IJCRR - 2(6), June, 2010
Pages: 32-42
Print Article
Download XML Download PDF
PHYSICIANS PRESCRIBING PATTERNS OF ORAL ANTIDIABETIC DRUGS
Author: Sreedhar D, Virendra SL, Manthan J, Ajay P, Prashanth M Udupa N
Category: Healthcare
Abstract:Physicians prescribing pattern of oral antidiabetic drugs may be key to avoid the serious complications of patients suffering from type 2 diabetes. However, fixed dose combinations were often prescribed to achieve target glycemic levels. Treatment complexity can be reduced by prescribing a fixed dose combination of two or more oral antidiabetic drugs. There are good numbers of studies which suggest the use of fixed dose combinations not only to reduce the complications of diabetes but also to improve adherence. A variety of fixed dose combination oral antidiabetic drugs in different dosage strengths are available and the strategies for selecting such fixed dose combinations options depends on physicians prescribing behavior and patients condition. This article describes the increasing preference of physicians to prescribe fixed dose combinations of oral antidiabetic drugs.
Keywords: Fixed dose combinations, oral antidiabetic drugs, physicians prescribing pattern.
Full Text:
Introductions
To understand the intricacies behind the current diabetes practice in India, it is important, to understand the physician's perceptions, attitudes and practices1 . Several studies suggest the use of combination of two or more antidiabetics drugs with different mechanism of action for the management of hyperglycemia in type 2 diabetes patients. A few studies demonstrate the comparison of low dose fixed dose combinations vs high dose single component products, a few studies describe the safety and efficacy of FDCs, a few studies did a comparative evaluation of monotherapy, combination therapy and fixed dose combination therapy and a few studies have stated the medication adherence and health related costs in type 2 diabetic patients2-26 . As many fixed dose combinations containing two or more oral antidiabetics drugs are available in the market, physicians are preferring to prescribe. Physicians prescribing preference is may be due to convenience, reduced pill burden or may be due to simplified regimen and the range of dosage strengths which allow flexible dose titration. There are a few studies which also describe the complexities associated with fixed dose combinations of oral antidiabetic drugs apart from their advantages27 .
Use of insulin in combination with Oral Antidiabetic Drugs (OADs) is also gaining importance. There are handful of studies and guidelines which recommend use of insulin in combination with OADs. It has been observed that 30 to 40% of patients can achieve the glycemic targets by combination of once daily premix insulin with OADs. However, the therapy needs to be intensified with the decline of ß-cell function (= insulin secretion) as disease progresses. In this case premix insulin should be scaled up to twice and thrice daily with or without one or multiple class of OADs. Premix insulin can be combined with insulin sensitizers and secretagogues when initiated once daily, nonetheless, OADs can be continued with twice and thrice daily premix insulin therapy.
Objectives of the study
To understand the physicians prescribing patterns with respect to Oral antidiabetic drugs. Survey was carried out among the physicians to mainly understand the following aspects:
- Frequency of fixed dose combination prescriptions
- Conditions for which FDCs were usually preferred
- Preferred oral antidiabetic fixed dose combinations
- Reasons for prescribing FDCs
Research Methodology
Research Design
Information with regard to the prescribing pattern of fixed dose combinations of antidiabetic drugs was collected. This information would give an idea whether physicians prefer to prescribe fixed dose combinations, if so in which conditions and their experiences on such combinations.
Research Type
Research type was exploratory. Exploratory research was conducted after thorough search of secondary data available.
Questionnaire Method
Questionnaire technique was followed to collect the information from the respondents. Questionnaire was developed in such a way that the respondents could answer the questions with ease. Effort was put to reduce the number of questions so that the respondents take less time to answer the questions as the respondents were physicians. Structured direct survey method was adopted for collecting the information from the respondents. A direct approach was pursued as the purpose of the study was disclosed or was obvious to the respondents. Questionnaire consisted of mostly fixed alternative questions (Multiple choice and dichotomous), where the respondent has to select from predetermined alternatives. There were a few unstructured open ended questions for which the respondents had to write down the answers. Apart from the basic information i.e the information related to the direct research problem, classification information, consisting of socioeconomics and demographic was also collected. Pretesting of the questionnaire was done in small sample of respondents (n=10) and possible errors were eliminated. After elimination of the errors, questionnaire was drafted and the responses were collected.
Sampling
Sampling design was done keeping in mind the target population. The target population was physicians who prescribe antidiabetic drugs. Information about prescription preference of fixed dose combination was collected. Study was carried out in five places namely Bangalore, Cochin, Hyderabad, Mangalore, Manipal and Udupi. Nonprobability sampling technique was adopted where it was decided arbitrarily which elements to be included in the sample. Convenience sampling was chosen, study units that happen to be available at the time of data collection were selected in the sample. Initial target sample size was 80. 20 each from Bangalore, Cochin, Hyderabad and 20 from Mangalore, Manipal and Udupi put together. Final sample size used for evaluation was 60. 20 questionnaire responses were not considered for evaluation as there were some incomplete responses. The sample was selected on pragmatic criteria. Respondents in the study were General Practitioners, Diabetologists and endocrinologists.
Inclusion/Exclusion Criteria
Physicians prescribing antidiabetic irrespective of their specialization were included in the study and the physicians having practice less than 5 years were excluded from the study.
Results and Discussion
Specialization and average duration of practice of 62 doctors is summarized in the table 1. Out of 62 doctors, fifty one were general physicians who were treating mostly diabetic patients, nine diabetologists and two endocrinologists. The average duration of practice was 14.5 years; general physicians (17.8), diabetologists (12.9) and endocrinologist (12.5).

Less duration of practice with respect to diabetologists and endocrinologist was probably because of the fact that diabetes became a super specialty only recently.
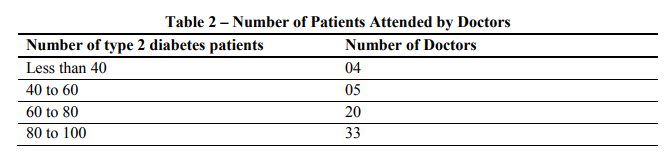
It is evident that 53% of physicians see between 80 to 100 patients with type 2 diabetes in a month, followed by 32% in the range of 60-80. Only a very few physicians (6%) see less than 40 patients respectively. This gives a rough picture about number of individuals suffering from type 2 diabetes.
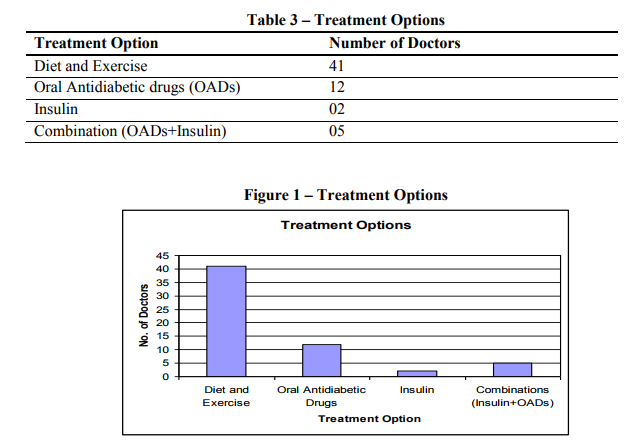
Non pharmacological treatment was preferred by most physicians (85%) soon after the patients were diagnosed with type 2 diabetes. Total of 12% doctors prescribe OADs and few doctors prescribe insulin (2) and combination of OAD and Insulin (5). Although most of the doctors preferred diet and exercise and Oral Anti-diabetic drugs, insulin initiation and combination of insulin and OADs cannot be neglected. There was one study conducted in Urban and Semi urban Bangalore district, where less number physicians were opting for nonpharmacological treatment (Rayappa PH, Raju KNM, Kapur A. Personnel communication) contradictory to the present study results. It was observed that most respondents (85%) approach was more aggressive when patients were not responding to nonpharmacological treatment or initial oral antidiabetic drugs. They were treating type 2 diabetes patients with all three options: diet and exercise, OADs and Insulin. This aggressive treatment approach by doctors might be due their experience in controlling blood glucose levels or they were made aware of how to lower the blood glucose levels effectively.
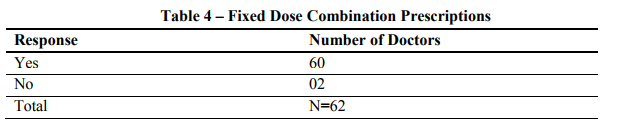
Most respondents (96%) of the study stated that they prescribe antidiabetic fixed dose combinations. Two responded in negative, one respondent commented that he was never impressed with the combinations available in the market and also read about the recent issues on irrationality of fixed dose combinations and another respondent reported that there is no need of prescribing fixed dose combinations and said most of the combinations are irrational in one way or the other. He also emphasized that, if one uses more drugs, there would be more side effects. Although majority of the respondents were prescribing FDCs, the irrational FDCs issue in the recent past may disturb the physicians' preference to prescribe FDCs in general. It is essential for the companies who manufacture FDCs to bring it to notice of the physicians that their combinations are rational and have been approved by Drugs Controller General of India (DCGI).
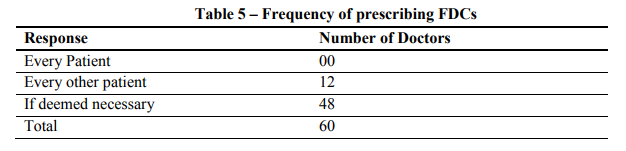
Most physicians (73%) reported that they would only prescribe antidiabetic fixed dose combination if deemed necessary for the patients suffering with type 2 diabetes. All patients with type 2 diabetes may not require to be treated with antidiabetic FDCs. It is essential to screen the blood glucose levels before prescribing antidiabetic fixed dose combinations.
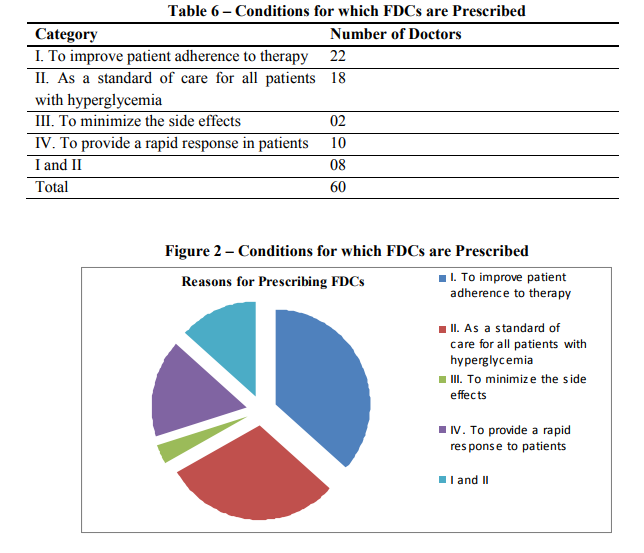
Most physicians (36%) who responded to the question affirmed that they prescribe FDCs to improve patient adherence to therapy and as a standard of care for all patients with hyperglycemia (30%). A few physicians (16%) stated that they prescribe FDCs to provide rapid response to the patients and only two physicians (3%) had stated they prescribe for minimizing the side effects.
Responses observed above are comparable with the advantages offered by fixed dose combinations.
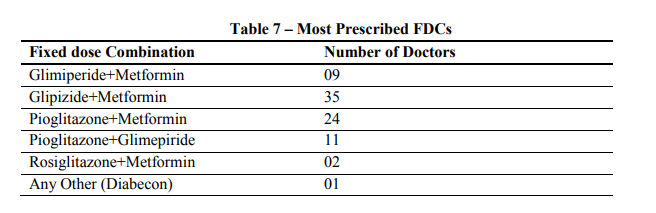
Majority of the doctors (44%) were prescribing Glipizide+Metformin combination followed by Pioglitazone+Metformin combination (29%). A few doctors were prescribing, Pioglitazone+Glimeperide (13%), Glimeperide+Metformin (11%) and Rosiglitazone+Metformin (2%) combinations. It was observed that one doctor is convinced of an herbal preparation and found improvement in disease status when prescribed as an adjuvant to an OAD. Although there are lots of antidiabetic fixed dose combinations available in the market, only a few combinations are mostly prescribed by the doctors.
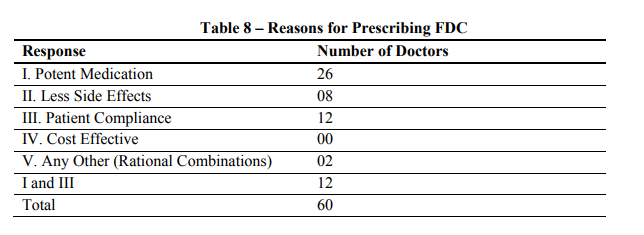
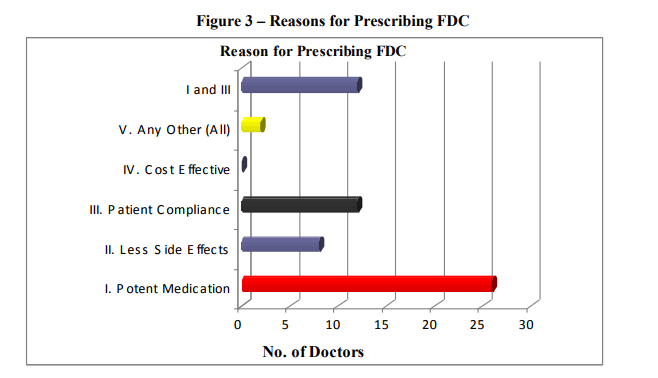
Most of the doctors had affirmed that pioglitazone+metformin and glipizide+metformin are very effective and the reason behind its effectiveness was potent medication. Not a single respondent have specified that they prescribe the combinations because of cost effectiveness. This shows the attitude of physicians towards cost of medicine and also gives an indication that they would overshadow the cost factor over other factors like effective drug, patient compliance and less side effects.
Conclusion
India is considered to be diabetes capital of the world and was even evident from the study where doctors were attending more than 80 patients in a month. Indians are more prone to develop diabetes due to life style and food habits. Moreover complications start at younger age. Consequently burden of uncontrolled diabetes in India is high with more than two third of the treated patients not achieving optimal glycemic control. This may be attributed to low purchasing power, inadequate access to health care facilities in remote areas of our country and most importantly diabetes patients are treated by general physicians who were not aware of guidelines which should be followed in Indian context. It was clear from the study that majority of the doctors were aggressive in treating diabetic patients by all possible means. It was observed that doctors start treatment with diet and exercise and then would prescribe OADs or put patients on Insulin.
Although new classes of medication and numerous combinations have been demonstrated to lower glycaemia, doctors were finding it difficult to achieve and maintain the optimal blood glucose levels. However, fixed dose combination antidiabetic drugs were being preferred by most of the respondents due to their advantages.
References:
1. Kapur A, Shishoo S, Ahuja MMS, Sen V, Mankame K. Diabetes Care in India: Physicians Perceptions Attitudes and Practices. Int J Diab Dev Countries. 1998;18:124-130.
2. Hays R, Kravitz R, Mazel R. et al. The impact of patient adherence on health outcomes for patients with chronic disease in the Medical Outcomes Study. Journal of Behavioral Medicine. 1994; 17: 347- 360.
3. Brown JB, Nichols GA, Glauber HS, Bakst A. Ten-year follow-up of antidiabetic drug use, nonadherence, and mortality in a defined population with type 2 diabetes mellitus. Clinical Therapeutics. 1999 Jun;21(6): 1045-1057.
4. Erle G, Lovise S, Stocchiero C. et al. A comparison of preconstituted, fixed combinations of low-dose glyburide plus metformin versus high-dose glyburide alone in the treatment of type 2 diabetic patients. Acta Diabetologica. 1999 Jun;36(12): 61-65.
5. Blonde L, Rosenstock J, Mooradian AD, Piper BA, Henry D. Glyburide/metformin combination product is safe and efficacious in patients with type 2 diabetes failing sulphonylurea therapy. Diabetes, Obesity and Metabolism. 2002 Nov;4(6): 368-375.
6. Garber AJ, Larsen J, Schneider SH, Piper BA, Henry D. Glyburide/Metformin Initial Therapy Study G. Simultaneous glyburide/metformin therapy is superior to component monotherapy as an initial pharmacological treatment for type 2 diabetes. Diabetes, Obesity and Metabolism. 2002 May;4(3): 201-208.
7. Garber AJ, Bruce S, Fiedorek FT. Durability of efficacy and long-term safety profile of glyburide/metformin tablets in patients with type 2 diabetes mellitus: an open-label extension study. Clinical Therapeutics. 2002 Sep;24(9): 1401- 1413.
8. Marre M, Howlett H, Lehert P, Allavoine T. Improved glycaemic control with metforminglibenclamide combined tablet therapy (Glucovance) in Type 2 diabetic patients inadequately controlled on metformin. Diabetic Medicine. 2002 Aug;19(8): 673-680.
9. Melikian C, White TJ, Vanderplas A, Dezii CM, Chang E. Adherence to oral antidiabetic therapy in a managed care organization: a comparison of monotherapy, combination therapy, and fixed-dose combination therapy. Clinical Therapeutics. 2002 Mar;24(3): 460- 467.
10. Schectman JM, Nadkarni MM, Voss JD. The association between diabetes metabolic control and drug adherence in an indigent population. Diabetes Care. 2002 Jun;25(6): 1015-1021.
11. Balkrishnan R, Rajagopalan R, Camacho F, Huston S, Murray F, Anderson R. Predictors of medication adherence and associated health care costs in an older population with type 2 diabetes mellitus: a longitudinal cohort study. Clinical Therapeutics. 2003; 25(11): 2958-2971.
12. Blonde L, Wogen J, Kreilick C, Seymour AA. Greater reductions in A1C in type 2 diabetic patients new to therapy with glyburide/metformin tablets as compared to glyburide coadministered with metformin. Diabetes, Obesity and Metabolism. 2003 Nov;5(6): 424-431.
13. Duckworth W, Marcelli M, Padden M. et al. Improvements in glycemic control in type 2 diabetes patients switched from sulfonylurea coadministered with metformin to glyburide-metformin tablets. Journal of Managed Care Pharmacy. 2003 May–Jun;9(3): 256-262.
14. Garber A, Marre M, Blonde L. et al. Influence of initial hyperglycaemia, weight and age on the blood glucose lowering efficacy and incidence of hypoglycaemic symptoms with a single-tablet metforminglibenclamide therapy (Glucovance) in type 2 diabetes. Diabetes, Obesity and Metabolism. 2003 May;5(3): 171- 179.
15. Garber AJ, Donovan DS Jr., Dandona P, Bruce S, Park J-S. Efficacy of glyburide/metformin tablets compared with initial monotherapy in type 2 diabetes. Journal of Clinical Endocrinology and Metabolism. 2003 Aug;88(8): 3598-3604.
16. Goldstein BJ, Pans M, Rubin CJ. Multicenter, randomized, doublemasked, parallel-group assessment of simultaneous glipizide/metformin as second-line pharmacologic treatment for patients with type 2 diabetes mellitus that is inadequately controlled by a sulfonylurea. Clinical Therapeutics. 2003 Mar;25(3): 890-903.
17. Grant RW, Devita NG, Singer DE. et al. Polypharmacy and medication adherence in patients with type 2 diabetes. Diabetes Care. 2003; 26: 1408-1412.
18. Krapek K, King K, Warren SS. et al. Medication adherence and associated hemoglobin A1c in type 2 diabetes. Annals of Pharmacotherapy. 2004 Sep;38(9): 1357-1362.
19. Lau DT, Nau DP. Oral antihyperglycemic medication nonadherence and subsequent hospitalization among individuals with type 2 diabetes. Diabetes Care. 2004 Sep;27(9): 2149-2153.
20. Vanderpoel DR, Hussein MA, Watson-Heidari T, Perry A. Adherence to a fixed-dose combination of rosiglitazone maleate/metformin hydrochloride in subjects with type 2 diabetes mellitus: a retrospective database analysis. Clinical Therapeutics. 2004 Dec;26(12): 2066-2075.
21. Bruce S, Park JS, Fiedorek FT, Howlett HCS. Beta-cell response to metformin-glibenclamide combination tablets (Glucovance) in patients with type 2 diabetes. International Journal of Clinical Practice. 2006 Jul;60(7): 783-790.
22. Mateo J, Gil-Guillen VF, Mateo E. et al. Multifactorial approach and adherence to prescribed oral medications in patients with type 2 diabetes. International Journal of Clinical Practice. 2006; 60: 422-428.
23. Rosenstock J, Rood JA, Cobitz AR, Biswas N, Chou H, Garber A. Initial treatment with rosiglitazone/metformin fixed-dose combination therapy compared with monotherapy with either rosiglitazone or metformin in patients with uncontrolled type 2 diabetes. Diabetes, Obesity and Metabolism. 2006; 8(6): 650-660.
24. Bangalore S, Kamalakkannan G, Parkar S, et al. Fixed-dose combinations improve medication compliance: a meta-analysis. Am J Med. 2007;120:713-9.
25. Chou HS, Palmer JP, Jones AR, Waterhouse B, Ferreira-Cornwell C, Krebs J, Goldstein BJ: Initial treatment with fixed-dose combination rosiglitazone/glimepiride in patients with previously untreated type 2 diabetes. Diabetes Obes Metab. 2007 Jul 21.
26. Bailey CJ, Day C. Fixed-dose single tablet antidiabetic combinations. Diabetes Obes Metab 2009; 11: 527-533.
27. Bailey CJ. Whence and whither the fixed-dose combination? Diabetes Vasc Dis Res. 2005; 2: 51-53.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





