IJCRR - 4(16), August, 2012
Pages: 69-75
Date of Publication: 28-Aug-2012
Print Article
Download XML Download PDF
A STUDY OF TRACE ELEMENTS (IRON, ZINK, COPPER, SELENIUM) IN LIVER CIRRHOSIS PATIENTS
Author: Sunil Gupta, Shravn Kumar Meena, Jitendra Ahuja, Vishnu Dutt Bohra
Category: General Sciences
Abstract:Objective \- The aim of present study is to examine serum level of Selenium, Copper, Zinc and Iron in Liver cirrhosis patients and Compare the level of Selenium, Copper, Zinc and Iron in Patients with liver cirrhosis with age, sex matched normal control subjects. Research Design Methods\- this open-ended comparative transverse study was designed to evaluate serum selenium, zinc, and copper and Iron levels in blood and liver function test (Bilirubin, Serum Glutamate Oxalate Transaminase, Serum Glutamate Pyruvate Transaminase, Akaline Phosphatse, Gamma Glutamyl transferase, Total Protein, Albumin, and Globulin) in 100 patients with liver cirrhosis and compared with 50 normal people without liver cirrhosis or any other clinical problems. Results\- the values of serum GGT, Bilirubin, copper and Iron levels in blood were increased statistically significant (p< 0.00l) in liver cirrhosis when compared with the control subjects. Statistically significant difference (p< 0.00l) in selenium, zinc and Albumin were also found in subjects of liver cirrhosis. Conclusions\-the correction of serum trace elements concentration would have a beneficial effect on treatment, complication and progression of the diseases, so it would be recommendable to provide laboratory analysis of trace elements as a routine in liver cirrhosis patients.
Keywords: Trace elements, liver cirrhosis, Liver function tests
Full Text:
INTRODUCTION
Cirrhosis is a chronic disease of the liver in which diffuse destruction and regeneration of hepatic parenchymal cells has occurred, in which diffuse increase in connective tissue has resulted in disorganization of the lobular architecture. The triad of parenchymal necrosis, regeneration and scarring is always present regardless of individual clinical manifestations.1 Liver cirrhosis is a major cause of death in the United States.2 Hepatitis and cirrhosis are also considered serious liver disease even in western countries. Former is known to be reported in about 75000 patients in a year and latter one is responsible for 23000 deaths a year in USA. These figures certainly will be several times more for India.3 In developing countries such as India, viral hepatitis is the leading cause of cirrhosis and in the developed countries such as USA, ALD, HCV and NASH is the most common cause of cirrhosis.4 Cirrhosis and chronic liver diseases were the 10th leading cause of death for men and 12th for women in the United States in 2001, killing about 27000 people each year.5 Long term intake of alcohol increases reactive oxygen species and Free radicals by two mechanisms first, cytochrome P-450 2E1 is regulated, causes oxidation of NADPH (Nicotinamide Adenin Dinucleotide phosphate)
reduced to NADP generating free radicals and second, hepatic macrophages are activated which subsequently produce TNF-α. TNF-α induce mitochondria to increase production of reactive oxygen species. Free radicals initiates’ lipid peroxidation which causes inflammation and fibrosis and oxidative stress causes necrosis and ap of liver cells. Due to deficiency of glutathione and vitamin-E, necrosis/ apoptosis exaggerated.6 To prevent this mechanism our cells possesses antioxidant such as copper-zinc superoxide dismutase (Cu-Zn SOD), glutathione peroxidase (GSH-Px) and catalase are present in the cell. All these antioxidant are designed to prevent the occurrence of free radical injury under normal condition. These antioxidants contain trace elements such as selenium, copper, zinc and iron.7 Increased level of lipoperoxidase have also been reported in the sera of liver cirrhosis patients which may be due to the reduction of glutathione peroxidase (a selenium containing enzyme) known to accompany liver impairment . 8 Zinc is associated with more than 300 enzymatic systems. Zinc augments the natural defense of reactive oxygen radicals by Zn-enzyme, Cu-Zn superoxide dismutase .9 Copper is an essential trace element which participates in many enzymatic reactions. Its most important role has in redox process. Reactive copper can participate in liver damage directly or indirectly through kupffer cells stimulation.10 On theoretical ground trace element may be protective against oxygen free radicals in the development of liver cirrhosis. So present study had been designed to study the levels of serum trace elements (Cu, Zn, Fe and Se) in patient of liver cirrhosis and compared to control subjects and to assess the level of trace elements.
MATERIAL AND METHOD
This open-ended comparative transverse study was conducted on 100 patients of liver cirrhosis diseases admitted in medical wards, in a tertiary care Hospital, during the period of August 2009 to August 2010. Written informed consent by the subject and ethical approval was appropriately sought before the study. Fifty healthy controls were taken Control subjects were selected. This study was designed to evaluate serum selenium, zinc, and copper and Iron levels in blood and liver function test (Bilirubin, SGOT, SGPT, ALP, y-GT, TP, Albumin, and Globulin) in 100 patient with liver cirrhosis. The data obtained from our study is to be compared with 50 normal people without liver cirrhosis or any other clinical problems. The data is also used to see that if there is any variation in levels of trace metals with severity of disease. The blood samples were collected after 12 hours of fasting. The peripheral venous blood samples were taken at 8 AM. Subject selection:- Based on following inclusion and exclusion criteria, a random selection of subjects for the study was made on basis of detailed history and proper clinical examination.
Inclusion Criteria:
- Patient with liver cirrhosis disease
- Age 20-60 year
Exclusion Criteria:
- Patient with the following condition:
- Hepatocellular carcinoma
- Age under 18
- Renal failure
- Lactation
- Any chronic disease
- Drugs affecting levels of trace metals eg. Corticosteroids, digoxin, thiazide diuretics etc.
A detailed clinical history of each patient, which included age, religion, residence, and socioeconomic status, Diet, Lifestyle, presenting complaints, Personal history, Past History family history, Drug history and Allergy history was recorded. A systemic examination was done to rule out presence of any systemic illness. The patient was made to lie in dorsal position and inspection, palpation and auscultation was done. The rest of the assessment was undertaken as per the prescribed study format. Serum Bilirubin, SGOT, SGPT, ALP, y-GGT, TP, Albumin, Globulin were estimated by enzymatic colorimetric method on Olympus AU400 auto analyzer after appropriate calibration. The copper, selenium, iron and zinc levels in the serum of each subgroup were measured with the help of an Atomic Absorption Spectrophotometer (AAS4 14 1AAS) in a standardized manner under set protocol.
RESULTS
The Mean age for case was 46.45 +7.00 and for control was 44.86 ±5.93.The maximum number of cases 41(41%) were in age group of 40-49 years ,followed by 36(36%) in more then 50 years age group, 23(23%) cases in 30-39 age group were present. It was observed that maximum number of cases was in age group 40- 49. This is consistent with the average age of diagnosis of liver cirrhosis. To avoid any variation that occurs due to difference in dietary habits of religions. We had taken liver cirrhosis patient and control persons according to the religion. The 79 (79 %) cases were of Hindu religion and 21 (21%) cases were of Muslim religion. In the control group 40 (80%) persons were of Hindu religion and 10 (20%) persons were of Muslim religion. The cases occurred in Middle Income Group class 37 (37%) followed by Lower Income Group 35(35%) and the only 28(27%) cases belongs to the Higher Income Group class. The maximum number of cases is of middle class supporting the fact that it is a disease of middle class persons. The maximum number of cases i.e. 70 (70%) included in the study were from Rural dwelling as compared to 30(30%) of cases from Urban background. This is consistent with the theory of cirrhosis as a disease of rural background. In the control group 41 (82%) persons is of urban background and 9 (18%) person is of rural background. The maximum number of the cases occurs in Alcoholic groups 64(64%) followed by 36(36%) cases belongs to the Non alcoholic groups. It reveals that cirrhosis occurred maximally in Alcoholic groups.
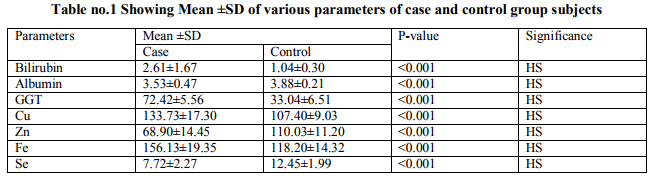
We observed in this study that the mean bilirubin and GGT levels were higher in liver cirrhosis patients as compared to control persons ( P<.001) The serum levels of Copper and The mean serum Iron levels was found to be higher in case group as compared to control group (P< 0.001), and this is highly statistically significant. The serum levels of Albumin, Zinc and Selenium were found to be lower in case group as compared to control group and this is also highly statistically significant (P< 0.001). There is also no statistically significant variation in BMI of case and control group were observed (22.72± 1.66 vs. 22.42 ± 1.78 P> 0.05).
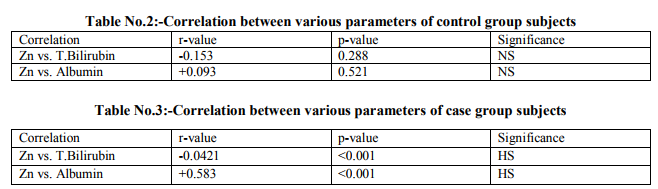
Table 3 shows that there was negative correlation between levels of bilirubin and Zinc. The r value was — 0.042 1 in case group which is statistically significant ( P< 0.001 ) as compared to control group (Table no. 2)in which the r value was 0.153 and this was not significant statistically ( P>0.05 ). Similarly, as far as Zinc was concerned there was positive correlation between levels of Albumin and Zinc. The r value was 0.583 in case group which is statistically significant (P< .001 as compared to control group in which the r value was 0.O93and this was not significant statistically (P> 0.05).
DISCUSSION
The importance of trace elements in the process of maintaining life is well known. Trace elements are characteristically required for growth and maintenance of life. At present, it is recognized that so many trace elements including copper, zinc, iron and selenium are essential for human body. Lack or an insufficient intake of such micro nutrients turns out a functional impairment or can consequence in disease.11 The clinical significance and evaluation of trace elements such as Copper, Iron, Selenium and Zinc in regard to different diseases including liver cirrhosis remain conflicting as well as controversial and many questions still remain unanswered. Mechanisms linked on ethanol metabolism, especially oxidative stress, redox potentials and acetaldehyde, participate in the emergence of liver damage. Trace elements play an important role in oxidative stress and redox potentials. A possible role of zinc, copper, iron and selenium in pathogenesis of liver cirrhosis and its complications is still subject of research. The present study, though probably first of its kind in Indian population, is an attempt forward in series of previous studies done internationally to study the level of trace elements in the patients of liver cirrhosis. In our research study the serum levels of zinc were found significantly lower in patients with liver cirrhosis in comparison to controls. (Table no.1) The same finding was reported by Lin et al in 2006;12 they find that mean zinc level in the serum of patients with hepatic cirrhosis was significantly lower than that of the control group. Moreover they found markedly elevated Cu: Zn Ratio in patients with hepatic cirrhosis or hepatocellular carcinoma. Their finding implies that the level of some trace elements, such as selenium, iron, copper, and zinc and Cu: Zn ratio might serve as biomarkers for the increased severity of viral hepatic damage. Alteration of Zn homeostasis in liver cirrhosis is supported by a large body of experimental and clinical evidence. Dario et al in 2006 demonstrated that the levels of zinc were significantly lower in patients with liver cirrhosis in comparison to controls (p<0.001).13 Hypozincemia in cirrhosis is also demonstrated by Celik et al in 2002, in this study they observed that the mean value of serum and ascites zinc level was significantly lower in cirrhosis patients than healthy controls.14 Similar study is also done by Loguercio et al in 2001 .Their results indicate that zinc concentration is associated with viral hepatitis, decreasing with the development of cirrhosis and low function of liver.15 However the cause and mechanism resulting in decreased serum zinc concentration in liver cirrhosis remain to be unexplained yet. But there are some explanations for the decrease of zinc content in the serum of cirrhosis patients. During the cell damage and inflammation, liver cells take up more zinc to synthesize nucleic acid, protein and enzymes related with zinc. With progression of the liver damage, due to poor appetite, impaired function of intestines and stomach and high pressure of the portal vein, the zinc intake and Absorption decreases and also the low content of serum albumin results in less combination with zinc and because of the diffusion characteristic of blood zinc, it is easily lost through urine and sweat. In our study the serum copper content was found significantly increased in patients with liver cirrhosis in comparison to the control group (Table no.1). The same finding was reported by Nakayama et al in 2002. Their results indicate that the copper level of the patients with liver cirrhosis and hepatocellular carcinoma were significantly higher than in patients with chronic hepatitis and controls.16 It could be explained with copper’s role in the redox process. Redox cycling between Cu2+ and Cu1+ can catalyze the production of toxic hydroxyl radicals. It is a well known fact that redox processes and oxidative stress play an important role in the pathogenesis of liver cirrhosis. The increased copper value may be due to release of copper from damaged necrotic hepatocytes. Similarly the mean value of iron in table no.1 summarized that the liver cirrhosis patients has increased serum iron concentration than the normal subjects. Hence the difference between the two samples mean statistically differ significantly i.e. <0.001. The same findings were reported by Jurczvk et al in 2001.17 The study done by Mohammad H. Somi et al 2007 implied that serum iron level was higher in cirrhosis patients than in normal subjects.18 Patients with chronic liver diseases have a tendency to accumulate an excessive amount of iron in their liver parenchyma. The acute phase reactions associated with chronic inflammatory states increase uptake of iron through the gastrointestinal tract and cause to remove excess iron by the kupffer cells. Consequently with the damage of hepatocytes, the release of iron from injured cells to serum develops. The serum selenium content was found significantly decreased in patients with liver cirrhosis in comparison to the control group (Table no1). Similarly Kalkan et al in 2002 have studied serum trace elements, including selenium in sera of patients with viral hepatitis cases, and statistically compared with the controls. A significant decrease in selenium levels has been suggested in patients with HCV infection due to the defense strategies of organisms probably induced by substances like retinol or various carotinoids.19 Jan Aaseth et al in 1982 reported that alcoholic cirrhosis and chronic hepatitis patients had a significant decrease of serum selenium level than in normal healthy adults.20
Decrease in serum selenium might indicate the development and progression of liver cirrhosis. It also links to the disease progress of some viral agents in relation to the biosynthesis of selenoproteins 21 and decrease in serum selenium significantly increases the risk of liver cirrhosis mortality.22 Declining serum Se might involve reduced biosynthesis of the hepatically derived selenium transport protein selenoprotein P (SePP) for its human promoter is negatively regulated by proinflammatory cytokines in vitro.23 Four-year animal studies showed that dietary supplement of Se reduced the HBV infection by 77.2%.24 In conclusion, the trace elements such as copper, zinc, iron and selenium are found to be statistically significant (p < 0.001); this study confirms the variation of their Concentration in liver cirrhosis patients compared with healthy volunteers. Change in trace elements associated with some biological reaction takes place in the liver. The results of present study also support the fact that there is positive correlation between albumin and zinc and negative correlation between bilirubin and zinc in patients of liver cirrhosis. Considering all that, the correction of serum trace elements concentration would have a beneficial effect on treatment, complication and progression of the diseases, so it would be recommendable to provide laboratory analysis of trace elements as a routine.
References:
1. Conn HO. Cirrhosis. In: Diseases of the liver 4th edition. Edited by Schiff L.Philadelphia: J.B. Lippincott Company; 1975:833
2. Yoon, Y.—H.; Yi, H.; Grant, B.F.; et al. Surveillance Report #60: Liver Cirrhosis Mortality in the United States, 1970-99. Washington, DC: National Institute on Alcohol Abuse and Alcoholism, 2002.
3. Tandon, B.N., S.K. Acharya, A Tandem Epidemiology of Hepatitis B Virus Infection In India, Gut, 1996, 38 (Suppl. 2), S56— S59. 4.
4.Wynn T. Cellular and molecular mechanisms of fibrosis. J Pathol2008; 214: 199-210
5. Arias, E.; Anderson, R.N.; Kung, H.-C.; Murphy, S.L.; and Kochanek, K.D. Deaths: Final Data for 2001. National Vital Statistics Reports, Vol. 52, No. 3. Hyattsville, MD: NCHS, 2003.
6. Giovanni Tarantino, Matteo Nicola Dario Di Minno and Domenico Capone. Druginduced liver injury: Is it somehow foreseeable? World J Gastroenterol. 2009 June 21; 15(23): 2817-2833.Published online 2009 June 21. doi: 10.3748/wjg.15.2817.
7. Halliwell Barry, Antioxidants in Human Health and Disease, Annual Review of Nutrition Vol. 16: 33-50 (Volume publication.date July 1996)DOI: 10.1146/ annurev. nu .16.070196.000341
8. Diluzio N R (1973): Antioxidants, Iipid peroxidation and chemical induced liver injury. Federation Proc. 32, 1875- 1881.
9. William E Stehben, Oxidative stress, toxic hepatitis, and antioxidants with particular emphasis on zinc, Experimental and Molecular Pathology,Volume 75, Issue 3, December 2003, Pages 265–276
10. Klein, D.,J. Lichtmannegger, U. Heinzmann, J. Muller Hocker, S. Michaelsen , K. H. Summer, Association of copper to metallothionein in hepatic lysosomes of Long–Evans cinnamon (LEC) rats during the development of hepatitis Eur. J. Clin. Invest. 28 (1998) :4,302.—310.
11. K. O. Soetan,C. O. Olaiya and O. E. Oyewole, The importance of mineral elements for humans,domestic animals and plants: A review, African Journal of Food Science Vol. 4(5) pp. 200-222, May 2010
12. Lin CC, Huang JF, Tsai LY, Huang YL. Selenium, Iron, Copper, and Zinc level and copper to zinc ratios in serum of patients at different stages of viral hepatic disease. Biol Trace Elem Res 2006; 109: 15-24.
13. Dario R.,Milan K., , Zljko Romi,Kristina Brki and Mladen Petrove~ki, Serum Concentration of Zinc, Copper, Manganese and Magnesium in Patients with Liver Cirrhosis, Coll. Antropol. 30 (2006) 3: 523– 528
14. Celik, H. A., H. H. Aydin, A. Ozsaran, N. Kilincsoy, Y. Batur, B. Ersoz, Clin. Biochem., 35 (2002) 477. — 12
15. Loguercio C, De Girolamo V, Federico A, Feng SL, Crafa E, Cataldi V, et al. Relationship of blood trace elements to Mohammad H. Somi et aL32 liver damage, nutritional status, and oxidative stress in chronic nonalcoholic liver disease. Biol Trace Elern Res 2001; 81: 245-54.
16. Nakayama A, Fukuda H, Ebara M, Hamasaki H, Nakajima K, Sakurai H. A new diagnostic method for chronic hepatitis, liver cirrhosis, and hepatocellular carcinoma based on serum metallothionein, copper, and zinc levels. Biol Pharm Bull 2002; 25: 426-3 1
17. Jurczyk K, Syczewska M, Kaczrnarska A, Sych Z. Serum iron parameters in patients with alcoholic and chronic cirrhosis and hepatitis. Med Sci Monit 2001; 7: 962-5.
18. Mohammad H. Somi, Alireza Ostad Rahimi, Behnaz Moshrefi,Parisa Rezaeifar,Jamal Ghaem Maghami Nutritional Status and Blood Trace Elements in Cirrhosis Hepatitis monthly 2007;7(1):27-32
19. Kalkan, A., Bulut, V., Avci, S., Celik, I. and Bingol, N. K., Trace elements in viral hepatitis. J. Trace Elem. Mcd. Biol., 2002, 16,227—230.
20. Jan Aaseth, Jan Alexander, Yngvar Thornassen, Jan P.Blomhoff and Sverre Skrede , Serum selenium levels in liver diseases, Clinical Biochemistry Volume 15, Issue 6, December 1982, Pages 281–283 Available online l8October 2004
21. Banares, F.F., E. Cabre, M. Esteve, Serum Selenium and risk of large size colorectal adenomas in a geographical area with a low selenium status, Am. J. Gastroenterol., 2002, 97, 2 103—8.
22. Beáta Éva Petrovski,Vera Pataki,Tibor Jenei,Róza Ádány,Zoltán Vokó Selenium levels in men with liver disease in Hungary, Journal of Trace Elements in Medicine and Biology Volume 26, Issue 1, January 2012, Pages 31–35
23. Dreher, I., T.C. Jakobs, J. Kohrle, Cloning and characterization of the human selenoprotein P promoter. Response of selenoprotein P expression to cytokines in liver cells, J Biol Chem., 1997, 272(46), 29364—7 1.
24. Taylor, E.W., R.G. Nadimpalli, C.S. Ramanathan, Genomic Structures Of Viral Agents In Relation To Biosynthesis Of selenoproteins, Biol. Trace Element Res., 1997, 56, 63—9 1.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





