IJCRR - 7(3), February, 2015
Pages: 43-47
Print Article
Download XML Download PDF
INCREASE IN ANTIBIOTIC RESISTANCE: ARE BACTERIA GROWING WITH PAN
RESISTANCE?
Author: V. S. Deotale, Ruchita Attal, P. Narang
Category: Healthcare
Abstract:Introduction: Pan Drug Resistant (PDR) bacteria are currently the leading cause of concern to the clinicians as they pose serious therapeutic challenges. A bacteria that is non-susceptible to all agents in all antimicrobial categories has been defined as PDR. This retrospective study has been undertaken to determine the prevalence of PDR \?GNRs (Gram negative rods) and to assess the risk factors associated with that in hospitalized patients of our rural hospital. Material & Method: A total of 1748 GNRs isolated and identified by standard phenotypic methods from various clinical specimens received in this laboratory between 1st June 2011 to 31st May 2012 from IPD patients were enrolled in this study. Antibiotic susceptibility of these isolates was done using Kirby-Bauer disk diffusion method as per CLSI guidelines. Predisposing factors for acquisition of PDR isolates were also studied. Results: A total of 32 (1.8%) of the 1748 GNRs studied were found to be PDR and these were recovered predominantly from surgical units (31.3%). Among these 45.5% were Acinetobacter species, 24.2% Klebsiella species, 15.2% Pseudomonas aeruginosa and 12.1% E.coli. 53.1% isolates were from pus & wound swabs followed by 21.9% from tracheal swabs. Prolonged hospital stay and patients with surgical interventions were found to be important predisposing factors. Conclusions: PDR-GNRs are originating in our rural hospital and particularly in patients with having prolonged stay in the hospital.
Keywords: PAN drug, PDR-GNR, Acinetobacter
Full Text:
INTRODUCTION
The fight between a mankind and microorganism is going on since ages. Microorganisms keep on acquiring new methods of resistance to the existing antibiotics and to cope up with these phenomenon human beings keep on discovering new antibiotics. It is constantly observed that microorganisms are slowly getting supremacy in their method of acquiring resistance and mankind is lagging behind at times with the discovery of new antibiotics and both them are trying to discover new defence to tackle with each other. Patients who are admitted in the hospital, having suppressed immune system have a greater risk of acquiring bacteria from environment of hospitals. Most of the nosocomial infections arise due to improper hand washings, improper sterilization of instruments and cross infections through patients wearing, IV stand, beddings, leading to surgical wound infections. In the hospital environment amongst many resistant bacteria, Gram negative bacilli are increasingly prevailing1-3. Amongst the Gram Negative bacilli considerable resistance are observed in Enterobacteriaceae and Nonfermenters4 .One of the common mechanism by which these Gram negative bacilli acquires resistance is via production of enzymes “betalactamases”. These betalactamases include ESBLs, AmpC & MBLs. In Indian hospitals, ESBL producing Klebsiella spp are predominant organism responsible for high morbidity. As per the definitions published in the article of Journal European Society of Clinical Microbiology and Infectious diseases 2012. Definition of MDR means “resistant to more than one antimicrobial agent” but no standardized definitions for MDR have been agreed upon yet by the medical community. XDR means: Bacteria, which are epidemiologically significant due to not only to their resistance to multiple antimicrobial agents but also to their ominous likelihood of being resistant to all. Extensively resistant Bacteria (XDR) are resistant to all but 1 or 2 classes of antibacterial agents and Pan drug resistant (PDR) means resistant to all antibiotic classes available for empirical treatment” 5 . Amongst the all Gram negative bacilli Acinetobacter, Pseudomonas and Klebsiella are the predominantly important cause of nosocomial infections due to pneumonia, bactereamia wound infections, nosocomial infections which shows PDR pattern. Globally,prevalent Pan drug resistant-Gram Negative (PDR-GNRs) are Acinetobacter, Pseudomonas & Klebsiella sp.6 The prevalence of PDR-Acinetobacter worldwide is about 0-20% of all Acinetobacter sp.infection.7, 8 In India, prevalence of MDR-GNR vary from 9-90% & PDR- GNR from 2-5%.9,10 The risk factors found to be associated with PDR –GNR infection depends on severity of the illness, admission to ICU, use of invasive interventions, duration of hospital and previous antibiotic use7,8.
MATERIAL AND METHODS:
This observational study was carried out on isolates to study the prevalence of PDR in E.coli, Klebsiella, Pseudomonas & Acinetobacter species isolated from hospitalised patients and to assess the risk factors associated with these organisms from 1st June 2011 to 31st May 2012 in tertiary care rural hospital of central India. Data was collected from case records of all patients from whom PDR-GNR isolates were isolated. Details were included as date of admission, demographic information (sex and age), medical history (underlying diseases, previous use of antibiotic(s), medical devices and corticosteroids), admission to Intensive Care Unit (ICU), site of infection or colonization, laboratory data (the pathogenic organism isolated and their antibiotic susceptibility pattern), mortality, treatment and outcome. E. coli, Klebsiella, Pseudomonas & Acinetobacter isolates from the clinical samples viz: pus & wound swab, endotracheal tube secretions, urine, blood, different body fluids, catheter tips, sputum, vaginal swab, from patients admitted in hospital. Isolates were identified & confirmed by using Standard laboratory techniques,and antibiotics were tested as per CLSI guidelines. Interpretation of zone diameter was done as per CLSI guidelines.11As per the reading of antibiotics, isolate were placed into categories of MDR, XDR and PDR (MDR as: one agent in three or more antimicrobial categories, XDR: resistant to at least one agent in all but two or fewer antimicrobial, PDR: Resistant to all available antibiotics in all antimicrobial groups). Information regarding associated risk factors in patients was retrieved from patient’s Case records.
RESULTS
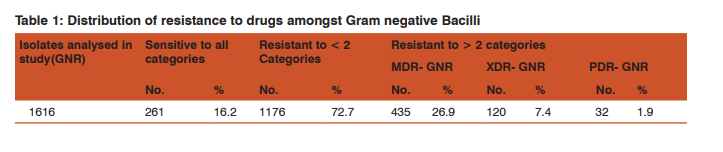
During the study period a total of 1,748 Gram Negative Bacilli were isolated. Amongst 1748, 1616 (92.44) were E.coli, Klebsiella, Pseudomonas and Acinetobacter while 132(7.55) were Salmonella-(3.03), Proteus-(28.03), Shigellaflexnerii-(10.60), Citrobacter-(50.75), Enterobacter-(5.30), Serratia-.(75), Vibrio cholerae –(1.51) and Gram positive positive ( ) organisms. (Table 1) 16.2% isolates were sensitive to all the antibiotics to which isolate was subjected for testing.11.1% isolates were resistant to 2 and > 2 drugs.(Table 2) 26.9% were MDR, 7.4% were XDR & 1.9% were PDR Gram negative bacilli. In E.coli 31.40% were MDR and .5% were PDR while in Klebsiella 26.3% were MDR and 2.10% were PDR. In Pseudomonas and Acinetobacter maximum resistance was seen to drugs of all the categories. In these two organisms 10.20% and 10.30% were XDR while PDR was noted in 2.30% and 6.30%. Acinetobacter showing 10.30% PDR was isolated from Pus, wound swab, tracheal swab and urine samples. PDR from blood sample was isolated from E.coli and pseudomonas .53.1% PDR& 28.3% XDR was isolated from pus and wound swab. Maximum number of MDR was isolated from urine (60%) and E.coli (31.4%). Maximum number of XDR was isolated from tracheal swabs (24.2%).

DISCUSSION
The medical community has been witnessing growing outbreaks of infections due to Gram-negative bacteria resistant to many classes of antibiotics in most countries of the world (Sharma et al., 2005; Canton et al., 2003; Hsueh et al., 2002; Landman et al., 2002). The control of nosocomial infections due to antibiotic-resistant organisms is a public health priority worldwide. It has been documented that bloodstream infection caused by Methicillin-resistant Staphylococcus aureus (MRSA), Vancomycin- resistant enterococci (VRE), extendedspectrum lactamase- producing Enterobacteriaceae, and multidrug-resistant Acinetobacter baumannii are associated significantly with mortality.Numerous papers have demonstrated that prior antimicrobial drug exposure is a strong risk factor for colonization and infection due to a drug-resistant pathogen.12 Studies have identified the risk factors for acquiring infection or colonization with PDR isolates which include the severity of the illness, admission to ICU, use of invasive interventions, duration of hospital stay before specimen collection, previous antibiotic use of especially third-generation cephalosporins, fluoroquinolones, amikacin and carbapenems and use of mechanical ventilator, central venous catheter, Foley catheter and total parenteral nutrition invasive interventions can lead to environmental contamination 13-20. However, the association between antibiotic therapy and the acquisition of antibiotic-resistant bacteria is still unclear and is often confounded by insufficient data on antibiotic usage. We could demonstrate that patients with PDR infection or colonization had a significantly longer length of hospital stay, compared to those infected or colonized with non-PDR. However, the mortality was not significantly different between the two groups. In our study, it was observed that Acinetobactor sp., Pseudomonas, E. Coli and Klebsiella were the organisms showing the resistance to many classes of antibiotics and similar pattern of resistance were observed in other studies done with similar objectives. These organisms are commonly associated with various nosocomial infections including septicaemia, pneumonia, bacteriemia, wound infections; hence, their isolation is more in majority of the studies done with the similar objectives. India currently produces at least 30% of the world’s oral & inject able antibiotics, and could rightly argue they are supporting the WHO agenda of supplying the world with affordable medicines. However, overuse of antibiotics that are excreted by the patients and find their way into hospital and community waste-water systems provides an environmental selection pressure for the emergence and persistence of multi-drug-resistant (MDR) and pandrug-resistance (PDR) bacteria. Thus, at a time when PDR-GNRs are fast becoming a global reality, both academia and pharmaceutical industry are ill equipped to respond. PDR GNRs is an emerging nosocomial pathogen especially in tertiary care settings. Risk factor for PDR-GNR acquisition includes those associated with the patients such as severity of the illness, inappropriate use of antibiotics, surgical interventions, prolonged hospitalization. The prevalence of PDR-Acinetobacter baumanii worldwide is about 0-20 percent of all A. baumannii infections. In Thailand, a report from Siriraj Hospital in Bangkok revealed the prevalence of MDR-AB to be 57.6 percentduring1996 and 1997. No PDR-AB was described during that period.14 The incidence of PDR-AB has been increasing in Maharaj Nakorn Chiang Mai Hospital. From 1998 to 2002, Acinetobacter spp. were either the fifth or sixth most common cause of nosocomial nfections at Maharaj Nakorn Chiang Mai Hospital. However, in 2003 Acinetobacter spp. had become the leading cause of nosocomial infections, followed by Pseudomonas aeruginosa, Klebsiella pneumoniae and E. coli.
CONCLUSION
In our study, the proportion of of PDR- and MDR-Acinetobacter was 6.8% and 15.3%. PDR Acinetobacter mostly isolated from pus and wound swab 7(21.9%) followed by from tracheal swab 5(15.6%). Prolonged hospital stay, surgical interventions and admission to ICU are the factors found to be associated with PDR- GNRs.To know the details regarding prior antibiotic use is very essential.
References:
1. Diekema D.J.,. Pfaller M.A, Jones R. N. et al. Survey of bloodstream infections in Gram negative bacilli; frequency of occurrence and antimicrobial susceptibility of isolates collected in United States, Canada and Latin America for the SENTRY Antimicrobial Surveillance Programme, 1997. Clinical Infectious Diseases, vol.29, no.3, pp.595-607, 1999.
2. Daoud Z. and Afif C.Escherichia coli isolated from urinary tract infections of Lebanese patients between 2000-2009: epidemiology and profile of resistance Chemotherapy Research and practice, vol.2011, Article ID218431, 6pages, 2011.
3. Nass T, Cuzon G.,. Bogaerts P, Glupczynski Y., and Nordmann P. Evaluation of a DNA microarray(check-MDR CT 102) for rapid detection of TEM, SHV and CTX-M extended spectrum beta-lactamases and of KPC, OXA-48 AND VIM, IMP and NDM-1 carbapenemases. Journal of Clinical Microbiology, vol.49, no.4, pp.1608-1613, 2011.
4. Livermore D.M. and. Woodford N. The Betalactamase threat in Enterobacteriaceae, Pseudomonas and Acinetobacter. Trends in Microbiology, vol.14, no.9, pp413-420, 2006.
5. .Falagas M. E.,. Karageorgopoulos D.E. Pandrug resistance (PDR), extensive drug resistance (XDR), and multidrug resistance (MDR) among gram-negative bacilli: need for international harmonization in terminology. Clin Infect Dis ; vol 46: pp.1121–1122, 2008.
6. Fawzia E. Al Otaibi* and Fatma F. Al-Hulaily Imipenemresistant Psedomonas aeruginosa: Epidemiology and susceptibility patterns at a Teaching Hospital in Riyadh, Saudi ArabiaAfrican Journal of Microbiology Research Vol. 6(7), pp. 1527-1533, 23 February, 2012.
7. Salem SE, Dahdouh E, Daoud Z. Resistance of Gram-neg- Salem SE, Dahdouh E, Daoud Z. Resistance of Gram-negative bacilli in Lebanon. ISRN Infectious diseases Volume 2013, Article ID759208, 6 pages.
8. Elham A.M. Retrospective Analysis of Neonatal Bacteremia and Antimicrobial Resistance Pattern in Neonatal Intensive Care Unit Research Journal of Medicine and Medical Sciences, 6(2): 62-68, 2011.
9. Jaykumar S, Appalaraju B Prevalence of multi and pan drug resistant Pseudomonas aeruginosa with respect to ESBL and MBL in a tertiary care hospital Indian J Pathol Microbiol 2007 Oct;50(4):922-5.
10. Sharma J, Gulati N, Chander J. Drug resistant urinary iso- Sharma J, Gulati N, Chander J. Drug resistant urinary isolates of Pseudomonas Aeruginosa and Acinetobacter species. J Global Infect Dis 2010;2:315-7.
11. Clinical and Laboratory Standard Institute. Performance standards for antimicrobial susceptibility testing: sixteenthinformational supplement. CLSI document M100-S16. Wayne, Pa: CLSI; 2006.
12. Hsueh PR, Teng LJ, Chen CY, et al. Pandrug-resistant Aci- Hsueh PR, Teng LJ, Chen CY, et al. Pandrug-resistant Acinetobacter baumannii causing nosocomial infec -tions in a university hospital, Taiwan. Emerg Infect Dis 2002;8:827- 32.
13. Corbella X, Montero A, Pujol M, et al. Emergence and rap- Corbella X, Montero A, Pujol M, et al. Emergence and rapid spread of carbapenem resistance during a large and sustained hospital outbreak of multiresist-ant Acinetobacter baumannii. J Clin Microbial 2000;38:4086-95.
14. 5. Manikal VM, Landman D, Saurina G, Oydna E, Lal H, Quale J. Endemic carbapenem-resistant Aci-netobacter species in Brooklyn, New York: citywide prevalence. Interinstitutional spread and relation to antibiotic usage. Clin Infect Dis 2000;31:101-6.
15. Kuo LC, Yu CJ, Lee LN, et al. Clinical features of pandrugresistant Acinetobacter baumannii bacteremia at a university hospital in Taiwan. J Formos Med Assoc 2003;102:601- 6.
16. Wang SH, Shengy WH, Chang YY, et al. Healthcare-asso- Wang SH, Shengy WH, Chang YY, et al. Healthcare-associated outbreak due to pan-drug resistant Acineto-bacter baumannii in a surgical intensive care unit. J Hosp Infect 2003;53:97-102.
17. Mahgoub S, Ahmed J, Glatt AE. Completely resist-ant Aci- Mahgoub S, Ahmed J, Glatt AE. Completely resist-ant Acinetobacter baumannii strains. Infect Control Hosp Epidemiol 2002;23:477-9.
18. Koeleman JG, Parlevliet GA, Dijkshoorn L, Savelkoul PH, Vandenbroucke-Grauls CM. Nosocomial outbreak of multiresistant Acinetobacter baumannii on a surgi -cal ward: epidemiology and risk factors for acquisition. J Hosp Infect 1997;37:113-23.
19. Simor AE, Lee M, Vearncombe M, et al. An outbreak due to multiresistant Acinetobacter baumannii in a burn unit: risk factors for acquisition and management. Infect Control Hosp Epidemiol 2002;23:261-7.
20. Gupta N, Yadav A, Saini S, et al. Biotyping and resisto- Gupta N, Yadav A, Saini S, et al. Biotyping and resistogram of Acinetobacter spp. in a tertiary care hospital. J Infect Dis Antimicrob Agents 2002;19: 57-61.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





