IJCRR - 3(9), September, 2011
Pages: 96-102
Print Article
Download XML Download PDF
THE EFFECTIVENESS OF REPETITIVE BILATERAL LEG TRAINING IN IMPROVING LOWER EXTRIMITY MOTOR FUNCTION OF HEMIPARETIC ACUTE MIDDLE CEREBRAL ARTERY STROKE PATIENTS.
Author: Sasidharan Tapan, N. Rajeev
Category: Healthcare
Abstract:Objective: The objective of the study was to find the effectiveness of repetitive bilateral leg training on improving lower extremity motor functions of hemi paretic patients in the geriatric age group Methods: An experimental approach, with pre test and post test control group design was used. 30 acute middle cerebral artery(MCA) stroke patients were conveniently selected and randomly distributed in to group A and Group B. Group A received conventional physiotherapy and group B received repetitive bilateral leg training in addition to conventional physiotherapy. Groups were assessed on first and the sixth week .Tool used for outcome measurement was Fugl-Meyer lower extremity physical performance scale(FMA) for measuring lower extremity motor function . Statistical analysis of data was done using student t test with SPSS software package. Result: It was found that lower extremity function and ADL improved significantly more in the experimental group (Group A) in comparison to control group (Group B). Conclusion: Repetitive bilateral leg training is a clinically simple and cost effective method for improving lower extremity motor and ADL functions of post MCA stroke hemi paretic geriatric patients .
Keywords: Repetitive bilateral leg training, Middle cerebral artery stroke, Geriatric population.
Full Text:
INTRODUCTION
Stroke is defined as a neurological deficit of cerebro vascular cause that persists beyond 24 hours or is interrupted by death within 24 hours1 . It is one of the most common causes of death and disability worldwide and leaves the survivors with significant physical and mental disability thus creating a major social and economical burden. The incidence of stroke increases dramatically with age , doubling every decade after 55. For the American white men aged 65-74 the incidence is about 14.84% , above 75 it is 24.6% and for 85 and older it is 27%.Incidence of stroke dramatically increases with age and increase in age is the single most powerful risk factor for stroke2 .By 2025 the world population is expected to include over 830 million people above 65 and most will live in developing countries like India, making it a major concern for the nation3 . The middle cerebral artery (MCA) is the single most common site of stroke. The term cardio vascular accident(CVA) is used interchangeably with stroke very often. Stroke can be of either ischemic or hemorrhagic variety. MCA stroke is characterized by common features such as contra lateral spastic hemi paresis or hemiplegia and sensory deficit of face, arm and leg with face and arm more involved than the leg. Lesions of the parieto-occipital cortex of the dominant hemisphere can produce aphasia .Motor deficits are characterized by either hemiplegia or hemi paresis typically on the side of body opposite to the site of lesion4 . Stroke is the largest consumer of rehabilitation services. Stroke is the third leading cause of death and there is a great need of physical rehabilitation in the initial phase after stroke5 . Physiotherapists have a major role in the hospital based ?inpatient‘ rehabilitation setting and in the community based rehabilitation settings6 . Re education of motor and functional abilities are the main targets of treatment by the physiotherapist. However the traditional methods have shown to improve the function only minimally and bilateral leg training was found to be an effective method in improving upper limb motor function7 . So in this study the investigator checks the effectiveness of repetitive bilateral leg training in improving the lower extremity motor function in post stroke hemi paretic patients of geriatric age group.
MATERIALS
Knee hammer
Standard 2 inch and .5 inch straps Static cycle Fugl Meyer Lower Extremity score Data collection sheet Essential stationary materials METHODOLOGY Prior sanction was obtained from the authorities, including ethical clearance, to conduct the study under the supervision of a consultant neurologist in PVS hospital, Calicut. Subjects were informed about the purpose of proposed research study .Referred patients with either left or right hemi paretic stroke were conveniently selected for the study on the basis of inclusion and exclusion criterias. Using random sampling subjects were then divided in to Group A or control group and Group B or experimental group. Both groups were assessed on the first day of treatment and after completion of their course of treatment. The control group was given 40 minutes of conventional physiotherapy for 6 days a week for 6 weeks. Outcome measures used were Fugl Meyer scale for assessing lower extremity motor performance. Experimental group was given 40 minutes of bilateral leg training in addition to conventional physiotherapy and a rest period of 1 minute was provided after each single group of exercises. Conventional physiotherapy group underwent 4 different types of exercises. Each single movement was repeated 10 times in patient‘s comfortable speed. First group of exercises were Active assisted range of motion(ROM) exercises for both upper and lower limbs which included 1)Elevation-depression, protraction- retraction of shoulder girdle.2)Abduction-adduction , Flexion-extension of glenohumeral joint.3)Flexion extension of elbow joint.4) supination-pronation of radio-ulnar joints.5) Flexion-extension and radial-ulnar deviations of wrist joint.6)Flexion- extension of metacarpophalangeal joint.7)Flexion-extension exercises of interphalangeal joint. In the lower limb following exercises were performed in patient‘s comfortable speed. 1) Flexion-extension in side lying, abduction-adduction and internal-external rotation in supine lying of hip joint.2) Flexionextension of knee joint.3) Dorsi-plantar flexion of ankle joint.4) Inversion-eversion of sub talar joints. Second group of exercises were Functional mobility exercises which included 10 repetitions of following movements. Third group was functional mobility exercises which included 1) Bed mobility exercises including rolling to affected side, rolling to un affected side, bridging of pelvis, prone on elbows, prone on hands, supine lying to sitting.2)Sitting to standing without assistance.3) Walking on parallel bar,4)Walking without support/assistive devices,5)Stair climbing exercises(five steps with assistance or support rails).Third group of exercises included Peg board activities for upper limb .Fourth group was balance training exercises including forward back ward steeping on wobble board ,braiding, manual perturbations sideways forwards and back words. The experimental group received bilateral leg training in addition to conventional physiotherapy. Bilateral leg training was given on supine lying, sitting positions and on a bicycle. The movements were started as active assisted movements and then progressed to active movements and to resisted movements depending on the improvements shown by patients. Each treatment session lasted for around 40 minutes and a rest period was provided after a single joint movement. Bilateral training consisted of two segments; ROM exercise and static cycling. ROM exercises included both symmetrical and asymmetrical movements of flexion-extension, abductionadduction, and medial-lateral rotation of hip joint. Both symmetrical and asymmetrical movements were repeated for 20 times and static cycling performed for 15-20 minutes. Statistical methods Statistical test used was students t Test. With in groups Pre and post test scores were compared using paired t test and between groups pre and post test scores were compared using unpaired t test. Level of significance was kept at .05. Data was analyzed using SPSS version 17.
RESULTS
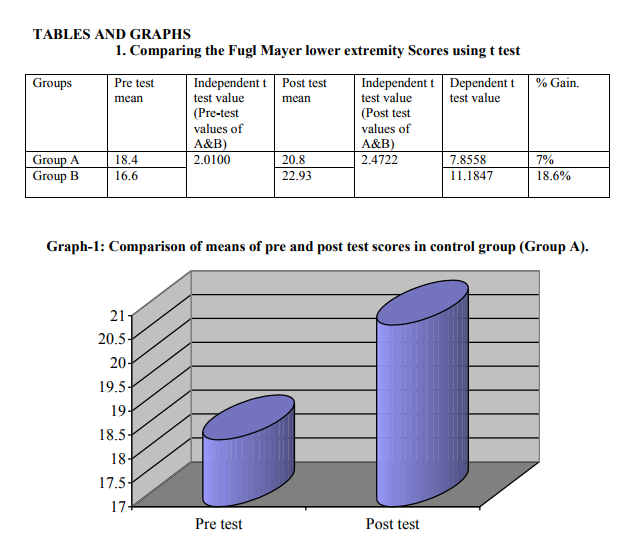
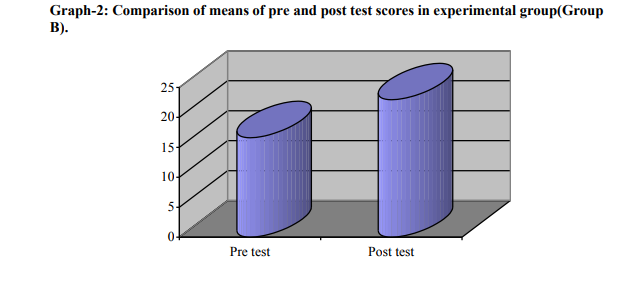
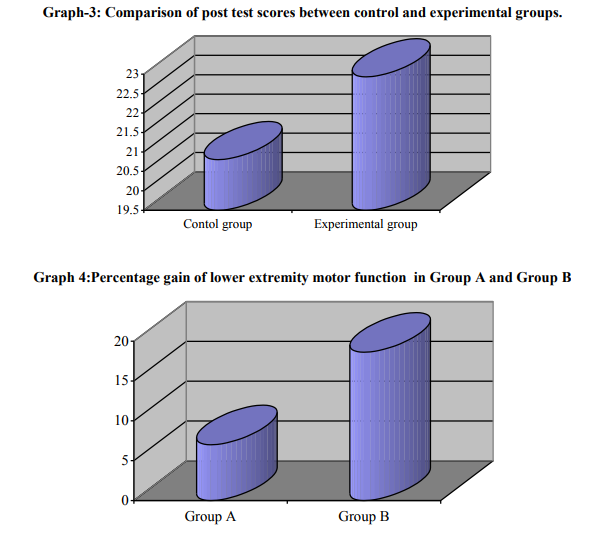
Pre test scores didn‘t show significant difference between two groups proving the homogeneity of the groups (t=2.010, sig=.145).Group A did show significant difference between pre and post test scores (t=7.858 sig=.05).Similarly group B also did show significant difference between pre and post test scores (t=11.1847, sig=.05). On comparison of post test scores between two groups also there was significant difference (t=2.4772, sig=.05).
DISCUSSION
Statistical tests proved that there was significant difference between pre test and post test groups of both experimental and control groups. But post test score of experimental group was found to significantly higher than that of control group proving that bilateral leg training is a superior method to conventional physiotherapy in improving lower limb motor function in acute hemi paretic MCA stroke patients. The better results obtained in the experimental group may be justified by the following findings. Practicing bilateral movements in synchrony and in alteration may result in facilitation effect from non paretic limb to paretic limb. When bimanual movements are initiated simultaneously, the limbs act as s unit that supersedes the individual limb action indicating that both limbs are strongly linked as coordinated unit in the brain8,9.Another proposed mechanism that is relevant here is neural plasticity. It refers to the fact that brain is malleable like plastic than being bare wired as previously thought. Researches shown that even a simple novel thumb movement sequence repeated over a time induced lasting cortical representation changes and these changes enlarge as learning occurs10- 12. Similarly other task specific repetitive practice regimens like constraint induced movement therapy too produced such kind of improvements. Another factor known as ?entraint‘ is suggested to be an important factor behind the effectiveness of bilateral training. It is better demonstrated by an example. Imagine signing ones first name on a chalk board using the non dominant hand at normal speed, but moving in direction opposite to normal. Even with practice this is very difficult to master. When attempting the task again with simultaneously writing using the dominant hand, it becomes easier. More importantly two hands appear to be locked together as the experiment demonstrates our limb; both upper and lower are indeed locked in what is commonly termed as entrainment13 . Related research suggested that limbs are spatially and temporally entrained that may be reason bilateral training is useful in relearning activities that are mutually bilateral such as walking14,15 . Role of contra lateral hemisphere is another important factor behind the effectiveness of bilateral training. Functional MRI studies had shown that damaged hemisphere had increased blood flow when bilateral movements were made. These data are consistent with the idea that activity of undamaged hemisphere might support damaged hemishere16.Similarly proprioceptive and visual feedback from the unaffected side is a very important factor in stroke rehabilitation. When performing bilateral training a patient can use the unaffected extremities neurologically intact afferent and efferent signals and look and feel of that movement within that limb, to promote similar movement in the affected limb17 . This study Suggests that a bilateral training program for the lower extremities of post stroke hemi paretic patients leads to significant gain in motor functions. This method appears simple and so it will be a useful training method in home for many stroke patients. What aspects of bilateral training lead to brain changes are still not very clear. So the future goal should be to systematically determine the most effective protocol for each patient.
References:
1. World Health Organization (1978). Cerebrovascular Disorders (Offset Publications). Geneva: World. ISBN 9241700432. OCLC 4757533
2. O‘Sullivan S B, Schmitz Thomas J , Physical rehabilitation-Assessment and treatment. 5th Ed. New Delhi: Jaypee brothers; 2007.PP 705-707,711-713.
3. Beers M.H, Berkow R, editors. The Merck manual of geriatrics.3rd Ed. White house station ( Nj): Merck research laboratories ;2003.
4. Carr J.H, Shepherd R B. Motor relearning program for stroke. 1st Ed .Woburn (MD): Butterworth and Heinman; 2000.
5. Gordon Mcir Gites, Jo Clarck Wilson. Brain injury rehabilitation-A neurofunctional approach. London: Chapman and Hall; 1993.
6. Harrison M. A, Ashburn. Physiotherapy in stroke management.1st Ed. London: Churchill Livingstone; 1995. PP 273-74.
7. Myers RS. Saunders manual of physical therapy practice. 1st Ed. Philadelphia: WB Saunders Company; 1995. PP 385-392.
8. Classen J. Liepest J et al. Rapid plasticity of human cortical representation induced by practice. J Neurophysiol .1998; 79(2):117- 1123.
9. Colleen A, Hanton B.S et al. New brain networks are active after right MCA stroke when moving the ipsilateral arm. Neurology.Jan2005:114-120.
10. Crammes SC, Bastings EP. Mapping clinically relevant plasticity after stroke. Neuropharmacology. 2000:39; 842-851.
11. Joachim L, Heike B et al. Treatment induced cortical reorganization after stroke in humans. Stroke. 2000:31; 1210.
12. Lenois GN, Wagner A et al. Experimental stroke therapy linked to brain changes. Stroke. June2005.
13. Neurophysiological and behavioural adaptations to a bilateral training intervention in individuals following stroke. Clinical Rehabilitation: Vol 18, Feb 2004; 48-59.
14. SJ Page, P Levine et al.A randomized efficacy and feasibility study of imagery in acute stroke. Clinical rehabilitation. 2001.
15. Jong SH, Kin Y et al. Cortical reorganization induced by task oriented training in chronic hemiplegic stroke patients. Neuro report. 2003:14(1) 137-141.
16. Staines WR, Mclloy WE et al. Bilateral movement enhances ipsilateral cortical activity in acute stroke- A pilot functional MRI study. Neurology 2001:56(3); 401-404.
17. Paje SJ, Peter Levine. Bilateral training aids rehabilitation progression. Biomechanics.Sept 2005.
18. Paje sJ, Johnson M, Levin P et al. Modified constraint induced therapy after sub acute stroke. A preliminary study. Neurorehabil neurorepair. 2002:16(3); 290-295.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





