (HBV-2.5%, HIV-1.1%) when compared to donors at the mobile site (HBV- 1.8%, HIV-0.6%).HCV had an equal prevalence (0.6%) in collections at both the sites. Malaria was not comparable as the prevalence was very low (~<0.1%).There was no positive results for syphilis in either group. The vasovagal reactions among donors were around 4% in fixed site and around 3% at mobile sites (p=0.35).
DISCUSSION Results suggest that recruitment efforts for a given centre require detailed understanding of patterns of participation and identifying areas of focus to maximize voluntary donations. There are selected similarities and wide variability in the characteristics of donors at different donation sites (fixed and mobile). Fixed sites are generally less convenient for donors as they need additional travel and time. This is shown by the fact that significant donation by the professionals and highly qualified people when the donation was at their place that these people don’t regularly donate due to the inconvenience and time off work to reach the donation site at an institution. This was much more significant with female donors as their response was overwhelming at camps compared to the fixed site.
Mobile blood drives are ultimate in convenience for donors. It brings many otherwise ‘unavailable’ blood donors into the system. Once mobile site donors have had a positive and successful blood donation experience, it is often possible to bring them to a fixed site for further donations with effective and continuous recruitment techniques8,9. Camps were also helpful in bringing the lost donors who had stopped donating due to some or the other reason as evidenced by average number of donations per donor and the gap between two subsequent donations. Average age of donors at the camps was slightly less (26yrs) than at the institute (28yrs) which probably points to the fact that the camps are helpful in catching the attention of young donors as well as the first time donors (53%) as compared to institute (45%). Study also threw light on the point that the site of donation did not bother much to the regular donors.
There was not much to choose between the donor reactions at these sites though there is lot of speculation that the vasovagal reactions occur at an increased frequency at camps due to improper ventilation and non conducible environment. The effect may also be nullified by the fact the hospital premises adds to anxiety among lot of donors. It can also be added that donors available in hospital premises which includes lot of patient’s bystanders, family and friends who would be stressed or emotionally disturbed whereas the general population who donated at camps would be slightly in better health. There are also few opinions among researchers that the blood donations at camps have a slightly more seropositivity to Transfusion Transmitted Diseases as the criteria’s for donor selection are less stringent there either due to pressure from organizers or the enthusiastic donors. But our study showed a slightly more seroreactivity among institutional donations with respect to HIV and HBV. This could be due to a fraction of familial or replacement donors at the institute which could be a notable drawback of the study.
CONCLUSIONS There are selected similarities and wide variability in the characteristics of donors at different donation sites (fixed and mobile). Results suggest that recruitment efforts for a given centre require detailed understanding of patterns of participation and identifying areas of focus to maximize voluntary donations.
References:
1. Graeme Woodfield; Road blocks in achieving 100% voluntary blood donation rate in the south Asian region; AJTS 2007 vol 1 issue 1 pg 33-38
2. Hillyer; Blood collection sites: Fixed and Mobile; Blood banking and Transfusion Medicine basic principles and Practice 2nd edn page 157-79
3. Patricia M. Carey, Patrick M. High Et al Donation return time at fixed and mobile donation sites. Transfusion 2012; 52:127-33.
4. C. T. Tagny, S. Owusu-Ofori, D. Mbanya and V. Deneys.The blood donor in sub-Saharan Africa: a review. Transfusion Medicine, 2010, 20, 1–10
5. Code of Federal Regulations. 21 CFR 606.40. Washington, D.C., U.S. Government Printing Office, April 1, 2005.
6. National Guidebook on Blood Donor Motivation. Ministry of Health and Family Welfare. 2nd ed. Government of India: 2003.
7. Kuppuswamy B. Manual of socioeconomic status (Urban), Manasayan, Delhi, 1981.
8. Ownby HE, Kong F, Watanabe K, Tu Y, Nass CC. Analysis of donor return behavior. Transfusion 1999; 39:1128-35.
9. Nguyen DD, Devita DA, Hirschler NV, Murphy EL. Blood donor satisfaction and intention of future donation. Transfusion 2008; 48:742-8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





