IJCRR - 7(10), May, 2015
Pages: 39-42
Print Article
Download XML Download PDF
VISUAL OUTCOME AND COMPLICATIONS OF NEODYNIUM : YTTRIUM ALUMINIUM GARNET LASER POSTERIOR CAPSULOTOMY IN PSEUDOPHAKIC PATIENTS USING SPIRAL METHOD OF CAPSULOTOMY
Author: Garima Agrawal
Category: General Sciences
Abstract:Aim: To determine the visual outcome and complications of Neodynium : Yttrium Aluminium Garnet laser posterior capsulotomy in pseudophakic patients with visually significant posterior capsular opacification using the spiral method of capsulotomy. Material and Methods: Neodynium : Yttrium Aluminium Garnet laser posterior capsulotomy was done in a spiral fashion in 50 eyes of 50 patients with visually significant posterior capsular opacification. The visual outcome and complications were documented 1week, 4 weeks and 12 weeks after the procedure. Observations: 94% patients had good visual recovery (best corrected visual acuity >/=6/12) 12 weeks post laser. The complicationsobserved were intraocular lens pitting in 6 eyes but was not significant to reduce vision. Intraocular pressure spike greater than 5 mm Hg was seen in 3 eyes 1 hour post laser but was controlled with anti -glaucoma medication. Cystoid macular edema was seen in 2 eyes, 8 and 10 weeks after laser. Conclusion Neodynium : Yttrium Aluminium Garnet laser posterior capsulotomy with the spiral method is effective in cutting the posterior capsule with good visual results and low rate of complications in our Institute.
Keywords: Neodynium: Yttrium Aluminium Garnet posterior capsulotomy, Visual outcome, Complications
Full Text:
INTRODUCTION
In the age where the femtosecond laser is being used for anterior capsulotomy in cataract surgery, we revisit the cold cutting laser i.e. Neodynium : Yttrium Aluminium Garnetlaser. Posterior capsular opacification is the most common delayed complication following cataract surgery.1 Neodynium: Yttrium Aluminium Garnet laser posterior capsulotomy is the standard treatment of posterior capsular opacification.2,3 The ND YAG laser offers a safe ,non invasive method of cutting the posterior capsule with good visual outcomes. Complications as rise in intra ocular pressure, cystoid macular edema and retinal detachment have been reported after the procedure.4,5A number of ways have been used to minimize energy delivery into the eye and minimize complications of the procedure. These include accurate focussing, cutting across tension lines along with a number of ways for cutting the posterior capsule including cross technique, can opener, inverted U, circular and spiral.6,7The present study aims at determining the visual outcome and complications of Neodynium : Yttrium Aluminium Garnet laser posterior capsulotomy in our Institute using spiral method of capsulotomy.
AIM
To determine the visual outcome and complications of Neodynium : Yttrium Aluminium Garnet laser posterior capsulotomy in pseudophakic patients with visually significant posterior capsular opacification using the spiral method of capsulotomy
MATERIAL AND METHODS
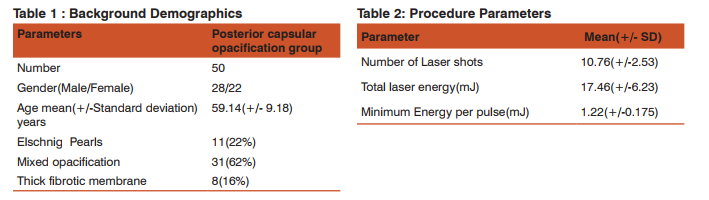
Fifty pseudophakic eyes of fifty cases (28males) and (22 Females) with visually significant posterior capsular opacification were enrolled . The study was carried out at our regional Institute of Ophthalmology from April 2014 to September 2014.The study is a prospective observational study. Ethical approval was obtained from the institutional review board. Informed consent was obtained from each enrolled subject for the procedure. The mean age (+/-SD) was 59.14+/-9.18 years(range 35-77 years). These cases had different types of PCO Elschnig pearls, mixed type and thick fibrotic membrane type.(Table I). All patients with corneal opacities, corneal edema, active intraocular inflammation, cystoid macular edema, retinal detachment, high myopia, lattice degeneration and history of retinal detachment in the fellow eye and other ocular comorbidities were excluded from the study. The meantime from cataract surgery was 22.42+/-16.32 months (range: 6–68). All patients were examined before Neodynium: Yttrium Aluminium Garnet laser capsulotomy and 1week, 4weeks, and 12 weeks after Nd: YAG laser capsulotomy. All patients underwent a complete ocular examination on all visits, including bestcorrected visual acuity, refraction, slit-lamp, intraocular pressure measurement, and posterior segment examination. Intraocular pressure was measured one hour after the laser. Tropicamide 1% and phenylephrine 2.5% were administered for pupillary dilatation prior to procedure. The capsulotomy size was kept slightly larger than the size of the mesopic pupil.The VISULAS II plus Q switched Neodynium: Yttrium Aluminium Garnet laser (Carl Zeiss Germany)was used. The capsulotomy was done in a spiral fashion. After capsulotomy, prednisolone acetate 1% four times daily and timolol maleate 0.5% eye drops twice daily for 15 days were prescribed. The chi square test was used for statistical analysis. p<0.05 was taken as significant
Observations and Results
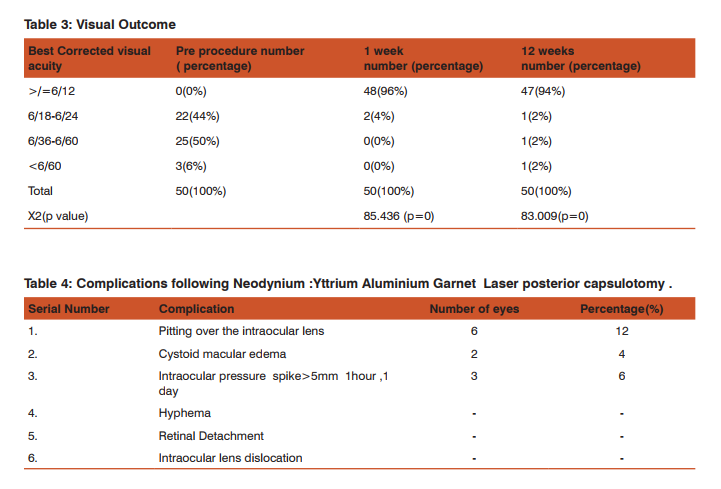
Table I shows the Background demographics. The mean age was 59.14(+/-9.18) years. Majority (62% ) patients had the mixed type of opacification (including pearls and fibrosis).28 were male and 22 patients were female. Table II shows the procedure parameters. The mean (+/-standard deviation ) total laser energy used was 17.46+/-6.23mJ.Table III shows the visual outcome.96 % patients had >/= 6/12 best corrected visual acuity one week post laser and 94%patients 3 months post laser. The p value is 0 i.e. <0.05 and hence the post laser visual acuity change is significant. One patient showed long term decrease of visual acuity of one line due to regression to posterior capsular opacification .The good visual results reflect the effectiveness of the procedure as well as good patient selection as we excluded patients with other ocular co morbidities. Table IV shows the complications of the procedure. Pitting over the intraocular lens was seen in 6(12%) patients, cystoid macular edema in 2(4%) patients and an intraocular pressure spike greater than 5 mm Hg in 3(6%) patients. Cystoid macular edema was the cause of poor visual recovery in two patients(BCVA <6/36).It was diagnosed on fundus examination and posterior segment optical coherence tomography and treatment started with topical nepafenac 0.1% four times a day and a posterior subtenon injection of 20mg Triamcinolone acetonide at our centre. Three patients had an IOP spike greater than 5mm Hg 1 hour,1 day post laser. The IOP was controlled and returned to baseline at I week with anti- glaucoma medication
DISCUSSION
Neodynium: Yttrium Aluminium Garnet laser is the standard treatment for posterior capsular opacification with good visual results. Jung KM et al have reported that the mean post procedural best corrected visual acuity was found to be 0.22±0.26 and procedural outcome showed 96 % (74 eyes out of the 77 eyes) enhancement in patients’ visual acuity.7In our study 94% patients had improvement in visual acuity 3 months post laser. We report high percentage of good visual results as all patients with other ocular co morbidities which may cause diminution of vision were excluded from the study. The procedure is not without its complications. Reported complications include damage to the intraocular lenses . 8,9We report pitting of the intraocular lens in 12 % of patients but it was not significant enough to cause diminution of vision. Increase in intraocular pressure, cystoid macular edema and disruption of the anterior vitreous face are also documented.4,10,11,12Three patients had a spike of intraocular pressure >5 mm Hg 1 hour,1 day post laser which was successfully treated with anti- glaucoma medication. Cystoid macular edema was seen in two of our patients 8weeks and 10 weeks after laser. Increased incidence of retinal detachment has been reported after the procedure.4,13,14,15,16,17 ,18In our study retinal detachment was not observed. A good patient selection and exclusion of high risk patients may account for low incidence of retinal detachment. We conclude that the spiral method of capsulotomy could be performed relatively safely with good visual recovery with low rate of complications using accurate focusing, proper technique and good patient selection.
Randomized controlled trials to compare two /several techniques of opening the posterior capsule are warranted to know the superiority of one method over the other.
CONCLUSION
Neodynium : Yttrium Aluminium Garnet laser posterior capsulotomy with the spiral method is effective in cutting the posterior capsule with good visual results and low rate of complications in our Institute. Good patient selection, accurate focusing and proper technique are cornerstones to maximize procedure results.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Aslam TM, Devlin H, Dhillon B. Use of Nd:YAG laser capsulotomy. Surv Ophthalmol 2003;48(6):594-612.
2. Aron Rosa D, Aron JJ, Griesemann M, Thyzel R. Use of neodymium yag laser to open the posterior capsule after lens implant surgery: a preliminary report. Am Intraoc Implant Soc Journal 1980;6(4):352-354.
3. Frankhauser F, Roussel P, Steffen J. Clinical studies on the efficiency of high power laser radiation upon some structures of the anterior segment of the eye. First experiences of the treatment of some pathological conditions of the anterior segment of the human eye by means of a Q-switched laser system .Int Ophthalmol 1981;3(3):129-139.
4. Steinert RF, Puliafito CA, Kumar SR, Dudak SD, Patel S. Cystoid macular edema, retinal detachment, and glaucoma after Nd:YAG laser posterior capsulotomy. Am J Ophthalmol1991;112(4):373-380.
5. Channel MM, Beckman H. Intraocular pressure changes after neodymium-YAG laser posterior capsulotomy. Arch ophthalmol 1984;102(7):1024-1026.
6. M Vella,S Wickhermansinghe, N Gupta, P Andreou, A Sinha.YAG laser capsulotomy, an unusual complication. Eye2009;18:193-194.
7. Jung KM, Jae HA, Jim HY.A new technique for Nd YAG laser posterior capsulotomy. Int J Ophthalmol 2014;7(2):345- 349.
8. Newland TJ, McDermott ML, Eliott D, Hazlett LD, Apple DJ, Lambert RJ, Barrett RP. Experimental neodymium:YAG laser damage to acrylic, poly(methyl methacrylate), and silicone intraocular lens materials. J Cataract Refract Surg 1999;25(1):72–76.
9. Trinavarat A, Atchaneeyasakul L, Udompunturak S. Neodymium:YAG laser damage threshold of foldable intraocular lenses. J Cataract Refract Surg 2001;27(5):775– 780.
10. Ge J, Wand M, Chiang R, Paranhos A, Shields MB. Longterm effect of Nd:YAG laser posterior capsulotomy on intraocular pressure. Arch Ophthalmol 2000;118(10):1334– 1337.
11. Krauss JM, Puliafito CA, Miglior S, Steinert RF, Cheng HM. Vitreous changes after neodymium-YAG laser photodisruption. Arch Ophthalmol 1986;104(4):592–597.
12. Bath PE, Fankhauser F. Long-term results of Nd: YAG laser posterior capsulotomy with the Swiss laser. J Cataract Refract Surg 1986;12(2):150–153.
13. Dardenne MU, Gerten GJ, Kokkas K, Kermani O. Retrospective study of retinal detachment following neodymium: YAG laser posterior capsulotomy. J Cataract Refract Surg 1989;15(6):676–680.
14. Javitt JC, Tielsch JM, Canner JK, Kolb MM, Sommer A, Steinberg EP. National outcomes of cataract extraction. Increased risk of retinal complications associated with Nd:YAG laser capsulotomy. The Cataract Patient Outcomes Research Team. Ophthalmology 1992;99(10):1487–1498.
15. Powell SK, Olson RJ. Incidence of retinal detachment after cataract surgery and neodymium:YAG laser capsulotomy. J Cataract Refract Surg 1995;21(2):132–135.
16. Shah GR, Gills JP, Durham DG, Ausmus WH. Three thousand YAG lasers in posterior capsulotomies: an analysis of complications and comparison to polishing and surgical discission. Ophthalmic Surg 1986;17(8):473–477.
17. Nielsen NE, Naeser K. Epidemiology of retinal detachment following extracapsular cataract extraction: a follow-up study with an analysis of risk factors. J Cataract Refract Surg 1993;19(6):675–680.
18. Hayashi K, Nakao F, Hayashi H. Influence of size of neodymium:yttrium-aluminium-garnet laser posterior capsulotomy on visual function. Eye 2010;24(1):101–106.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





