IJCRR - 5(15), August, 2013
Pages: 23-30
Date of Publication: 17-Aug-2013
Print Article
Download XML Download PDF
EVALUATION OF ANATOMIC VARIATIONS IN CORONARY ARTERY ON 64-SLICE COMPUTED TOMOGRAPHY ANGIOGRAPHY (CTA)
Author: Ritu Mehta, Sanjeev Agarwal
Category: Healthcare
Abstract:Objective: We retrospectively evaluated anatomic variants and anomalies of coronary arteries and found their incidence in 106 patients with the help of the 64-slice Computed Tomography Angiography (CTA). Materials and Methods: CT data of 106 patients who underwent 64-slice CT angiography (CTA) because of screening or suspected coronary artery disease were retrospectively reviewed in Department of Radiology, Geetanjali Medical College and Hospital, Udaipur. In each case, anatomic variants and anomalies were investigated. Results: The coronary artery system was right dominant in 85%, left dominant in 12% and co-dominant in 2.8 % of the cases. Ramus intermedius was present in 16.9%. Conus artery from Right coronary artery found in 72.6%, with a same ostium was observed in 10.3 % and in 16.9 % conus arteries originating with separate ostia were visualized. The sinus node artery (SNA) originated from the right coronary artery (RCA) in 66.9% and from the Left Circumflex artery (Cx) in 33%. LMCA was absent in 0.9%. Myocardial bridging was observed in 11.3%. Conclusion: Complex anatomy of the coronary artery tree can precisely be showed by 64-slice CTA. This technology is an appropriate substitute to conventional coronary angiography in distinguishing coronary artery variations and anomalies.
Keywords: Anatomic Variations, Coronary Artery
Full Text:
INTRODUCTION
Coronary artery anomalies can be fatal during or subsequent to heavy physical activity, usually in young population. The information of coronary anomalies is also crucial for cardiologist before performing any invasive procedure in coronary artery disease patients. The coronary anomalies cause 11.8% deaths in young athletes in USA.(1) An another study depicted that 12% of sports-related sudden cardiac deaths and 1.2% of non-sports-related deaths were originated from coronary abnormalities in 14 to 40 year-old persons. (2)
Screening of coronary anomalies in population is becoming viable with Contrast-enhanced CT angiography. In comparison with Conventional angiography, coronary CTA has developed into an imperative non-invasive modality in the diagnosis of coronary artery disorders. High temporal and spatial resolution capabilities of multislice computed tomography (MSCT) scanners enable detailed 3D visualization of complex coronary artery anatomy without motion artefact. The introduction of new generation MSCT, making novel, detailed coronary artery studies possible. The origin, course, variations and anomalies of the coronary artery along with, the anatomy of the heart can now be meticulously studied with coronary CTA.(3,4) Furthermore, radiologists now have more skill in interpretation of images on normal anatomy in terms of anatomic anomalies and their cross-sectional images, which shows the way to improved diagnostic precision.(5) In this study, we aimed to recognize the 64-slice CTA appearance of the anatomic variations and anomalies of the coronary arteries and find out their incidence in a population of 106 patients.
MATERIALS AND METHODS
Population
CT data of 106 patients (91 male, 15 female, , range 31–78 years), who underwent 64-slice coronary CTA from January 2007 to December 2012 in Department of Radiology ,GMCH, Udaipur, were retrospectively assessed for anatomical variations and anomalies of coronary arteries. Patients were included who were advised by clinicians for coronary CTA screening or suspected coronary artery disease (CAD).The Institutional Review Board approved the study protocol.
CT scan and reconstruction parameters
All evaluations were carried out with a 64-slice CT scanner (Sensation 64, Siemens- Forcheim, Germany) with the subsequent parameters: slices/collimation 64/0.6 mm, rotation time 330 ms, effective temporal resolution (with 180° algorithm) 165 ms, 120 kv, 950 mAs, table feed/s 11.63 mm, effective slice thickness 0.6 mm, reconstruction increment 0.3 mm, field of view (FOV) 140–180 mm, isotropic voxel resolution of 0.4 ×0.4×0.4 mm.
×0.4×0.4 mm.
Blood urea and serum creatinine levels were estimated before the procedure. Patients were premedicated with tablet propronalol (40 mg); those have a heart rate more than 75 beats/min one hour before the scan. Sublingual nitro-glycerine was also given to the patient just before the scan. After sensitivity test a bolus of 100 ml of high iodinated contrast material (350 mg/ml ultarvist German remedies) was injected with a flow rate of 5 ml/s, followed by a 40-ml saline chaser into an antecubital vein of the right arm. Synchronization between arterial route of contrast and coronary CTA was done with the help of bolus-tracking technique. Collection of data were done in end-diastolic phase (from -300 to -450 ms just prior the peak of the successive R wave) or end-sistolic phase by retrospective gating to get a clear image of the right coronary artery (RCA).
Image analysis
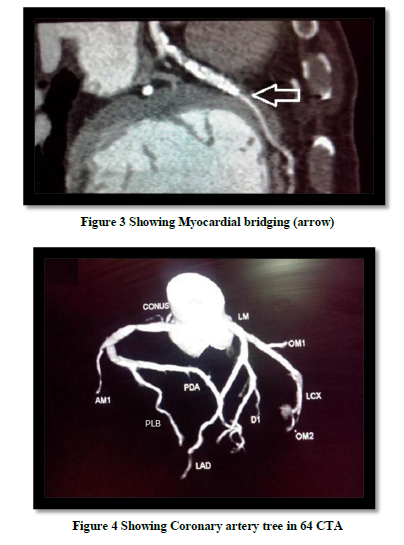
Image analysis was carried out to another workstation where the reconstructed Images at optimal phase were transferred. Interpretation of radiological images were done in axial projection initially with the following tools ,like Volume-Rendering Technique (VRT) with transparent background display, curved planar reformat (CPR), thin-slab maximum intensity projection (thin MIP) and multiplanar reconstructions (MPR).Evaluation of images starts from examining the dominance of the coronary artery , their branching pattern, the origin, course, and supplying region of the major coronary arteries were assessed. The origin of the posterior descending artery (PDA) is deciding factor for dominance pattern in coronary artery. Right dominance were defined as when PDA originating from the right coronary artery (RCA) in coronary artery systems and when PDA arising from the left main coronary artery (LMCA) were defined as left dominant. Coronary artery systems where PDA was come up from the RCA and most of part of the left ventricle’s posterior wall was supplied by posterolateral branches (PLB) from the circumflex artery (Cx) were termed as co-dominant. (6)
Coronary artery anomalies were classified according to Angelini et al. They classify coronary anomalies according to their origination, course, termination and anomalies of intrinsic coronary artery anatomy. (7)
RESULTS
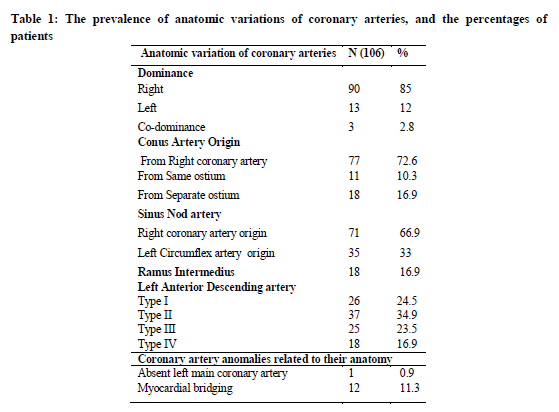
Prevalence of normal variations and anomalies of coronary arteries observed in this study is demonstrated in Tables 1. Total 106 patients were screened through CTA. Right dominance was revealed in 90 patients (85.0%), left dominance in thirteen (12 %), and co-dominance in three (2.8%). The Most common origin of conus artery was from RCA in 77 out of 106 cases (72.6 %), the conus artery is also originated from same ostium or the right sinus valsalva in 13/106 cases (12 %), and it had a separate ostium origin in the remaining 18 cases (16.9%). The sinus node artery (SNA) originated from the RCA in 71 cases (66.9 %) and the left main coronary artery (LMCA) in 35 cases (33 %).The Ramus intermedius branch were found in 18 cases. The variation in LAD was found as type I in 26 cases (24.5%), type II in 37 cases (34.9 %), type III in 25 cases (23.5 %) and type IV in 18 cases (16.9%).Type I is described as not supplying the apex, type II partially supplying the apex and type III supplying entire the apex and type IV wraps around the apex.
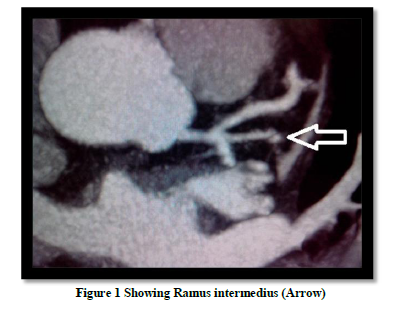
Coronary artery anomalies were observed in a total of 13 cases (57.8%). One case (0.9%) had no Left Main Coronary Artery (LMCA). Left anterior Descending (LAD) and Left Circumflex (LCx) had outflows with separate ostia from the left sinus valsalva due to the absence of the LMCA. In this case LAD and LCx originated from the sinus valsalva between the aortic annulus and sino-tubular junction and blood flow was not low or high.
The LMCA trunk presented a variable length (mean 11.35±3.3 mm, range 1.2–18.7 mm, : <1 cm (n=34, 33%), 1–2 cm (n=72, 67.9%).
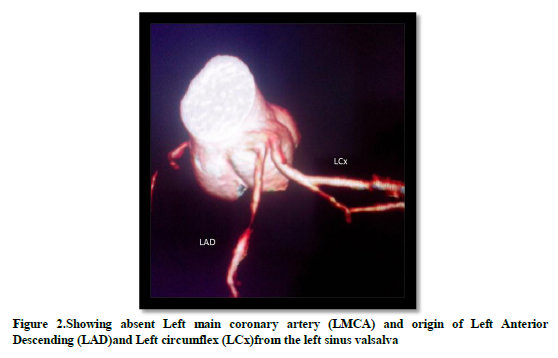
When coronary arteries runs via myocardium, it is called as Myocardial bridging, was observed in 12 of 106 cases (11.3%). The mid-distal segment of the Left Anterior Descending was commonly affected by myocardial bridging.
DISCUSSION
The appropriate knowledge of coronary artery variant or anomaly is very helpful to avoid difficulties during cardiac interventions or complications during graft surgery. Angioplasty process requires a precise anatomical evaluation of the coronary artery branching for revascularization purposes. (8) Coronary anomalies are relatively asymptomatic and sometimes accidentally discovered. The coronary anomalies may be the cause of severe complications, so they are not be consider just rare. (9)
Interpretations of coronary CTA images should be commenced by the study of dominance of the coronary artery system. Earlier studies on coronary CTA examination have essentially commented on this aspect .(10,11) Co- dominance is described by different authors but there is no marked concord on co-dominance and some authors defined that if the PDA and the posterior left ventricular branches together supply blood to the infero-lateral section of the posterior septum. (11, 12) Previous studies were revealed that the rate of right dominance was 80-85%, left dominance was 7-9%, and co-dominance was 5-8%. (10, 11, 12) In our study, right dominance was found in 85%(90 cases), left dominance in 12%(thirteen cases) and co-dominance in 2.8%(three cases).The rates of right and left dominance of this study were somehow similar with the earlier studies, but the lower co- dominance rates may be clarified by the fact that different authors had no agreement on co-dominance of the coronary arteries.
The conus artery commonly originates from the RCA but it may also originate from the right sinus valsalva via a separate orifice. (13) In our study, the conus artery originates from the right coronary artery in 77(72.6 %) patients , common origin from same ostium (right conus artery and right coronary artery from right sinus of Valsalva) was seen in 11(10.3%) patients and separate ostium (aortic) origin of conus artery was seen in 18(16.9% ) patients. The origin of conus artery according to a study was, from RCA 83.1% and from same ostium 16.86%.(14) In contrast to this study our study shows a higher incidence of conus artery origin from separate ostium (10.3%).It may be because of geographical and racial difference.
In our study, it was found that the SNA originated from the RCA in 71 cases (66.9 %), from the Left Cx in 35 cases (33%). Our findings well correlated with the literature which has observed that the SNA is most commonly originated from the RCA. (14)
Anatomically LMCA has two branches, LAD and Cx but sometimes it may trifurcate and the third branch is called as Ramus intermedius which is the most common variation in LMCA. The Ramus intermedius artery itself has variable branching. The Ramus intermedius can be of two types .When it supplies the anterior wall, it is identified as a diagonal branch and when it supplies the lateral wall, it is described as an obtuse marginal branch. In our study, the Ramus intermedius variation was found in 18 cases (16.9 %), this branch is one of most common variations observed in the left coronary arterial system with an incidence rate of 33%.Our observation was lower than the previous studies. (5, 15)
The incidence of the absence of a LMCA is very low in previous studies from 0.41 to 0.52% (16, 17) however Cademartiri et al. notified a high incidence rate of 3.3%.(18) We found only one case (0.9%) of the absence of the LMCA .The incidence rate for the absence of the LMCA in our study was comparable to the former observations. (5, 15) The absence of a LMCA does not have any clinical consequences and does not affect blood flow to myocardium. Although The lack of information about this anomaly may lead to misdiagnosis for example a normal LAD and Cx can be considered stenotic mistakenly in case of the absence of a LMCA. (16) Such errors can be avoided when screening of coronary artery performed by CTA and identification of such anomalies is important before planning invasive procedure for the LMCA. (17, 19)
The coronary arteries usually have an epicardial course but occasionally they may have an intra-myocardial segment. This condition is described as myocardial bridging .The incidence rates for this have been reported as 0.5-2.5% in invasive coronary angiographies while the rates are higher (10.9-43.3%) in 64 and 128 slice CT angiographies. (14,18) Normally this does not cause a problem for a person who have it, but it may rarely result in acute myocardial infarction (MI), acute coronary syndrome, coronary spasm, rupture of ventricular septum, arrhythmia, or even sudden death. Though, in arrhythmic patients with angina, myocardial bridging should be excluded. (5,20,21)We found that the myocardial bridging was observed in a total of 12 cases (11.3%) in the current study. Myocardial bridging was most frequently observed in the mid-distal segment of the LAD. Our study revealed that CTA is very precise in detecting myocardial bridging.
Anomalies of coronary arteries may generally do not create a significant risk to myocardial perfusion but sometimes these may lead to fatal pathologies which may couse in sudden cardiac casualty and myocardial ischemia. Sudden cardiac deaths among young people after exercise or sport activity are due to coronary artery anomalies.(22) Invasive coronary angiography does not give a complete information, and the details are limited about the origin of anomalies. (23) New –generation CT modality provide an accurate and detailed information about all the of the above coronary artery variations to cardiologists.
CONCLUSION
In conclusion, the 64-slice CT is an efficient diagnostic tool to evaluate the anatomic variations and anomalies of the coronary arteries and give comprehensive and accurate information about it. The coronary CTA can replace the percutaneous invasive procedures or preoperative catheter angiography for coronary arteries, and it may also be more beneficial to patients because of its low radiation dosage relative to invasive angiography, the opportunity to use less of a contrasting agent, the increase in the number of cross-section, test duration, shortening the improvement in temporal resolution and its non-invasive approach increasingly supports the use of this technique.
References:
- Van Camp SP, Bloor CM, Mueller FO, et al. Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc. 1995; 27: 641–647
- Burke AP, Farb A, Virmani R, et al. Sports-related and non-sports-related sudden cardiac death in young adults. Am Heart J. 1991; 121: 568–575.
- Flohr T, Ohnesorge B. Heart rate adaptive optimization of spatial and temporal resolution for electrocardiogram-gated multislice spiral CT of the heart. J Comput Assist Tomogr 2001;25:907-23.
- Okur A, Onbas O, Karaman A. MDBT koroner anjiyografi. Multidedektör BT koroner anjiografi, sonuçlar?n güvenirli?i ve radyasyon dozu. Bölüm 1. In: Okur A, Kantarc? M, editors. ?stanbul: Aktif Yay?nevi; 2006. s. 1-11.
- Ko?ar P, Ergun E, Oztürk C, Ko?ar U. Anatomic variations and anomalies of the coronary arteries: 64-slice CT angiographic appearance. Diagn Interv Radiol 2009;15:275-83.
- Zimmet JM, Miller JM. Coronary artery CTA: imaging of atherosclerosis in the coronary arteries and reporting of coronary artery CTA findings. Tech Vasc Interv Radiol 2006; 9:218–226.
- Angelini P, Velasco JA, Flamm S. Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation 2002; 105:2449–2454.
- Cheng TO Prevalence and relevance of coronary artery anomalies. Cathet Cardiovasc Diagn 1997; 42:276–277.
- Angelini P, Velasco J.A., Flamm S. Current Perspective-Coronary Anomalies-Incidence, Pathophysiology, and Clinical Relevance Circulation. 2002; 105: 2449-2454 doi: 10.1161/?01.CIR.0000016175.49835.57
- Bluemke DA, Achenbach S, Budoff M, Gerber TC, et al. Noninvasive coronary artery imaging: magnetic resonance angiography and multidetector computed tomography angiography: a scientific statement from the American Heart Association committee on cardiovascular imaging and intervention of the council on cardiovascular radiology and intervention, and the councils on clinical cardiology and cardiovascular disease in the young. Circulation 2008 29; 118:586–606.
- Kini S, Bis KG, Weaver L. Normal and variant coronary arterial and venous anatomy on high-resolution CT angiography. AJR Am J Roentgenol 2007;188:1665-74.
- Patel S. Normal and anomalous anatomy of the coronary arteries. Semin Roentgenol 2008;43:100-12.
- Miller SW. Normal angiographic anatomy and measurements. In: Miller SW, editor. Cardiac angiography. Boston: Little, Brown; 1984. p. 51-71.
- Kayan M, Yavuz T, Munduz M, Türker Y, Ye?ilda? A, Etli M, et.al. Evaluation of coronary artery anomalies using 128-Slice computed tomography. Temmuz 2012, Cilt 20, Say? 3, Sayfa(lar) 480-487.
- Dewey M, Kroft LJM. Anatomy. In Dewey M, editor. Coronary CT angiography. Berlin: Springer; 2009. p. 11-26.
- Duran C, Kantarci M, Durur Subasi I, Gulbaran M, Sevimli S, Bayram E, et al. Remarkable anatomic anomalies of coronary arteries and their clinical importance: a multidetector computed tomography angiographic study. J Comput Assist Tomogr 2006;30:939-48.
- Montaudon M, Latrabe V, Iriart X, Caix P, Laurent F. Congenital coronary arteries anomalies: review of the literature and multidetector computed tomography (MDCT)- appearance. Surg Radiol Anat 2007;29:343-55.
- Cademartiri F, La Grutta L, Malagò R, Alberghina F, Meijboom WB, Pugliese F, et al. Prevalence of anatomical variants and coronary anomalies in 543 consecutive patients studied with 64-slice CT coronary angiography. Eur Radiol 2008;18:781-91.
- Goel S, Dhir A. Absent left main coronary artery. Ann Card Anaesth 2007;10:61-2
- Ko SM, Choi JS , Nam CW , Hur SH. Incidence and clinical significance of myocardial bridging with ECG-gated 16-row MDCT coronary angiography. Int J Cardiovasc Imaging. 2008;24(4):445-52.
- Canyigit M, Hazirolan T, Karcaaltincaba M, Dagoglu MG, Akata D, Aytemir K, et al. Myocardial bridging as evaluated by 16 row MDCT. Eur J Radiol 2009;69:156-64.
- Shabestari AA, Akhlaghpoor S,Tayebivaljozi R ,and Masrour F.F.Prevalence of Congenital Coronary Artery Anomalies and Variants in 2697 Consecutive Patients Using 64-Detector Row Coronary CT Angiography Iranian Journal of Radiology. 2012 ; 9(3): 111-121.
- Van Ooijen PM, Dorgelo J, Zijlstra F, Oudkerk M. Detection, visualization and evaluation of anomalous coronary anatomy on 16-slice multidetector-row CT. Eur Radiol 2004;14:2163-71.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





