IJCRR - 5(15), August, 2013
Pages: 6-11
Date of Publication: 17-Aug-2013
Print Article
Download XML Download PDF
CLINICALLY RELEVANT MORPHOMETRIC AND TOPOGRAPHIC ANALYSIS OF CORONARY OSTIA
Author: Dattatray Dombe, Takkallapalli Anitha, Sanjay Kalbande, Thaduri Naresh
Category: Healthcare
Abstract:Background: Accurate knowledge of coronary ostia is not only important for anatomists but also for radiologists and intervention cardiologists performing angiographies and shunt surgeries. The high prevalence, morbidity, mortality and enormous socioeconomic burden of coronary artery disease, has necessitated us to take up this study. We have made a sincere attempt to describe the normal and variant anatomy of the coronary ostia in 64 cadaveric hearts of Indian origin. The origin of coronary arteries, the number of coronary ostia, their location in relation to sinotubular junction and the diameter of coronary ostia were observed and their clinical implications are discussed. Aim: To study the variations in number, location of coronary ostia in aortic sinuses and measuring their diameter. Methodology: Sixty four cadaveric hearts with great vessels attached were analyzed in this study. The ascending aorta cut longitudinally at the posterior aortic sinus to visualize right and left posterior aortic sinus for analysis. Results: In all 64 heart specimens right coronary ostia was present in anterior aortic sinus and left coronary ostia in left posterior aortic sinus. Multiple coronary ostia were noted in 18.7% of cases. Conclusion: The great importance of coronary catheterization for diagnostic and therapeutic purposes has currently motivated the present study.
Keywords: Coronary arteries, Coronary ostia, Aortic sinuses, Anomalous.
Full Text:
INTRODUCTION
Coronary catheterization for diagnostic and therapeutic purposes has assumed significance in recent times, as the incidence of coronary artery diseases has seen an increasing trend in developing countries in the last few decades. Considering the hypothesis formulated by some authors [1,2] that changes in coronary flow may be due to changes in diameter, position and anatomic relations of the coronary ostia, this study provides data regarding the variations of coronary ostial origins, emphasizing the importance of such anatomic variants in the development of treatment.
In the vast majority of people, there are two main coronary arteries, right and left, which arise from separate ostia in the aorta. The bulbar aortic sinus and the proximal ascending aorta comprise the aortic root. A slight circumferential thickening, known as the sinotubular ridge (sinotubular junction) marks the separation of these two structures. The bulbous sinus and the three aortic cusps merge to form the sinuses of valsalva. The right sinus of valsalva lies right and anterior in the aortic root and contain the right aortic semilunar cusp, where as the left sinus of valsalva lies left and posterior in the aortic root and contains the left aortic semilunar cusp. The posterior sinus of valsalva lies posterior to the right sinus and contains the non coronary aortic semilunar cusp [3].
The coronary ostia are usually located below the sinotubular ridge within the sinus of valsalva, centrally located between the commissural attachments of the aortic cusps [4]. The ostium of each coronary artery tends to form a slight funnel, with the diameter of the left main coronary artery at its ostium slightly larger than that of the right coronary artery (mean 4.0 versus 3.2mm) [5].
MATERIAL AND METHODS
64 formalin fixed cadaveric hearts with their great vessels attached were used in this study, which was carried out in the department of Anatomy at Chalmeda Anandrao Institute of Medical Sciences, Bommakal, Karimnagar, India, over a period of 3 years i.e. 2010 to 2013. The hearts were dissected, the pericardium involving the root of the aorta was removed, and the origin of the right and left coronary arteries was isolated. Then, the ascending aorta was sectioned approximately 3cm above the commissures of the aortic leaflets. Next, the aorta was longitudinally opened at the level of posterior aortic sinus (non coronary sinus) to enable the visualization and analysis of the right and left aortic leaflets and their respective coronary ostia. In addition, the coronary arteries were sectioned at the level of their origins in the aortic wall (Juxta mural portion of the coronary arteries). The coronary ostia in relation to the right and left aortic leaflets were identified. The origin of coronary arteries, number of coronary ostia, their location in relation to the sinotubular junction and the diameter of coronary ostia using the vernier caliper were noted and tabulated.
RESULTS
The following criteria have been taken into consideration
1) Origin of right and left coronary arteries.
2) Number of coronary ostia in various aortic sinuses.
3) Location of right and left coronary ostia in relation to sinotubular junction.
4) Diameter of right and left coronary ostia.

DISCUSSION
The morphometric and topographical analysis of coronary ostia have been implicated in various clinical conditions and awareness of these anatomical variants may decrease the morbidity and mortality associated with various invasive procedures.
The aortic root is a frequent site of interventional procedures in both adults and children. Understanding the precise nature and relation of the anatomical structures composing the aortic root including coronary orifices is valuable in percutaneous and transcatheter therapeutic techniques for valve or device implantations as well as in various open heart procedures [6].
The origin of coronary artery is an important parameter in cardiac procedures. A single coronary artery occurs in 0.024% of people. It is usually benign but may be associated with congenital heart disease, such as transposition of the great arteries, tetralogy of Fallot, truncus arteriosus and coronary artery fistula [7]. Despite the anomalous origin, the peripheral coronary artery distribution is usually normal. This entity can be mistaken for two separate ostia originating from the same sinus of valsalva or for artesia of coronary ostium [8]. In 25% of patients with a single coronary artery, a major branch crosses the infundibulum, which can not only cause chest pain, myocardial infarction or sudden death but also has technical implications for the surgeon when exposing the heart, instituting extracorporeal circulation or when performing a right ventriculotomy.
The origin of right and left coronary arteries from the anterior aortic and left posterior aortic sinuses respectively is 100% in the present study and matches the standard books of anatomy[9] [Table No.1].
Presence of multiple anomalous ostia is rare and could cause certain clinical consequences. An abnormal location or an accessory origin of the coronary orifices may disturb performing an aortotomy incision for aortic exposure, preparing a coronary button in root replacement, direct delivery of cardioplegia through the coronary orifices and approach for aortic root enlargement [5].
Solitary coronary ostium giving rise to solitary coronary arteries can be a substrate for sudden cardiac death and carries the potential to precipitate severe ischaemic heart disease, including myocardial infarction in younger patients [10]. However, we could not find a solitary coronary ostium in the present study [Table No: 2].
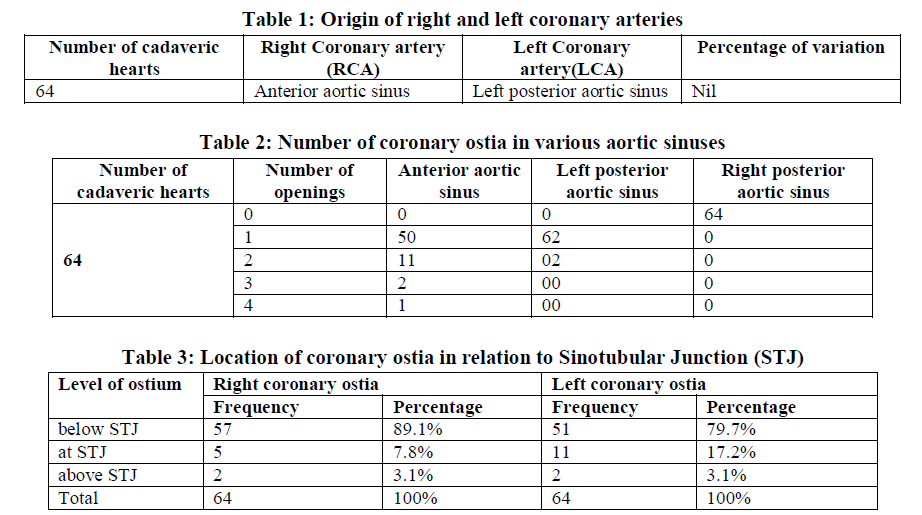
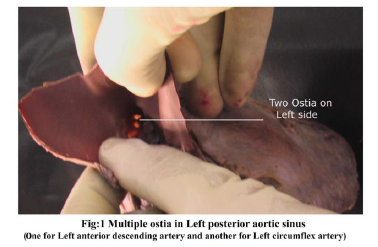
When multiple ostia are observed in the anterior aortic sinus, the most common variation observed is an accessory orifice for right conus artery [11]. The third coronary artery usually forms an anastomosis with the likewise branch of left coronary artery. This anastomosis lies on the distal part of the pulmonary trunk and is known as the “vieussens arterial ring”. This may serve as collateral path between the right and left coronary arteries. Similar observation was made in our present study where 2 ostia arose from anterior aortic sinus in 11 cases (Fig: 2) [Table No. 2].
In approximately 8% of hearts, the openings were three or more in number. In such cases, one of the extra ostia may be that of SA nodal artery. In 50% of cases, the SA nodal artery arises as a branch of the initial part of the right coronary artery [11]. In the present study, three coronary ostia were seen in anterior aortic sinus in 2 cases. One heart had 3 separate ostia in the anterior aortic sinus for the right coronary, right conus artery and a vasa vasorum to the pulmonary trunk.
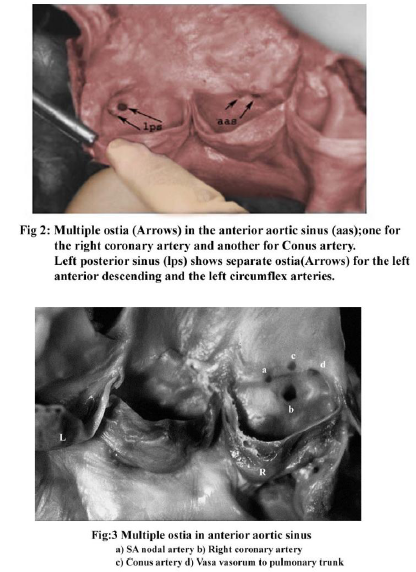
The present study reports 4 separate ostia (Fig: 3) in the anterior aortic sinus of a single heart. One of the ostia was for the right coronary and the three accessory ostia were for the right conus and SA nodal arteries and vasa vasorum to the pulmonary trunk [Table No.2].
Presence of multiple ostia is a hazard to heart surgeries as the ostia of small arteries like third coronary artery are usually very small and barely get opacified in angiographies, thus these arteries miss detection preoperatively and can get nicked during surgery [12].
The preoperative knowledge of location of coronary ostia in relation to sinotubular junction is important in the management of patients with different pathologies involving the aortic root and coronary arteries. Alexander et al [13] stated that the right and left coronary ostia arise normally within the aortic sinuses or at the junction of sinus and tubular portions of aorta. Such a location of ostium allows maximal coronary filling during ventricular diastole. Alexander described a record position of ‘High take off coronary artery’ as 2.5cm above the sinoaortic junction. The detection of such high originating coronary arteries is clinically significant because it can decrease the diastolic coronary arterial filling and such arteries can be missed while performing procedures like coronary angiography.
Vlodover et al [14] stated that both the coronary ostia were observed above the sinotubular ridge in 6% of randomly selected hearts. This becomes important to the operator attempting to perform coronary angiography, where selective intubation of the anomalous vessel may be extremely difficult, especially in the case of the right coronary artery with a high anterior ostium.
In our present study 3.1% of cases of both right and left coronary ostia were above the sinotubular junction [Table No.3].
The diameter of coronary ostia is also significant. The proximal segment of each coronary artery is intramural; it courses through the aortic wall and is usually tapered or funnel shaped. Jenny sales cavalcanti et. al. [15] reported 16% reduction in juxta mural diameter of RCA compared to the ostial diameter and in LCA the reduction was 11%. This needs to be considered when designing stents for aorto-ostial coronary lesion in order to achieve optimal results avoiding retrograde aorto coronary dissection and reducing restenosis. The smaller dimension of some coronary artery segments has important diagnostic and therapeutic implications since for any interventional procedure the absolute size of the coronary artery matters.
It has been reported that occlusion or thrombosis is more common in vessels less than 2.5mm in diameter. A moderate (60%) stenosis in a 2.5mm vessel would have more effects on flow than the same degree of stenosis in a 3.5mm vessel as the cross sectional area in the former would be reduced to 1.76mm2 as compared to 3.46mm2 in a larger vessel. Thus a moderate plaque would cause significant implications in coronary revascularization.
In our present study, the mean ostial diameter of left coronary artery was larger than right coronary artery [Table No. 4].
CLINICAL SIGNIFICANCE
Accurate knowledge of the locations of the coronary ostia in relation to the aortic root is critical for a number of interventional and surgical cardiovascular procedures, including cannulation or catheterization of the coronary arteries, aortic graft repair or root replacement and implantation of percutaneous aortic valves or transapical replacement. The recent advent of percutaneous aortic valves, providing a non-operative treatment of symptomatic aortic valve disease has necessitated continuing development of device, techniques and treatment protocols for optimization of percutaneous aortic valve procedures [16]. With the proximity of the coronary ostia to the aortic annulus and valve leaflets, a particularly challenging issue is the risk of obstruction of the coronary ostia during percutaneous aortic valve replacement.
Concerning percutaneous and transapical valve replacement, obstruction of the coronary arteries during and/or after implantation remains a risk that can have catastrophic consequences. Boudjemline and Bonhoeffer [17] point out that precise placement, with respect to height of percutaneous aortic valve is crucial. Locations too high above the valve annulus result in coronary ostial obstruction and locations too low can negatively impact left ventricular and/or mitral valve function.
CONCLUSION
Knowledge of variants in coronary anatomy is important as failure to recognize these anomalies may at times create challenges during radio diagnostic, various invasive and operative cardiac procedures.
References:
-
Leguerrier A, Calmat A, Honnart F, etal, Anatomic variations of the aortic coronary openings. Bull ASSO Anat (Nancy) 1976; 60: 721-31
-
Brewgr RJ, Deck JD, Capiti B etal. The dynamic aortic root cardiovasc. surg. 1976;72:413-17
-
David M-Fiss-Normal coronary anatomy and anatomic variations. Supplement to applied radiology www.applied radiology.com January 2007, 14-26
-
Balm DS, Grossman W. coronary angiography In: Balm S,ed Grossman’s Cardiac Catheterization, Angiography and Intervention 6th ed Philadelphia, Pa: Lippincott Williams and Wilkins; 2000; 211-256
-
Baroldi G, Scomazzoni G. coronary circulation in the normal and the pathologic heart Washington DC, Armed forces institutes of pathology. 1967.
-
Parimala Sirikonda, Sreelatha S-Measurements and location of Coronary ostia – Int J Bio. Med. Res. 2012;3(4);2489-2496.
-
Memisoglu E, Hoblkoglu G, Tepe Ms. Congenital Coronary anomalies in adults; comparison of anatomic course visualized by catheter angiography and Electron beam CT. Catheter cardiovasc. interv. 2005;66:34-42.
-
Byrum CJ, Blackman MS, Schneider B et al. Congenital atresia of the left coronary ostium and hypoplasia of the left main coronary. Am Heart J. 1980;99:354-358.
-
Standing S. Gray’s Anatomy 40th ed.spain; Churchill Livingstone Elsevier; 2008 978-980.
-
Koiumi,M, Kawai, k, Honma,s, kodma, k. Anatomical study of single coronary artery with special reference to the various distribution patterns of bilateral coronary arteries. Ann.ANAT 2000; 182:549-547.
-
Schlesinger MJ, Zoll PM, Wessler S. The conus artery; A third coronary artery. AM Heart J. 1949; 38:823-836.
-
Vaishaly.K. Bharambe, vasanti Arole, A study of variations in coronary ostia. J Anat. Soc. India 2012, 61[2] 221-228.
-
Alexander W, Schlant RC, Foster V. The heart 9th ed. London: Mcgraw-Hill; 1995, Chapter2, Anatomy of heart, p-55.
-
Vlodaver Z, Neufeld HN, Ed Wards JE. Pathology of coronary disease. Semin. Roentgenol 1972, 7:376-394
-
Jenny sales cavalcanti, Natalia correa vielrademelo, Renatasimoes de vasconcelos. Morphometric and topographic study of coronary ostia. Arq Bras cardiol 2003;81:359-362
-
Lutter G, Ardehali R, Cremer J, Bon hoeffer P, percutaneous valve replacement: current state and future prospects. Ann.Thorac Surg 2004 78[6]: 2199-2206.
-
Boudjemline Y, Bonhoeffer P. steps towards percutaneous aortic valve replacement. Circulation 2002,1056: 775-778.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





