IJCRR - 5(17), September, 2013
Pages: 57-64
Date of Publication: 12-Sep-2013
Print Article
Download XML Download PDF
WORK POSTURE AND PREVALENCE OF MUSCULOSKELETAL SYMPTOMS AMONG WOMEN IN PACKING ACTIVITIES OF PHARMACEUTICAL INDUSTRY
Author: Prasuna Velaga, Neeraja Telaprolu
Category: Healthcare
Abstract:The pharmaceutical industry is one of the major industries of Andhra Pradesh. Huge number of women were employed in these industries to carry out packing activities manually. These packing activities being static and repetitive may give rise to fixed body positions, continued repetition of movements and concentrated force on hand or wrist with out sufficient recovery between the movements. A study was undertaken to determine the prevalence of musculoskeletal symptoms among women workers involved in packing activities of pharmaceutical industry. The sample consisted of 270 women workers randomly selected from nine pharmaceutical industries in Hyderabad. Work posture was evaluated by using RULA (Rapid Upper Limb Assessment) technique. A scale was developed to study the musculoskeletal symptoms in nine anatomical body regions. The musculoskeletal discomforts like pain, stiffness, swelling, spasms and so on experienced by women were explored. Correlation between the postural score obtained with the use of RULA and musculoskeletal symptoms was explored. There was a significant positive correlation between RULA posture score and prevalence of musculoskeletal symptoms. Further through ANOVA significant difference between the respondents with mild, moderate and severe musculoskeletal symptoms was found out. The results emphasized poor working postures of the workers in packing activities need to be changed soon.
Keywords: Musculoskeletal Symptoms, Packing, Pharmaceutical industry, Posture, RULA
Full Text:
INTRODUCTION
The Indian Pharmaceutical Industry is in the first rank among India’s science based industries with wide ranging capabilities in the complex field of drug manufacture and technology (APITCO, 2009, [1]). In pharmaceutical industry though the process of manufacturing is mechanized, the process of packing is still undertaken manually. Mostly the packing is done by women. The majority of packing activities are characterized by a sitting posture, worker’s head and trunk flexed forward and shoulders flexed and abducted. In this situation high rate of work related musculoskeletal disorders occurrence could be expected. Work related musculoskeletal disorders (WMSD) are a group of painful disorders of muscles, tendons and nerves. WMSD arise from ordinary arm and hand movements such as bending, straightening, gripping holding, twisting, clenching and reaching. These common movements are not particularly harmful in the ordinary activities of daily life. These movements become hazardous due to continuous repetition often in a forceful manner with lack of time for recovery between them (Canadian Centre for Occupational Health and Safety, 2005, [2]). The main objectives of present research were (i) Evaluate body postures of workers.
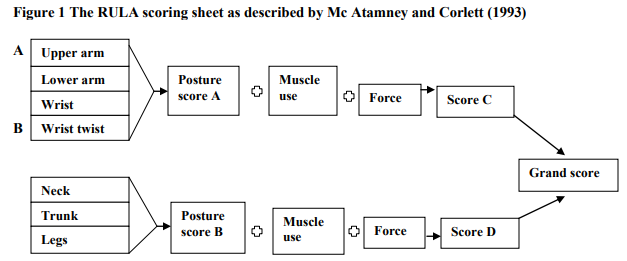
(ii) Determining the prevalence of musculoskeletal symptoms among workers. (iii) Finding out the relationship between body posture and musculoskeletal symptoms. MATERIALS AND METHODS Sampling procedure The state capital of Andhra Pradesh was selected to draw the sample for the present investigation. The women who were involved in the packing activities in pharmaceutical industries for a period of minimum three years and aged above 30 years were selected as the sample for the study. A sample of 270 women was chosen at random from nine pharmaceutical industries from the list procured from office of the Commissioner of Industries. Data collection Back ground information like age, number years of education, number of years work experience were collected by interview method. The prevalence of musculoskeletal symptoms was obtained by developing a scale and using it in the present study. Musculoskeletal symptoms are developed in the nine anatomical regions of the human body such as neck, shoulder, elbow, wrist/hand, upper back, lower back, hips/thighs/buttocks, knees and ankles/feet (Kuorinka et al., 1987, [4] and Dickinson et al., 1992 [5]). Upper limb consists of upper arm, elbow, fore arm, wrist, hand and fingers. The back region of the human body includes upper back and lower back. The lower limb part of the human body includes thigh, knee, ankle, feet and toes (Winwood and Smith, 1985 [6]). In the present investigation the nine anatomical regions were grouped as neck, shoulder, upper limb (upper arm, elbow, fore arm, wrist, hand and fingers), back (upper back and lower back), and lower limb (thigh, knee, ankle, feet and toes). The scale assessed the musculoskeletal symptoms like pain, stiffness, swelling, spasms, cramps, numbness and tingling sensations. The frequency of experiencing the musculoskeletal symptoms in nine anatomical body regions varied from never to always. The frequency of symptoms was assessed as never if symptoms may not present. The frequency of symptoms was assessed as rarely, some times, frequently and severe if prevalence of symptoms was few hours in a week, 1-2 days in a week, 3-4 days in a week and through out the week respectively. Higher the score indicated higher the prevalence of symptoms. The working position of women workers in packing activities of pharmaceutical industry was studied with RULA (Rapid Upper Limb Assessment) technique which is known as penpaper observational method (Mc Atamney and Corlett, 1993, [3]). According to this a score was calculated for the posture of each body part such as upper arm, lower arm, wrist, wrist twist, neck, trunk and legs. A score of 1 indicated the best or most neutral posture, e.g., arms by sides, elbows in approximately 900 flexion, wrist in neutral position, forearms mid- way between pronation and supination, neck in 100 flexion, trunk and legs sitting and well supported. A score of 4 indicated the worst position e.g., shoulder flexion above 900 or flexion between 450 and 900 and abduction. The combined individual scores for upper am, lower arm, wrist and wrist twist gave score A and those for neck, trunk and legs gave score B. Muscle use in each packing worker position were attributed a score of 1 and force exerted 0 or 1 because they were static postures with out loading or with loading of 2 to 10 kg. These scores were added to scores A and B to obtain scores C and D, respectively. And based on the design of the RULA method, each combination of scores C and D (a number of 1-7) called grand scores. Low grand scores (1 or 2) indicate acceptable working posture (action level 1). For grand scores of 3 or 4, further investigation is needed and changes may be required (action level 2). Prompt investigation and changes are required soon for scores of 5 or 6 (action level 3). Finally, immediate investigation and changes are required for grand score of 7 (action level 4) (Fig 1).
Statistical analysis
The interrelationship between RULA scores and presence of musculoskeletal symptoms was assessed through Pearson’s correlation coefficient. Analysis of variance (ANOVA) was computed between the RULA scores and musculoskeletal symptoms of the study to find out the significant mean differences. Step wise regression was carried out to find out the major contributing factor among all the variables.
RESULTS AND DISCUSSION
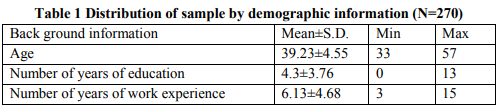
Subject demographic information The mean age of the employees was 39.23±4.55 years; mean number of years of education was 4.3±3.76 years. The mean number of years of work experience of packing workers at the time of assessment was 6.13±4.68 (Table 1).
RULA Scores
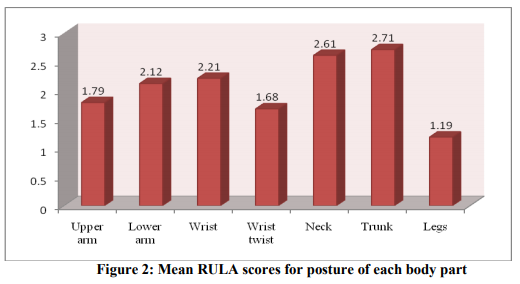
The possible upper arm scores are 1 through 6. The mean upper arm position score of women involved in packing activities was 1.79. This indicates upper arm position was slightly abducted with flexion 150 to 450 but however the movements were continuous. The possible lower arm score is from 1 to 3. The mean lower arm score was 2.12 indicate flexion less than 600 and up to 1000 . The possible wrist score varies from 1 through 4. The mean wrist score was 2.21 indicating many of them placed in extension status and made angle rather than 150 . The possible wrist twist score ranges from 1 to 2. The mean score was 1.68 indicating wrist twist at or near end of range rather than in mid range. The possible neck and trunk position scores are 1 through 6. The mean neck and trunk scores were 2.61 and 2.71. These scores indicate that the neck and trunk of the respondents were in flexion, rotation or side bending. The possible legs score are 1 and 2. The mean legs score was 1.19 (Fig 2).
RULA scores obtained by sample revealed that 79 per cent of the respondents scored 2 for upper arm. Majority of the respondents (88%) obtained lower arm score 2. Nearly eighty per cent of the respondents obtained wrist score 2 and 68 per centwrist twist score 2). Score 3 was obtained by majority of respondents for neck (61%) and trunk (71%). Maximum respondents (81%) obtained score 1 for legs (Table 3).

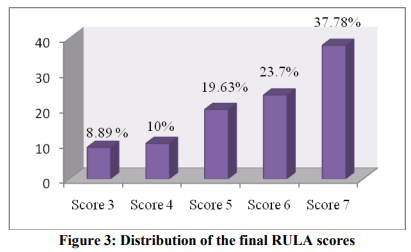
The possible muscle use scores are 0 and 1. All the respondents were working under static positions more than a minute with repetitive actions. This posture lead them to get score 1. The possible load scores vary from 0 to 3. In the present study majority of the respondents (75%) were carrying loads 2 to 10kg hence, scored 1. Only 25 per cent of the respondents were not involved in carrying loads/applying force and thus obtained score 0. The estimated mean for the arm and wrist score was 4.37. The estimated mean for the neck, trunk and legs scores was 5.41. The same results were depicted among VDT workers where the mean arm and wrist score was found to be 4 for men and women and neck, trunk and legs score 4.7 for women and 4.2 for men (Shuval and Donchin, 2005 [7]). The Grand RULA score denotes work posture of the worker while carrying out the work. This includes arm and wrist scores, neck, trunk and leg scores along with muscle use and load scores. The maximum score that can be obtained is 7 which indicate high risk. In the present investigation 33.7 per cent of the women scored 7 (action level 4) means that they had dangerous posture. In case of these respondents the work posture needs to be changed immediately. Scores 6 and 5 indicate medium risk (action level 3) and 43 per cent of the workers were found in this category. There is a need to change this posture soon. Scores 4 and 3 indicate low risk (action level 2). Only 18.9 per cent of the respondents were in this category. RULA scores 1-2 indicate an acceptable posture. But nobody obtained acceptable posture. The mean overall score was 5.7 indicated the need for change of workers’ posture while carrying out packing activities (Fig 2). The mean grand score in packing activities in pharmaceutical industry in Iran was 4.87 (Varmazyar et al., 2009 [10]) and while among truck drivers with posterior mechanism for rubbish collection and those of street cleaning vehicles were 4.71 and 4.53 respectively (Massaccesi et al., 2004[11]).The grand score 7 (action level 4) was calculated for saw mill occupation: saw filter workers (Jones and Kumar, 2007 [8]), grand scores 5 and 6 (action level 3) for carpet mending operation workers (Choobineh et al., 2004 [9]).
Prevalence of musculoskeletal symptoms
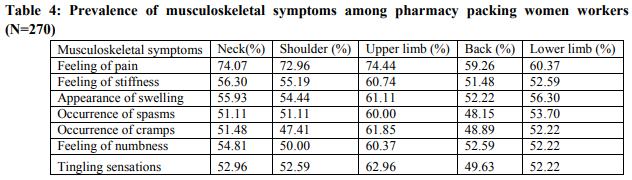
Majority of the respondents were experiencing the feeling of pain in neck (74%) followed by feeling of stiffness (56.3%) and appearance of swelling (55.93%). Among the respondents 74 per cent of the respondents were experiencing the feeling of pain in upper limb, 59.3 per cent in back and 60 per cent in lower limb (Table 4). Pharmacy packaging workers have a high relative prevalence of discomforts in terms of knees (44.7%), back (36.8%) and neck (31.6%) pain (Varmazyar et al., 2009).
Relationship between posture and self reported musculoskeletal symptoms
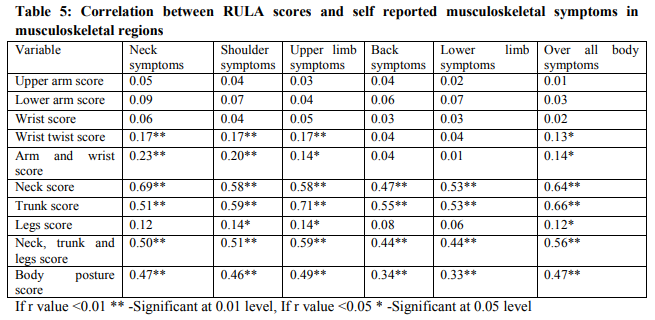
The relationship between upper arm score, lower arm score, wrist score with musculoskeletal symptoms in neck, shoulder, upper limb, back, lower limb and over all body were found to be non-significant. The wrist twist score showed significant positive correlation with musculoskeletal symptoms in neck (r=0.17), shoulder (r=0.17), upper limb (r=0.17) and over all body (r=0.13). Significant positive correlation was found between neck, trunk score with musculoskeletal symptoms in all musculoskeletal regions. Legs score showed significant positive correlation with musculoskeletal symptoms in shoulder (r=0.14), upper limb (r=0.14) and over all body (r=0.13). The arm and wrist score showed significant positive correlation with musculoskeletal symptoms in neck (r=0.23), shoulder (r=0.20), upper limb (r=0.14) and over all body (r=0.14). The neck, trunk and legs score showed significant positive correlation with musculoskeletal symptoms in neck (r=0.50), shoulder (r=0.51), upper limb (r=0.59), back (0.44), lower limb (0.44) and over all body (r=0.56). Body posture score showed significant positive correlation with musculoskeletal symptoms in neck (r=0.47), shoulder (r=0.46), upper limb (r=0.49), back (0.34), lower limb (0.33) and over all body (r=0.47) (Table 5).
Through ANOVA, the computed F values revealed significant mean difference between arm and wrist position score and musculoskeletal symptoms in neck (F=10.76**), shoulder (F=8.35**), upper limb (F=3.02*) and over all body (F=3.95*). The computed F values revealed significant mean difference at 0.01 level between neck, trunk and legs position score and musculoskeletal symptoms in neck (F=26.75**), shoulder (F=26.36**), upper limb (F=42.79**), back (F=19.86**) and lower limb (F=20.08**) and over all body (F=36.85**). The computed F values revealed significant mean difference between body postural score and musculoskeletal symptoms in neck (F=30.70**), shoulder (F=33.33**), upper limb (F=31.67**), back (F=15.89**), lower limb (F=12.12**) and over all body (F=13.47**). Significant differences were observed between RULA body part scores and the reported pain in neck and trunk in packing workers in pharmaceutical industry (Pourmahabadian et al., 2008 [12]). Survey revealed that among truck drivers RULA scores were significant particularly in neck (Massccesi et al., 2003) and similar among carpet menders (Choobineh et al., 2004) According to the results of the present study it can be concluded that the arm and wrist position of women workers in packing activities of pharmaceutical industry was at low to moderate risk. Respondents earned a score of 3, 4 and 5 were categorized as low risk group, moderate risk group and relatively high risk group. Multiple comparisons test was used to compare the risk groups. The women with arm and wrist at low and moderate risk position were sometimes experiencing musculoskeletal symptoms in neck, shoulder, upper limb and over all body. The women with arm and wrist at high risk position were frequently experiencing musculoskeletal symptoms in neck, shoulder, upper limb and over all body. Similar findings were reported by Varmazyar et al. (2008) among packing workers in pharmaceutical industry. The position of arm and wrist while at work play a major role in developing pain and other musculoskeletal symptoms. In the present investigation the neck, trunk, legs position scores less than or equal to 3 were categorized as low risk position, scores 4-6 as moderate risk and scores 7 and above 7 as high risk position. The women with neck, trunk, legs at low risk position were never experienced musculoskeletal symptoms in neck, shoulder and rarely experienced musculoskeletal symptoms in upper limb, back, lower limb and over all body. The women with neck, trunk, legs at moderate risk position were sometimes experiencing musculoskeletal symptoms in neck, shoulder, upper limb, back, lower limb and in over all body. The women with neck, trunk, legs at high risk position were frequently experiencing musculoskeletal symptoms in neck, shoulder, upper limb, back, lower limb and in over all body. According to Mc. Atamney and Corlet (1987) RULA final posture scores 1-2 are acceptable posture scores, scores 3-4 are low risk posture scores, scores 4-6 are moderate risk posture scores and scores 7 and above 7 are high risk posture scores. Women working with low risk body posture were rarely experiencing musculoskeletal symptoms in neck, shoulder, upper limb, back, lower limb and over all body. Women working at moderate risk posture were sometimes experiencing musculoskeletal symptoms in neck, shoulder, upper limb, back, lower limb and in over all body. Women working at high risk posture were frequently experiencing musculoskeletal symptoms in neck, shoulder, upper limb, back, lower limb and in over all body. Through step wise regression the determinants for musculoskeletal symptoms in neck, shoulder, upper limb, back, lower limb and over all body were found. It showed significant results that neck position was contributing for causing musculoskeletal symptoms in neck and trunk position for causing musculoskeletal symptoms in shoulder, upper limb, back, lower limb and over all body.
CONCLUSION
The postural problems were mainly due to awkward postures, repetitive movements and force exertion involved in the work and improper work seat, work table, arm reach in the workplace. Ergonomic interventions could be taken into account to lead the worker to reduce exposure to risk consequently preventing WMSD and hence to improve better health and enhanced productivity in the organization. The suggested ergonomic interventions included engineering controls like providing adjustable work seats and adjustable work tables or redesigning workplace layout; administrative controls like giving rest breaks, training and education in good ergonomic practices and work postures; personal controls like regular exercise for keeping health of the workers.
References:
1. APITCO Limited, Engineering Growth, Draft Diagnostic study report, Pharmaceutical cluster, Hyderabad, Andhra Pradesh submitted to PMD Division, Small Industries Development Bank of India, 2009.
2. Canadian Centre for Occupational Health and Safety, OSH Answers: Work-related Musculoskeletal Disorders (WMSDs). 2005.
3. Mc. L. Atamney, E.N.Corlett, RULA: a survey method for the investigation of work related upper limb disorders. Applied Ergonomics, 24 (2), 1993, 91–99.
4. I.Kuorinka, B. Jonsson, A. Kilborn H. Vinterberg, , S.F. Biering, G. Andersson and K. Jorgensen, Standardized Nordic questionnaire for the analysis of musculoskeletal symptoms. Applied Ergonomics, 1987, 18, 233–237.
5. C.E. Dickinson, K. Campion, A.F. Foster, S.J. Newman, A.M.T.O. Rourke and P.G. Thomas. Questionnaire development: an examination of the Nordic Musculoskeletal Questionnaire. Applied Ergonomics, 23(3), 1992, 197-201
6. R.S. Winwood, Smith, J.L. Anatomy and Physiology for Nurses. (Education Academic and Medicinal Publishing Division of Hodder and Stoughton, London, 1985)
7. Shuval, K., Donchin, M. Prevalence of upper extremity musculoskeletal symptoms and ergonomic risk factors at a Hi-Tech company in Israel. Industrial Ergonomics, 35, 2005, 569-58.
8. T. Jones and S. Kumar, Comparison of ergonomic risk assessments in a repetitive high risk saw mill occupation: saw filter, Industrial Ergonomics, 37, 2007, 744-753.
9. A.Choobineh, R. Tosian, Z. Alhamdi and M. Davarzanie, Ergonomic intervention in carpet mending operation, Applied Ergonomics, 35, 2004, 493-496.
10. S. Varmazyar, A.S. Varyani, I.M. Zeidi and H.J. Hashemi, Evaluation Working Posture and Musculoskeletal Disorders Prevalence in Pharmacy Packaging Workers, European Journal of Scientific Research, 29(1), 2009, 82-88.
11. M. Massaccesi, A. Pagnotta, A. Soccetti, M. Masali, C. Masiero and F. Greco, Investigation of work-related disorders in truck drivers using RULA method, Applied Ergonomics, 34, 2003, 303-307.
12. M. Pourmahabadian, M. Akhavan and K. Azam, Investigation of risk factors of workrelated musculoskeletal disorders in a pharmaceutical industry, Journal of Applied Sciences, 8(7), 2008, 1262-1267.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





