IJCRR - 6(1), January, 2014
Pages: 34-38
Print Article
Download XML Download PDF
MUCORMYCOSIS- AN UNUSUAL PRESENTATION
Author: Tevethia H., Aashish A., Manigandan G., Sunny DAN, Anjay B.
Category: Healthcare
Abstract:Mucormycosis is a rare life threatening invasive fungal infection caused by fungi of order mucorales commonly rhizopus. It usually occurs in immune compromised individuals like diabetic ketoacidosis, leukemia, lymphoma, severe malnutrition, high dose corticosteroids and organ transplantation. It occurs in many forms but the most common being rhinocerebral mucormycosis. A black necrotic eschar is the hallmark of mucormycosis. Patients present with varying manifestations like multiple cranial nerve palsies, unilateral periorbital facial pain, orbital inflammation, eyelid edema, blepharoptosis, proptosis, ophthalmoplegia, headache, and acute loss of vision. Here we describe an unusual presentation of a case of rhinocerebralmucormycosis in an adult female with diabetes mellitus. The reason to present this case is because of the unusual clinical presentation, course and how we arrived at the final diagnosis of mucormycosis.
Keywords: Mucormycosis, eschar, diabetes mellitus, rhizopus
Full Text:
INTRODUCTION
Mucormycosis is a rare life threatening oppurtunistic infection caused by fungi of the order mucorales. It was called as zygomycosis but recent reclassification has placed the order mucorales in the subphylum mucormycitoma and has abolished zygomycetes, hence the term mucormycosis1. Conditions that predispose to this disease include immune compromised states like diabetic ketoacidosis, neutropenia, severe malnutrition, high dose corticosteroids and organ transplantation, trauma. There are six different forms of mucormycosis, the commonest being rhinocerebral mucormycosis.2
CASE REPORT
38 year old adult female who is a known diabetic and hypertensive on irregular treatment presented to the emergency department with decreased levels of consciousness and fever for 4 days. On examination she was disoriented, febrile, blood pressure of 230/120 mm hg, tachycardia, s1 s2 normally heard, bilateral basal rales, abdominal examination was soft, no organomegaly, CNS examination showed equal but sluggishly reacting pupils bilaterally, bilateral plantar mute. Initial investigations showed leukocytosis, urine ketones positive, metabolic acidosis and CT brain was normal. Provisional diagnosis of hypertensive encephalopathy with diabetic ketoacidosis was made and patient was admitted in intensive care unit and started on intravenous fluids, intravenous insulin correction, broad spectrum antibiotics and other supportive medications.
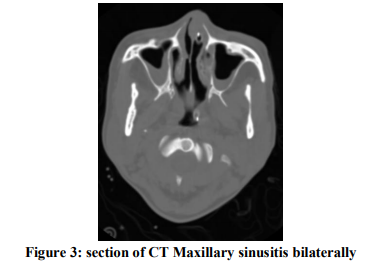
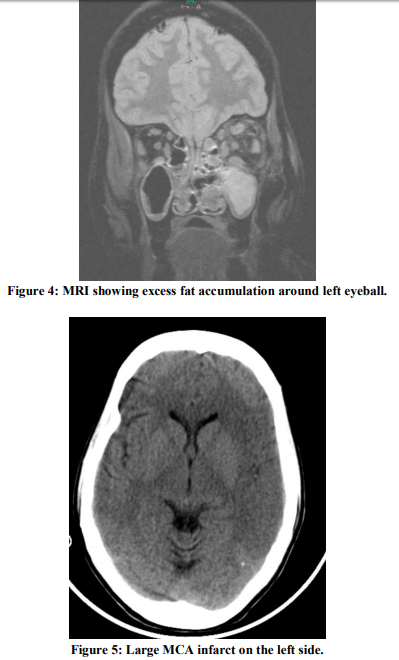
Next morning patient condition deteriorated, her saturation dropped and she was electively intubated. On examination she had right sided plantar extensor with hypotonia was present. Urgent repeat CT scan was done which showed extensive left sided middle cerebral artery infarct(Figure 5). Diagnosis was revised to cerebrovascular accident with diabetic ketoacidosis. 48 hours after admission patient showed no improvement and she developed swelling of her left eyelid(Figure 1) and oral cavity examination showed black eschar on the hard palate(Figure 2) with bloody left sided nasal discharge. MRI brain revealed pansinusitis and excess fat accumulation around the left eyeball(Figure 4).
With high suspicion of mucormycosis nasal endoscopy was done and biopsy was taken. Histopathology of the biopsy revealed rhizopus fungi. Patient underwent urgent debridement and started on intravenous amphotericin b as per guidelines. In the following days patient GCS improved, total counts came down, blood sugar levels was under control, but patient had weakness of her right upper and lower limb with UMN facial palsy on left side due to left sided infarct.
DISCUSSION
Mucormycosis is a life threatening invasive fungal infection caused by organism of order mucorales most commonest being rhizopus1. Based on clinical presentation and the involvement of a particular anatomic site, mucormycosis can be divided into at least six clinical categories: rhinocerebral, pulmonary, cutaneous, gastrointestinal, disseminated, and miscellaneous. Rhinocerebralmucormycosis continues to be the most common form of the disease, accounting for between one-third and one-half of all cases of mucormycosis. About 70% of rhinocerebral cases are found in diabetic patients in ketoacidosis.2It develops due to inhalation of fungal sporangiospores into the paranasal sinuses. The invading fungus may spread inferiorly to invade the palate, posteriorly to invade the sphenoid sinus, laterally into the cavernous sinus to involve the orbits, or cranially to invade the brain. The fungus invades the cranium either through the orbital apex or the cribriform plate of the ethmoid bone. Sometimes vascular invasion leads to hematogenous dissemination and may or may not produce aneurysms.[3,4]
A black necrotic eschar of nasal mucosa or hard palate is the hallmark of mucormycosis.6 However, the absence of this finding should not exclude the possibility of mucormycosis. Fever, marked leukocytosis in the presence of functioning bone marrow. Signs and symptoms that suggest mucormycosis in susceptible individuals include multiple cranial nerve palsies, unilateral periorbital facial pain, orbital inflammation, eyelid edema, blepharoptosis, proptosis, ophthalmoplegia, headache, and acute vision loss. CT brain and MRI usually reveal features of sinusitis and fat accumulation in the extraocular muscles and thrombosis if there is vascular invasion.5
In our patient there was fever, leukocytosis, raised blood sugar, urine ketones positive with metabolic acidosis but patient was drowsy and disoriented, hence the usual symptoms and signs which are classical for mucormycosis couldn’t be recognized which lead the initial treatment towards hypertensive encephalopathy and diabetic ketoacidosis. Furthermore the second CT brain showed large infarct in the left middle cerebral artery territory (Figure 5), which again lead the diagnosis towards cerebrovascular accident. MRI brain revealed pansinusitis with fat accumulation in the extraocular muscles signifying infection in our case. No evidence of thrombosis or aneurysms.
Eventhough cerebrovascular accident could occur in mucormycosis by means of infarct or hemorrhage due to vascular invasion, in this patient there was no evidence of vascular invasion in the form of mycotic aneurysms or cavernous sinus thrombosis in MRI. Only because of the presence of left eyelid swelling (Figure 1), bloody nasal discharge and classical black eschar in the hard palate (Figure 2) with underlying diabetic ketoacidosis mucormycosis was suspected which was later confirmed with histopathological diagnosis.
CONCLUSION
This case highlights the devastating complications that occur in diabetes mellitus. Any immune compromised patient especially those with diabetes mellitus even with subtle symptoms or signs mucormycosis especially rhinocerebral mucormysis should be ruled out, because of its rapid invasive nature it could be life threatening and fatal . Hence due to its varied presentations early recognition and prompt treatment is necessary for better outcome and survival of the patients.

References:
- Hibbett DS, Binder M, Bischoff JF, et al. A higher-level phylogenetic classification of the fungi. Mycol Res 2007; 111:509 - 47.
- Spellberg B, Edwards J Jr, Ibrahim A. Novel perspectives on mucormycosis: pathophysiology, presentation, and management. ClinMicrobiol Rev 2005; 18:556 - 69.
- Hosseini SM, Borghei P. Rhinocerebralmucormycosis: pathways of spread. Eur Arch Otorhinolaryngol 2005; 262:932 - 8.
- Terk MR, Underwood DJ, Zee CS, Colletti PM. MRI imaging in rhinocerebral and intracranial mucormycosis with CT and pathologic correlation. Magn Reson Imaging 1992; 10:81 - 7.
- Petrikkos G, Skiada A, Lortholary O, Roilides.E et al. Epidemiology and Clinical Manifestations of Mucormycosis Clinical Infectious Diseases 2012;54(S1): S23 - 34
- Mallis.A, Mastronikolis S.N, Naxakis S.S, Papadas A.Trhinocerebral mucormycosis: an update European Review for Medical and Pharmacological Sciences 2010; 14: 987- 992
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





