IJCRR - 5(2), January, 2013
Pages: 42-44
Print Article
Download XML Download PDF
UNUSUAL FINDING OF CYSTIC CHANGES IN HASHIMOTO'S THYROIDITIS: A REPORT
Author: Ashwini B.R., Sunita Vernekar, Rajeshwari Bhuttannavar
Category: Healthcare
Abstract:Hashimoto's thyroiditis(HT) is a chronic autoimmune thyroiditis affecting women more commonly. It is characterized by lymphoplasmacytic infiltration of thyroid follicular cells, hurthle cells resulting in atrophy of the follicular cells and fibrosis. Cystic change is an unusual finding in Hashimoto's thyroiditis. A 35 year old female presented as nodular goiter clinically with ultrasound showing multiple cystic areas. Histopathological examination of the specimen after thyroidectomy showed features of Hashimoto's thyroiditis with cystic areas. We report a rare case of Hashimoto's thyroiditis with cystic changes in for the first time to the best of our knowledge. A more detailed study in this regard is warranted to understand the pathogenesis of cystic changes in HT.
Keywords: Hashimoto’s thyroiditis, cystic changes
Full Text:
INTRODUCTION
Hashimoto’s thyroiditis (HT) is an autoimmune disorder, characterized histologically by lymphoplasmacytic infiltration of thyroid follicular cells, hurthle cells resulting in fibrosis and atrophy of the cells. Cystic changes are an unusual finding in HT. We report the first case of HT with cystic changes.
CASE REPORT
A 35 year old female patient presented to our hospital with history of swelling in front of the neck from 2 years. Swelling was gradually increasing in size. There were no symptoms of hypothyroidism or hyperthyroidism in the patient. On examination there was a firm swelling with nodular surface measuring 9x6 cms. Patients pulse rate was 80/min, and BP was 120/82 mm of Hg. A clinical diagnosis of nodular goiter was made. Ultrasound showed enlargement of both lobes with multiple cystic areas with thick internal contents. Fine needle aspiration cytology of thyroid showed follicular cells in clusters, Hurthle cells with scant lymphocytic infiltration in the background of thin colloid. Diagnosis of nodular goiter was made. Thyroid function tests showed T3 162.8ngm/dl, T4 8.7µgms/dl and TSH 2.4 µIU/dl. Subtotal thyroidectomy was done. Post operatively the thyroid specimen was sent to the department of pathology. The specimen consisted of both lobes of thyroid with isthmus and was nodular. Cut section was gray white with lobular and cystic areas as in Figure 1. Histopathology showed dense lymphocytic infiltration with destruction of follicular cells. Hurthle cells, cystic areas with colloid and cyst macrophages were also seen. The cystic spaces did not have any lining epithelium as in figure 2. Immunohistochemistry showed polymorphous population of lymphocytes surrounding the follicular cells.
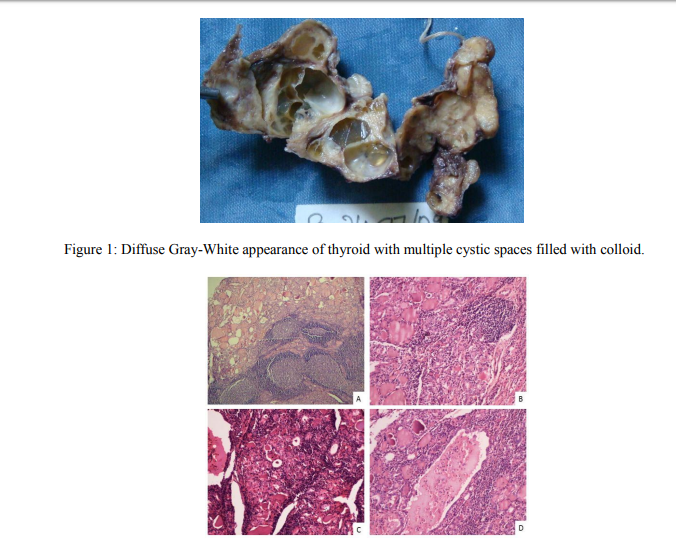
Figure 2: [A]- Thyroid follicles with dense lymphocytic infiltration and germinal center formation (4x). [B]- Lymphoplasmacytic infiltration with destruction of the follicles (10x). [C]- Hurthle cells with atrophic follicles with cystic space in the left upper corner (40x). [D]- Cystic spaces showing cyst macrophages and colloid with no lining epithelium (40x). Diagnosis of Hashimoto’s thyroiditis with cystic changes was made. Post-operative evaluation of the patient showed seropositivity for antithyroglobulin antibodies.
DISCUSSION
Lymphoplasmacytic infiltration of follicular cells causes atrophy of the cells with fibrosis and sclerosis. Autoimmune B and T lymphocytes along with reactive intermediates induce apoptosis and also damage the thyrocyte cell membrane causing thyrocyte necrosis1 . Cystic changes occurs in nodular goiter is due to vascular compromise, ischemia and necrosis. Cystic change can be seen in HT associated with secondary pathology like papillary carcinoma and malignant lymphoma. Matsuzuka et al reported a case of HT who developed small cyst like pattern on serial ultrasound2 . Histopathology showed features of malignant lymphoma with HT. Mitteldoff et al reported a case, seropositive for Human immunodeficiency virus (HIV) showing bilateral complex cysts with high titers of antimicrosomal antibodies. Cysts showed heterogenous
lymphocytic population and occasional groups of immature squamous cells with cytological features of autoimmune thyroiditis3 . True cysts lined by squamous epithelium, bordered by a row of lymphoid follicles in thyroid is been reported by Louis et al4 . Our case was sero-negative for HIV and the cystic spaces had no lining epithelium.
CONCLUSION
Cystic changes in HT are of rare occurrence. The lymphocytic infiltration in HT induces fibrosis rather than cystic degeneration. A case with cystic changes in HT being reported for the first time to the best of our knowledge.
RECOMMENDATIONS
A more detailed study in this regard is warranted to understand the pathogenesis of cystic change in HT.
ACKNOWLEDGEMENT
The authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. DECLARATION ON CONFLICT OF INTEREST: Nil
References:
1. Dimitry A Chistiakov. Immunogenetics of Hashimoto’s thyroiditis. Journal of Autoimmune Diseases 2005;2:1
2. FurmioMatzuzuka, Nobuyuki Amino, Kanji Kuma, Akira Miyauchi. Serial changes in thyroid ultrasonogram in a patient with Hashomoto’s thyroiditis who developed malignant lymphoma. Thyroid 2005;15(7):742- 43
3. Cristina A.T.S Mitteldorf, Antonio Carlos de OliveriaMisiara, Iara Emiko de Carvalho. Multicystic Autoimmune thyroiditis-like disease associated with HIV infection a case report. Acta cytol 1999;43:862-66
4. Multiple Branchial cleft like cysts in Hashimoto’s thyroiditis. American journal of surgi Pathol 1989;13(1)
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





