IJCRR - 10(21), November, 2018
Pages: 07-13
Date of Publication: 15-Nov-2018
Print Article
Download XML Download PDF
Pharmacoepidemiological Study of Gynecological Disorders Among Women in Community Setup
Author: Naga Lekhini Ravi, Pravallika Kasula, Madhu Latha Gurram, Shafiya Begum Shaik
Category: Healthcare
Abstract:Background: Gynecological problems are universal in occurrence. Lack of awareness about various gynecological problems, economic and social barriers, delay the early diagnosis of the gynecological problems. In order to understand and to create awareness about gynecological problems this study was undertaken.
Materials and Methods: Observational cross sectional study was conducted in the community settings (In and around Guntur) by taking samples randomly for a period of 6 months i.e., from October 2017- March 2018. Subjects were selected based on inclusion and exclusion criteria and Patients were informed about study and obtained Informed Consent Form (ICF). The data was collected by using a self administered questionnaire. Subjects were educated on their disease by verbal and also by providing patient information leaflets.
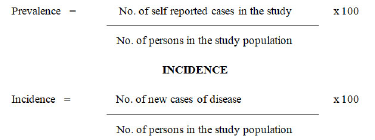
Results: Out of 5000 subjects, only 826 subjects met the inclusion criteria. Incidence (3.44%) and prevalence (4.6%) of abnormal uterine bleeding was high among all gynecological related problems followed by urinary tract infections in the age group between 26-35 years.
Conclusion: There was a high prevalence (4.6%) and incidence (3.44%) of abnormal uterine bleeding among other gynecological problems. Generally urinary tract infection is self limiting, so by educating about medication usage, lifestyle modification, medication adherence and by providing patient information leaflets we observed there was a reduction in symptoms. Finally from the study we concluded that awareness plays a significant role in decreasing disease progression, complications and thereby reducing the economic burden
Keywords: Abnormal uterine bleeding, Awareness, Gynecological problems, Incidence and prevalence
Full Text:
INTRODUCTION:
Epidemiology is the “study of the distribution and determinants of health-related states or events in a specified population and the application of this study is to control diseases and other health problems”. [1]
Aim of epidemiological studies was to control or eliminate diseases in the community.
Need of epidemiological studies:
-
In a typical Indian society, the health problems of women are often neglected more so the gynecological problems because women in their reproductive years prioritize the health of children, husband and other family members over their own.
-
Lack of awareness about various gynaecological problems, economic and social barriers, delay the early diagnosis of the gynecological problems.
-
In recent years it has been observed that improper awareness on a disease or a condition is leading to more number of surgeries or complications.
-
Infertility is also being reported in a very high rate which always has any other gynecological disorder as an underlying problem.
-
This study is performed to find out the incidence and prevalence of gynecological problems in community setup. So, that complication can reduce and prevention can be done effectively.
A gynecological disorder is a condition which affects the female reproduction organs, namely the breasts and organs in the abdominal and pelvic area including the womb (uterus), ovaries, fallopian tubes, vagina and vulva.[2]
Every women in her life time will suffer with a gynecological condition and most of them will be minor and treatable and some conditions leads to devasting consequences-impacting their ability to have a children and sometimes threatens their life when the condition become severe.
Uterine Fibroids, Urinary Tract Infection(UTI), Ovarian Cysts, Polycystic Ovarian Syndrome (PCOS), Pelvic Inflammatory Disease (PID), Dysmenorrhea, Menorrhagia, Oligomenorrhea, Amenorrhea, Abnormal Uterine Bleeding(AUB) etc. are some of the most common reproductive problems.
MATERIALS AND METHODS
MATERIALS USED:
-
Patient consent form
-
Self administered questionnaire
-
Prescriptions and case records
-
Patient information leaflets
METHODOLOGY:
STUDY DESIGN: Observational Cross Sectional Study
STUDY PERIOD: The study was carried out for a period of 6 months i.e., from October 2017- March 2018.
SAMPLE SIZE: Total of 826 subjects who are diagnosed with various gynecological problems.
INCLUSION CRITERIA:
-
Patients who are willing to participate and who meets the study criteria.
-
All female subjects above 18 years to 45 years of age who are with gynecological disorders.
-
Patients diagnosed with Polycystic Ovarian Syndrome, Menorrhagia, Amenorrhea, Fibroid uterus, Urinary tract infection which are new or known cases.
EXCLUSION CRITERIA:
DATA COLLECTION:
-
The study was conducted in the community settings (In and around the Guntur) by taking the samples randomly.
-
Subjects were selected based on inclusion and exclusion criteria and Patients were informed about study and obtained Informed Consent Form (ICF).
-
The data was collected by using a self administered questionnaire.
-
Subjects were educated on their disease by verbal and also by providing patient information leaflets.
-
All the materials (Patient information leaflets, data collection form) validated by Head of the department(HOD) of gynecology department, Government General Hospital (GGH), Guntur.
-
Follow up was planned for urinary tract infection since it has a chance of recurrence and can be effectively treated with medication and life style modifications.
STATISTICAL ANALYSIS:
Data was statistically analyzed using SPSS 22.00 software and Ms Office Excel worksheet.
Paired t- test was used for follow ups, the significance value was tabulated as p<0.05.
RESULTS
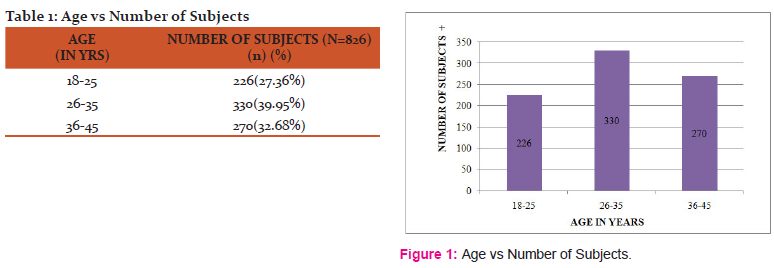
Table 1 depicts the information regarding distribution of subjects within age groups of 18-45years. Majority of subjects were found within 26-35yrs 330 (39.95%) followed by 36-45yrs 270 (32.68%) and 18-25yrs 226 (27.36%) which is graphically represented in figure 1.
Table 2 depicts the information regarding distribution of subjects based on level of education. Majority of subjects were illiterate 260 (31.48%) followed by less than 5th standard 212 (25.66%), 5th to 10th standard 162 (19.61%), intermediate 112(13.56%) and degree 80 (9.68%) which is graphically represented in figure 2.
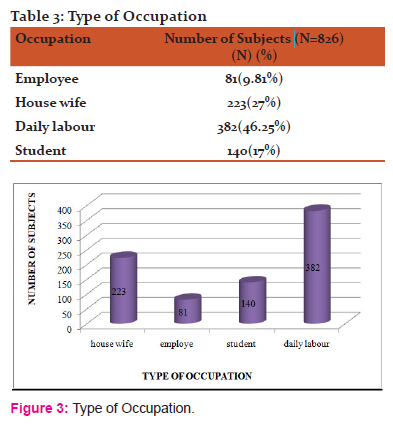
Table 3 depicts the information regarding distribution of subjects based on type of occupation. Majority of subjects were daily labors 382 (46.25%) followed by house wives 223 (27%), students 140(17%) and employees 81(9.81%) which is graphically represented in figure 3.
Table 4 depicts the information regarding distribution of subjects based on marital status. Majority of subjects were married 562 (68.03%) followed by single 176 (21.30%) and divorced 88 (10.65%) which is graphically represented in figure 4.
Table 5 depicts the information regarding distribution of subjects based on gap between pregnancies. Majority of subjects were having 1year gap 274 (33.17%) followed by 1-2years 242 (30%), infertility and one child 170 (20.6%), 2-3years 90 (11%) and more than 3years 50 (6.05%) which is graphically represented in figure 5.
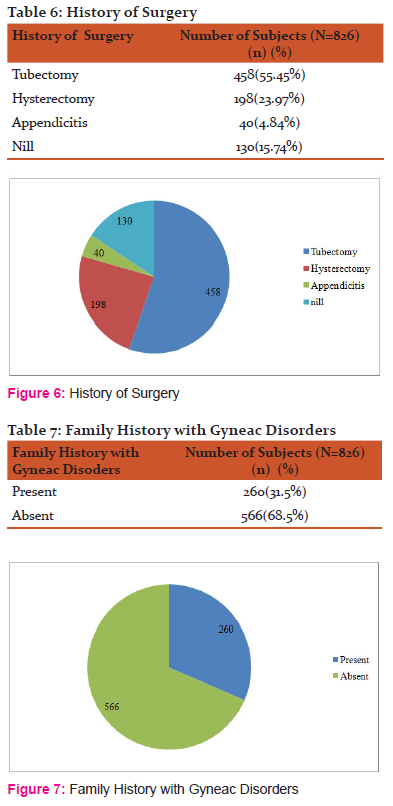
Table 6 depicts the information regarding distribution of subjects based on history of surgery. Majority of subjects were underwent tubectomy 458 (55.45%) followed by hysterectomy 198 (23.97%), without any surgery 130 (15.74%) and appendicitis 40 (4.84%) which is graphically represented in figure 6.
Table 7 depicts the information regarding distribution of subjects based on family history with gyneac disorders. Majority of subjects were not having family history 566 (68.5%) followed by having family history 260 (31.5%) which is graphically represented in figure 7.
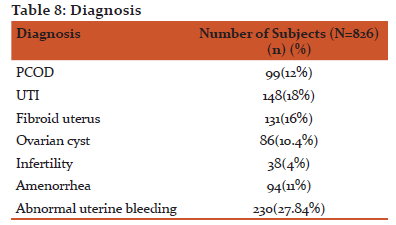
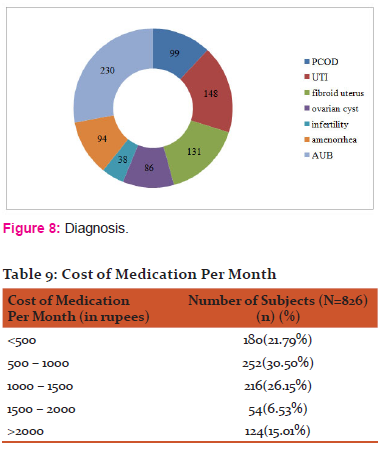
.Table 8 depicts the information regarding distribution of subjects based on diagnosis. Majority of subjects were diagnosed with Abnormal uterine bleeding 230 (27.84%), followed by UTI 148 (18%), Fibroid uterus 131 (16%), PCOD 99 (12%), Amenorrhea 94 (11%), Ovarian cyst 86 (10.4%) and Infertility 38 (4%) which is graphically represented in figure 8.
Table 9 depicts the information regarding distribution of subjects based on cost of medication per month. Majority of subjects were spending 500 – 1000 rupees 252 (30.50%) followed by 1000 – 1500 rupees (26.15%), less than 500 rupees 180 (21.79%), more than 2000 rupees 124 (15.01%) and 1500 – 2000 rupees 54 (6.53%) which is graphically represented in figure 9.
FORMULA USED TO CALCULATE INCIDENCE AND PREVALENCE OF GYNECOLOGICAL DISORDERS
PREVALENCE
DISCUSSION
An observational cross sectional epidemiological study on gynecological disorders among women in community setup was conducted among women within the age group of 18-45 yrs who are diagnosed with different gynecological problems. Total of 826 subjects met the inclusion criteria and were included in the study. The data obtained was tabulated and analyzed.
In our study we found that majority of subjects who are suffering with gynecological disorders are in between the age groups of 25-36 years. Based on results obtained our study revealed that the prevalence of menstrual problems more when compared to other gynecological disorders. This result was in concordance with the study done by Harlow ZD, Campbell OM (2004) which showed that prevalence of abnormal uterine bleeding was higher and it is the major cause of gynecological morbidity. [3]
In our study we found that majority of subjects who are Illiterates (31.48%) are facing more gynecological related problems because of poor knowledge, do not seek health care until it becomes an emergency, lack of decision making power because of education and less number of subjects who are highly educated (9.68%) were reported less gynecological related problems because of knowledge, revealed their gynecological related problems by excluding social barrier and decision making power. This result was in concordance with the study done by Dheresa M, Assefa N, Berhane Y, Worku A, Mingiste B, Dessie Y (2017) which showed that gynecological morbidity was associated with illiteracy, lack of decision making power, parity, early marriage and age.[4]
In our study we found that majority of subjects who are daily labours (46.25%) are facing more gynecological related problems because of low economy, education level, poor knowledge and subjects who are employees (9.81%) are facing less gynecological related problems because of knowledge, socio-economic status. This result was in concordance with the study done by Poornima S, Katti SM, Mallap UR, Vihay M (2013) which showed that 52.25% of house wives are facing reproductive problems followed by subjects involved in production work (21.25%) and concluded that there is no association of gynecological problems with the education, socio-economic status and age.[5]
Our study also revealed that prevalence of gynecological problems among the married women in the reproductive age group is high. This result was in concordance with the study done by Poornima S, Katti SM, Mallap UR, Vihay M (2013) which showed that prevalence of gynecological problems among the married women in their reproductive age group of urban Belgaum is moderately high.[5]
In our study we found that majority of subjects who are with short interbirth interval (i.e 1 year [33.17%]) were facing more problems because of decreased hormone levels and decreased body strength. This result was in concordance with the study done by Abdel-Fattah M, PhD, Hifnawy T PhD, El Said TI MD, Moharam MM MD, Mahmoud MA MRCOG (2007) which showed that Short interbirth interval is due to girl child birth and effects the health of women. [6]
In our study we found that majority of subjects are facing reproductive problems after tubectomy (55.45%) because of Post Tubal Ligation Syndrome (PTLS) followed by hysterectomy (23.97%) due to hormonal imbalance. PTLS means physical (menstrual pattern changes, painful periods, hot flashes) and mental changes (depression, anxiety) after tubectomy. This result was in concordance with the study done by Jahanian Sadatmahalleh SH, Ziael S, Kazemnejad A, Mohamadi E (2016) which showed that Tubal Ligation (TL) or tubectomy is a cause of menstrual disorders. [7]
In our study we found that family history (31.5%) also plays a key role in developing gynecological related problems. This result was in concordance with the study done by Acheson LS MS MD, Wang C MSc, PhD, Zyzanski SJ, PhD, Lynn A PhD, Ruffin MT IV, MD, MPH, Gramling R MD DSc et al. (2010) which showed that having a family history of a disease increases its salience and does not change one's perceived ability to prevent the disease.[8]
In our study we found that subjects are spending 500-1000 rupees (30.50%) to purchase medications per month followed by 1000-1500/month (26.15%) and subjects are not coming for regular follow up (8.95%) due to low economy, busy work.
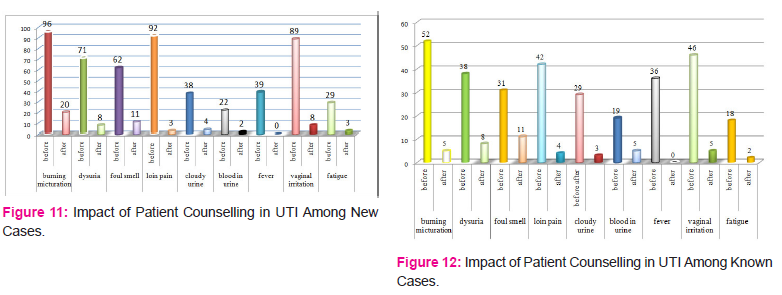
Our study also revealed that burning micturition (100%) was the most common UTI symptom followed by loin pain (90.5%). This result was in concordance with the study done by Pradhan R, Mathur RK, Mathur P, Gupta A, Chowhan M (2012) which showed that burning micutrition was the most common urinary complaint followed by increasing frequency of micturition.[9]
CONCLUSION
Based on the results obtained, our study concluded that incidence (3.44%) and prevalence (4.6%) of abnormal uterine bleeding was higher among other gynecological problems and it effects women health status, quality of life and social integration. Generally urinary tract infection is self limiting, so by educating about medication usage, lifestyle modification, medication adherence and by providing patient information leaflets we observed there was a reduction in symptoms. It is suggested that menstrual complaints should be thoroughly evaluated and treated on top priority. Finally from the study we concluded that awareness plays a significant role in decreasing disease progression, complications and reducing the economic burden.
FUNDING: No funding resources
CONFLICT OF INTEREST: None declared



References:
1. Sistey J Moshi. Epidemiology in Gynecological Diseases- https://www.glowm.com/pdf/Chap-33_Moshi.pdf [Cited 26 December 2017].
2. Gynecological disorders- https://www.omicsonline.org/scholarly/gynecological-disorders-journals-articles-ppts-list.php [Cited 9 November 2017].
3. Harlow SD, Campbell OM. Epidemiology of menstrual disorders in developing countries: a systematic review. Int J Gynaecol Obstet 2004 Jan; 111(1):6-16.
4. Dheresa M, Assefa N, Berhane Y, Worku A, Mingiste B, Dessie Y. Gynecological Morbidity among Women in Reproductive Age: A Systematic Review and Meta- Analysis. J Women’s Health Care 2017 May 26: 367. dio: 10.4172/2167-0420.1000367.
5. Poornima S, Katti SM, Mallapur, Vinay M. Gynecological problems of married women in the reproductive age group of urban Belgaum, Karnataka. Al Ameen J Med Sci 2013; 6(3): 226-230.
6. Abdel-Fattah M, PhD, Hifnawy T PhD, El Said TI MD, Moharam MM MD, Mahmoud MA MRCOG. Determinants of birth spacing among Saudi women. J Family Community Med 2007 Sep-Dec; 14(3): 103-111.
7.Jahanian Sadatmahalleh SH, Ziael S, Kazemnejad A, Mohamadi E. Menustrual pattern following tubal ligation: a historical cohort study. Int J Fertil Steril.2016;9(4): 477-482.
8. Acheson LS MS MD, Wang C MSc, PhD, Zyzanski SJ, PhD, Lynn A PhD, Ruffin MT IV MD MPH, Gramling R MD DSc et al. Family history and perceptions about risk and prevention for chronic diseases in primary care: A report from the Family Healthware Impact Trial. Genet Med 2010 Apr; 12(4): 212-218.
9. Pradhan R, Mathur RK, Mathur P, Gupta A, Chowhan M. Study of Common Urinary Problems of Females at a Government Hospital in Central India. Scientific Research 2012 May 17; 3(6): 339-343.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





