IJCRR - 4(24), December, 2012
Pages: 105-112
Print Article
Download XML Download PDF
EFFECT OF LEAD EXPOSURE ON BIOCHEMICAL PARAMETERS IN AUTOMOBILE WORKERS FROM BIJAPUR, KARNATAKA
Author: Nilima Dongre, Adinath Suryakar, Arun Patil, Basavaraj Devarnavadagi, Jeevan Ambekar, Dileep Rathi
Category: Healthcare
Abstract:Background of the Study: In humans, lead can cause a wide range of biological effects depending upon the level and duration of exposure. The heavy metal lead (Pb) is one of the most widely scattered toxic metals in the world. It has been used by mankind for over 9000 years. Lead in the environment may be derived from natural or anthropogenic sources. Aim and Objective: The aim of this study was to investigate the adverse effect of exposure to lead on a) systolic and diastolic blood pressure, b) serum calcium, ionized calcium, phosphorus and c) kidney functions, of automobile workers. Methods: For this study, two groups of thirty (30) automobile workers and thirty age matched healthy control subjects were selected from Bijapur city. Demographic, occupational and clinical data was collected using questionnaire. From these two groups, venous blood samples in EDTA and Plain bulbs and random midstream urine samples were collected in amber coloured bottles. The biochemical parameters were estimated using standard assay procedures. Statistical analysis of the data was done using independent student?s„t? test for parametric variables. Values were expressed as mean \? standard deviation (SD). P values of 0.05 or less were considered to be statistically significant. Results and Conclusions: As compared to controls, the automobile workers were found to have significantly increased (P< 0.001) blood and urinary lead levels, significantly increased (P< 0.05) systolic and diastolic blood pressure and high (P< 0.05) levels of blood urea, serum uric acid and serum creatinine levels and the levels of serum calcium, ionized calcium, phosphorus were significantly reduced (P< 0.001). The chromatography of the urine samples shows the generalized aminoaciduria in these workers. The results of this study clearly indicate that the absorption of lead is more in these workers which adversely affects blood pressure, disturbs calcium and phosphorus metabolism and damages renal tubules. Since absorption of lead has ill effects on the health of automobile workers, there is an urgent need to safeguard them from the hazards of occupational lead exposure.
Keywords: Automobile workers, Blood lead (Pb-B), Urinary Lead (Pb-U), Systolic and Diastolic blood pressure, Calcium, Phosphorus, Ionized Calcium, Kidney function tests and aminoaciduria.
Full Text:
INTRODUCTION
Lead (Pb) is one of the most widely scattered toxic metals in the world. It has been used by mankind for over 9000 years. Lead in the environment may be derived from natural or anthropogenic sources. Lead and its compounds may enter the environment during mining, smelting, processing, use, recycling or disposal. Airborne lead can be deposited on soil and pollute water thus reaching humans through the food chain and drinking water. Levels of lead found in air, food, water, soil and dust vary widely throughout the world and depend upon the degree of industrial development, urbanization and lifestyle factors 1, 2 . Lead is absorbed by the gastrointestinal tract (GIT) via food, beverages, soil and dust in industrial zone. Diet, nutritional status, chemical form of the metal and the pattern of food intake affect lead absorption. Lead is not distributed homogeneously throughout the body. It is rapidly taken up in blood and soft tissues (half life 28-30 days) followed by a slower redistribution to bone (half life 27 years). Dietary lead which is not absorbed in GIT is excreted in faeces 3, 4 . A wide variation exists in individual?s susceptibility to lead poisoning, with a corresponding range in the spectrum of clinical findings. Sub acute or chronic toxicity is more common than acute poisoning. Early symptoms are often subtle, nonspecific and/or subclinical, involving the nervous system (restlessness, fatigue, irritability, sleep disturbance, headache, difficulty in concentrating, decreased libido etc.), GI system (abdominal pain, anorexia, nausea, constipation, diarrhoea etc.) or musculoskeletal system (arthralgia, myalgia). Other less common conditions include tremor, toxic hepatitis or acute gouty arthritis (saturnine gout). In general, severity of symptoms worsens with increasing blood lead levels. A high blood lead level may result in delirium, coma, and seizures associated with lead encephalopathy, a life threatening condition 5, 6, 7 . In humans, lead can cause a wide range of biological effects depending upon the level and duration of exposure. It causes adverse effects in several organs and organ systems including nervous, renal, cardiovascular, reproductive, haematological and immune system 2, 7 . Adverse biochemical effects of lead are well known today. A correlation between clinical signs and symptoms with blood lead level and relevant biochemical changes may provide important information for making suitable changes in the working environment of workers. Therefore the present study was planned to find out the effect of lead on kidney functions, calcium and phosphorus metabolism, systolic and diastolic blood pressure of automobile workers.
METHODOLOGY
The study was carried out in 30 subjects with occupational exposure to lead i.e. Automobile workers (study group) and 30 normal healthy subjects (non-occupational lead exposure controls) from Bijapur. All the study group and control group subjects were in age ranging from 20 to 45 years. Prior to data and biological specimen collection, the workers were informed on the study objectives and health hazards of lead exposure. Informed consent was obtained from all the workers. Demographic, occupational and clinical data were collected by using questionnaire and interview. The ethical clearance was obtained from the institutional ethical committee. Most of the automobile workers had major complaints of muscle pains, itchy feeling, mild fatigue, aggressiveness, irritability, lethargy, poor concentration and abdominal discomfort etc. All the subjects of both the study group and controls belonged to average socio-economic strata of society. None of the subjects had any past history of major illness. Dietary intake and food habits of all subjects were normal. The subjects, who were on medication for minor illnesses, were excluded from this study. The workers selected for the study were non-smokers and non-alcoholic males, who were exposed to lead for more than 6 hrs/day and for 2 to 20 yrs period. The present study was carried out in the Dept. of Biochemistry, B.L.D.E.U?s Shi B.M.Patil Medical College Bijapur and Central Faciilty Centre, Shivaji University, Kolhapur. Venous blood samples were collected from the subjects and dispensed in plain screw cap test tube for the estimation of biochemical parameters from serum samples and also in test tube containing heparin as anticoagulant for estimating blood lead. To avoid the errors from the inadequate collection of 24 hrs urine samples, spot midstream urine samples were collected from each subject in amber
Where S Ca = Serum total calcium and
S Pr = Serum total protein
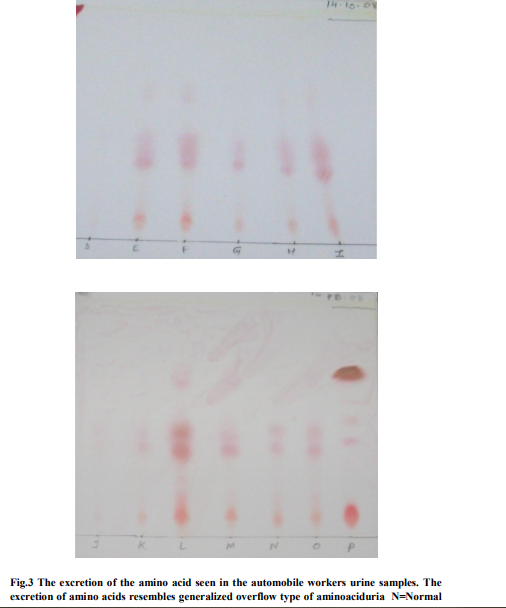
Serum inorganic phosphorus was estimated by Wang et.al; and Daly and Ertingshausens method 14,15 . Inorganic phosphorous combines with ammonium molybdate in presence of strong acids to form phosphomolybdate. The formation of phosphomolybdate is measured at 340 nm and is directly proportional to the concentration of inorganic phosphorous present. Urinary excretion of amino acids was analyzed by thin layer chromatography. The chromatography separation takes place by partitioning of the molecules from the mixture between the stationary
colour bottle at the time of blood collection. Both the blood and urine samples were immediately stored at 0 0 c to 4 0 c temperature. All biochemical parameters including kidney function tests were measured on the same day of the sample collection. Blood–lead (Pb-B) and urinary-lead (Pb-U) levels were estimated by the atomic absorption spectrophotometer (AAS) a Perkin Elmer model 303 fitted with a Boiling three slot burner. The spectrophotometer was connected to a readout Hitachi 165 recorder 8, 9 . Systolic and diastolic blood pressures of the workers were measured in resting i.e. supine position before the sample collection and expressed as mm of Hg 10 . Serum Calcium was estimated by Arsenazo III complex method in which calcium reacts with a dye Arsenazo III at pH 3.8 to form bluish purple colour complex and the intensity of the colour formed is directly proportional to the amount of calcium present in the sample 11 . Serum ionized calcium was calculated by employing the method of Mclean and Hasting as adopted by Beeler and Atrou using the following formula 12, 13 .phase and the mobile phase depending upon their relative affinity to each one of the phases 16 .
RESULTS
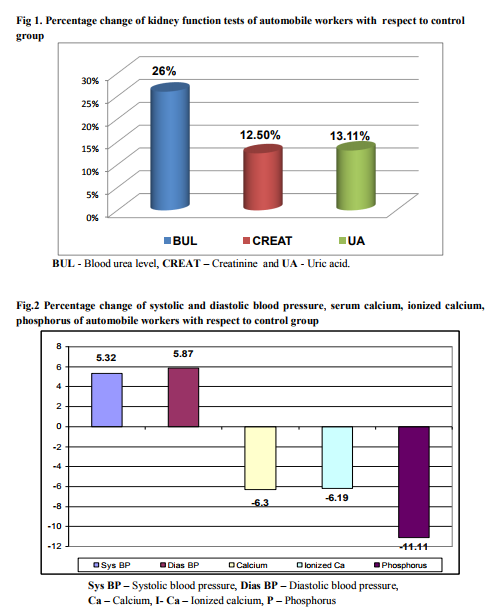
The results obtained in terms of mean values and SD of biochemical parameters of the study group and the control group are presented in Table 1.which shows Blood lead and urinary lead levels of automobile workers are significantly increased (P<0.001) as compared to controls. Systolic and diastolic blood pressure were significantly raised (P<0.05) in the study group as compared to controls. Serum calcium, ionized calcium, phosphorus were significantly decreased (P<0.001) in the study group. Blood urea, serum uric acid and serum creatinine (P<0.05) levels were significantly increased in the automobile workers. The Percentage change of kidney function test parameters of automobile workers as compared to controls are shown in Figure 1. The Percentage change of Systolic and diastolic blood pressure, Serum calcium, ionized calcium and phosphorus are presented in Figure 2.
DISCUSSION
In automobile workers blood lead (Pb-B) (364%, P < 0.001), and urinary lead (Pb-U) (176%, P < 0.001) (Table 1) levels were significantly increased as compared to control subjects. This indicates that absorption of lead is more in these workers. Absorption of lead ordinarily results in its rapid urinary excretion. It is reported that Pb-B levels generally reflect acute/recent and /or current exposure as also by the influence of previous storage in the body. Automobile workers are prone to lead exposure due to their routine activities like battery recharging and replacing, welding, spray painting, radiator repairing etc 17. However in this study we have taken workers involved only in radiator repairing, spray painting and battery recycling and recharging. The work places in which these workers undertake the job were not confirming to standard specifications for it. Further the workers were blissfully ignorant about the ill effects of exposure to lead. They were also very unhygienic. It was observed that they neither bothered change their working garments nor wash their hands properly before having their meals. Such unhygienic working conditions and habits have resulted in the workers showing symptoms of anorexia, muscular pain, abdominal pain and headache which they accept with disdain. Increased blood lead level affects on several biochemical parameters. In our study, as shown in (Table-1, Figure-1) in respect of automobile workers as compared to controls it is observed that blood urea (26%, P <0.05), serum uric acid (13.11%, P<0.01) and serum creatinine (12.5%, p<0.001) levels were significantly increased, indicates slight nephrotoxicity may be due to lead. Lead is known to cause proximal renal tubular damage, characterized by generalized aminoaciduria, hypophosphataemia, with relative hyperphosphaturia and glycosuria accompanied by nuclear inclusion bodies, mitochondrial changes and cytomegaly of the proximal tubular epithelial cells. Tubular effects are noted after relatively short-term exposures and are generally reversible, whereas sclerotic changes and interstitial fibrosis, resulting in decreased kidney function and possible renal failure, require chronic exposure to high lead levels. Increased risk from nephropathy was noted in workers with a PbB level of over 60 ?g/dl 1 .The evolution of lead nephropathy is usually silent. The central events appear to be the progressive destruction of tubular cells and their replacement by fibrosis. Clinical manifestation of impairment, characterized by rise in blood urea nitrogen or serum creatinine, does not ordinarily become evident until 50-70 % of the nephrons are destroyed. Pathological late stage of lead nephropathy is characterized by interstitial fibrosis with atrophy and dilation of the tubules and relative sparing of glomeruli at this stage intranuclear inclusion are infrequent 1 . This study indicates that Systolic (5.32%, P < 0.05) and diastolic (5.87%, P < 0.05) (Table 1, Fig.2) blood pressure were significantly high in automobile workers as compared to controls, which indicates adverse effects of lead on cardiovascular system. Lead impairs normal kidney functions which may result in secondary hypertension. In automobile workers serum calcium (– 6.3 %, P < 0.001), ionized calcium (– 6.19%, P < 0.001), phosphorus (– 11.11%, P < 0.001) were significantly decreased as compared to controls. (Table 1, Fig.2). It may be due to inhibition of 1-α hydroxylase enzyme in renal tubules. Lead causes nephrotoxicity and inhibits 1- α hydroxylase enzyme which leads to decreased calcitriol synthesis resulting in impaired calcium and phosphorus absorption across GIT and renal tubules. It is well known that lead causes proximal renal tubular damage which leads to generalized aminoaciduria, hypophosphatemia with relative hyperphosphoturia and glycosuria 18, 19. Therefore, we made an attempt to investigate whether any amino acids are excreted in automobile workers. These investigations revealed generalized aminoaciduria in 13 automobile workers, out of 30 i.e. 43% (Fig.3). These results clearly indicate that, lead adversely affects on the normal function of renal tubules. This is also supported by the evidence of increased blood urea, uric acid and creatinine found in these study groups.
CONCLUSIONS
The study shows that automobile workers must be considered as personnel under professional risk as their routine activities affect many systems in our body like liver, kidney and may lead to organ damage. The dietary factors, nutritional status, patterns of food intake, demographic changes and the chemical form of the metal affects the absorption of lead. The clothes of automobile workshop workers serve as a source of lead exposure to their family members also. A drastic increase in the number of automobiles in last two decades has only added to increase in the exposure of workers of this industry segment to the ill effects of lead. The study indicates lead toxicity still persists in automobile workers. There is a need to protect these workers. Medical examination and estimations of blood and urinary lead should be done be at regular intervals to identify workers with potential lead toxicity. The implementation of modern risk assessment techniques could improve the preventative element in these workshops.
Conflict of interest: NIL
ACKNOWLEDGEMENTS
We express our deep gratitude to all the automobile workers who consented to volunteer in the project. We also acknowledge the research facilities provided by B. L. D. E. U? s Shri B M Patil Medical College, Bijapur, Karnataka, Dr. V M Govt. Medical College, Solapur and Central Facility Centre, Shivaji University Kolhapur, Maharashtra, India. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. Authors are also grateful to authors /editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. World health organization, Biological indices of lead exposure and body burden. In: IPCS, Inorganic lead Environmental Health Criteria 118? Geneva Switzerland: WHO; 1995. 165:114-118.
2. Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological profile for lead, US Department of Health and Human Services, Atlanta Georgia USA: US Government Printing; 2005.102-225.
3. Casarett and Doull?s Toxicology “The Basic Science of Poisons” edited by Curtis D.Klaassen Chapter 23: Toxic effects of metals – 2008. p 943-947 7th ed. Mc Graw Hill publication.
4. Carl Zenz O, Bruce Dickerson and Edward P.Horvath edited Occupational medicine Ch 38. “Lead and its compounds –Leon A. Saryan and Carl Zenz. 1994; Page 506-540, 3rd ed Mosby publishing company.
5. IPCS Environmental health criteria 85 LeadEnvironmental effect Geneva WHO, 1989. 106.
6. D.A Gidlow, “Lead Toxicity” In depth review. Occupational Medicine. 2004. 54:76-81.
7. Arun J. Patil, Vinod R. Bhagwat, Jyotsna A. Patil, Nilima N. Dongre, Jeevan G. Ambekar and Kushal K. Das. Biochemical aspects of lead exposure in silver jewellery workers of Western Maharashtra (India). Journal of basic and clinical physiology and pharmacology 2006. Vol.17, No.4, 213-229.
8. Parson P J Slavin W. A rapid Zeeman graphite furnace AAS method for determination of lead in blood spectrochim Acta 1993. 48 B 925- 939.
9. A.A. Grenik. Determination of lead chelated with EDTA in blood after precipitation of protein with perchloric Acid. Brit. J Industr Med 1970.27, 40-42.
10. Jill A. Metz , Cynthia D.Morris ,Leslie A. Roberts , Michael R.McClung , and David A.McCarron. Blood Pressure, and calcium intake are related to bone density in adult males. British Journal of Nutrition . 1999; 81:383-388.
11. Biggs H.G Moorehead,W R Determination of Serum calcium. Clin Chem. 1974; 20 ,1458 – 1460.
12. Mcleans FL, Hastings AB. The state of calcium in the fluids of the body. J Biol Chem 1935;108:285-322
13. Beeler MF, Catrou PG. Disorders of calcium metabolism. In: Interpretations in Clinical Chemistry: A Textbook Approach to Chemical Pathology. Chicago: American Society of Clinical Pathologist; 1983. p. 34-44
14. Daly J A and Ertingshausen G. Direct method for determining Inorganic Phosphorus in serum with centrichem. Clinical Chem 1972; 18: 263.
15. Wang J, Chen C C, Osaki S. Optimization of the phosphorus –UV reagent. Clin Chem.1983; 29, 1255.
16. Varley?s Practical Clinical Biochemistry 6th ed. Allan H.Goewenlock in “Separative Procedures Chromatography”. 1987; 34-85.
17. Pachathundikandi S. K, Veghese E.T. Blood zinc protoporphyrin serum total protein and total cholesterol levels in automobile workshop workers in relation to lead toxicity our experience. Indian J Clin Biochem; 2006; 21(2): 114-117.
18. Kopp SJ, Baron JT, Tow JP,. Cardiovascular actions of Lead and relationship to hypertension: a review. Environ Health Perspect. 1988; 78: 01-9.
19. Suma Vupputiri, Jiang He, Paul Muntner, Lydia A. Bazzano, Paul K. Whelton, Vecihi Batuman. Blood Lead Level Is Associated With Elevated Blood Pressure in Blacks Hypertension. 2003; 41:463.
20. Nilima N. Dongre, Adinath N.Suryakar, Arun J. Patil, Indira A. Hundekari, Basavaraj B. Devaranavadagi. Biochemical Effects of Lead Exposure on Battery Manufacture Workers with Reference to Blood Pressure, Calcium Metabolism and Bone Mineral Density. Published online Ind J Clin Biochem. 2012. DOI 10.1007/s12291-012-0241-8.

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





