IJCRR - 5(16), August, 2013
Pages: 54-62
Date of Publication: 28-Aug-2013
Print Article
Download XML Download PDF
AN EPIDEMIOLOGICAL STUDY OF LOW BIRTH WEIGHT IN A TERTIARY CARE HOSPITAL, TIRUPATI, ANDHRA PRADESH
Author: N. Swarnalatha, P. Bhuvaneswari
Category: Healthcare
Abstract:Objective: To know the prevalence of low birth weight and its association with socio demographic and maternal factors in Tertiary care Hospital, Tirupati. Settings: Government Maternity Hospital attached to S.V. Medical College, Tirupati Study design: Hospital based cross sectional study Participants: 1200 postnatal women who delivered single live baby in the Government Maternity Hospital, Tirupati. Methodology: Systemic random sampling Study Period: January 2011 to December 2011 Statistical analysis used: Chi-square test and binary logistic regression analysis Results: Prevalence of Low birth weight was 26.8%. The prevalence of low birth weight was high and significant in less than 20 years of age group (42.0%), illiterate mothers (37.4%), occupation as labor (27.4%), low income (28.5%), consanguinity history (38.7%), primigravida (29.8%), women of birth order 3 and above (33.3%), narrow birth interval (34.8%), gestational age less than 37 weeks (72.7%), weight gain less than 6 kgs (57.7%), height less than 145cms (51.0%), weight less than 45kgs (55.2%), low hemoglobin level, less than 3 ante-natal checkups (87.5%), IFA tablets not consumed or less than 50 tablets during pregnancy (48.0%), hard physical labor during pregnancy (56.4%), tobacco chewing (44.7%), female babies (30.6%) and obstetric complications during pregnancy (50.4%). sHowever residence of mother showed any significant effect on low birth weight. Conclusion: To emphasize on need of improving ante natal coverage as well as quality of services.
Keywords: Low birth weight, antenatal check up, IFA tablets, birth interval
Full Text:
INTRODUCTION
Children’s health is tomorrow’s wealth is one of the World Health Organization’s slogans of recent years. However, children’s health is to a great extent determined by factors that operate in utero, well before they are born. At birth fetal weight is accepted as the single parameter that is directly related to the health and nutrition of the mother, and on the other hand is an important determinant of the chances of the newborn to survive and experience healthy growth and development.[1] A multifactorial inter-relationship exists between the environment in which pregnant mothers live and the growth of the fetus.[2] This relationship has prompted public health personnel to suggest that birth weight distribution and the low birth weight babies to be considered as indicators of socioeconomic development. Low birth weight (LBW) (<2500 gms) is the strongest determinant of infant morbidity and mortality in India.
Low birth weight is one of the most serious challenges for mother and child health (MCH) in developing countries. It has been revealed that half of all peri-natal and one-third of all infant deaths occur due to low birth weight.[3] There is significant variation in the incidence of LBW across regions. According to the UNICEF, South Asia has the highest incidence, with 27% of all infants born in world with LBW, while East Asia/Pacific has the lowest (7%). Nearly 40% of all LBW babies in the developing world are born in India.[4] In India, the prevalence of LBW infants is about 28%,[4] as compared to 4.5% in industrially developed countries.[5] Low birth weight infants are three times more likely than normal birth weight infants to have neurodevelopmental complications and congenital abnormalities.[6] Among the factors that were identified by Kraemer[7] as possible determinants of LBW, maternal factors such as maternal weight and height, education, parity of the mother, gestational age, caloric intake, quality of antenatal care and sex of the delivered child were listed as prominent factors. The major challenge in the field of public health is to identify the factors influencing low birth weight and to institute remedial measures. Every pregnant woman irrespective of her risk status needs high quality maternal health services during pregnancy, delivery and postpartum period.[8] Some of the interventions suggested to reduce LBW include delaying child bearing in adolescents, efforts to improve the nutritional status of women, particularly anemia in pregnancy, access to antenatal care, advice on adequate rest during pregnancy, efforts to reduce tobacco chewing in areas wherever it is a common practice, improving female education, especially that of mothers.[9] Despite the benefits of adopting and implementing the primary health care system, health services have remained inaccessible in many respects and have therefore affected its optimum utilization. Hence there is need for further research in finding of the relation between low birth weight and maternal factors in order to decrease infant mortality rate and maternal mortality rate. In this context, this study is conducted to identify the epidemiological factors affecting birth weight and also to know the relationship of demographic, socio economic and obstetric factors with Low birth weight.
OBJECTIVE
To assess the magnitude of Low birth weight and factors contributing it
METHODOLOGY
A prospective, hospital based study was conducted in Government maternity hospital, Tirupati, a tertiary care hospital in Andhra Pradesh between January 2011 to December 2011. Sample size was 1200 calculated with 25% as the minimum prevalence of low birth weight, with 10% precision. Study variable: Maternal age, residence, maternal education and occupation, per capita income, parity, anthropometric measurements of mother, consanguinity history, birth interval, ANC checkups, iron and folic acid tablets consumption during pregnancy, anemia, gestational age, sex of the delivered child, weight gain, hard physical work , tobacco chewing and obstetric complications during pregnancy. Outcome variable: Low birth weight (LBW). Data collection method: 1200 postnatal mothers who delivered in the hospital during study period were included as study subjects and they were selected by systemic random sampling technique. They were interviewed using predesigned and pretested questionnaires and the information regarding the study variables were collected after obtaining consent form. The available records are also reviewed to collect the information regarding weight at first antenatal visit, last menstrual date and hemoglobin level.
Inclusion criteria: Singleton pregnant mother willing to participate in the study. Exclusion Criteria: Mothers with multiple pregnancy, mothers whose last menstrual period was not exactly known, ante-partum hemorrhage, caesarean delivery, neonates with congenital malformations, chromosomal anomalies and hemolytic disease of newborn. Birth weight less than 2500 g was used to label a child as LBW. Birth weight of every child was measured in gram within one hour after delivery using pretested and pre-calibrated Salter weighing machine (UNICEF). Protocol: In order to exclude inter-observer variation all measurements of study participants were taken by single investigator in the postnatal wards. Mother’s height was measured up to the accuracy of 0.5 cm by height measuring stand and weight was recorded on bathroom weighing machine up to the accuracy of 0.5 kg. Standardization of equipment was done to minimize error. The gestational age was calculated from the last menstrual period in completed weeks of gestation. Physical work during pregnancy was graded as described by Pachauri and Marvah in their study.[10] The data collected was complied, tabulated and finally analyzed. Descriptive statistics are reported as percentage. Group comparison was done by Chi-square test using SPSS package. P values less than 0.05 were considered as statistically significant.
RESULTS
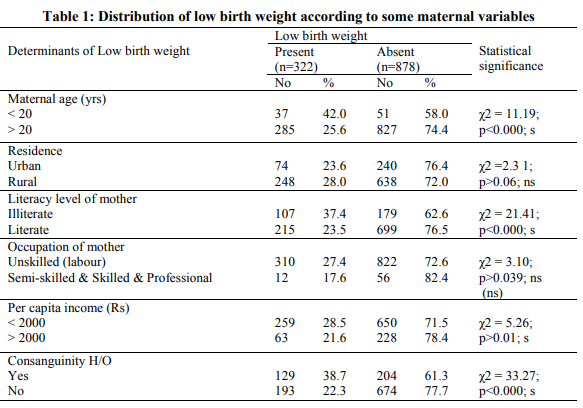
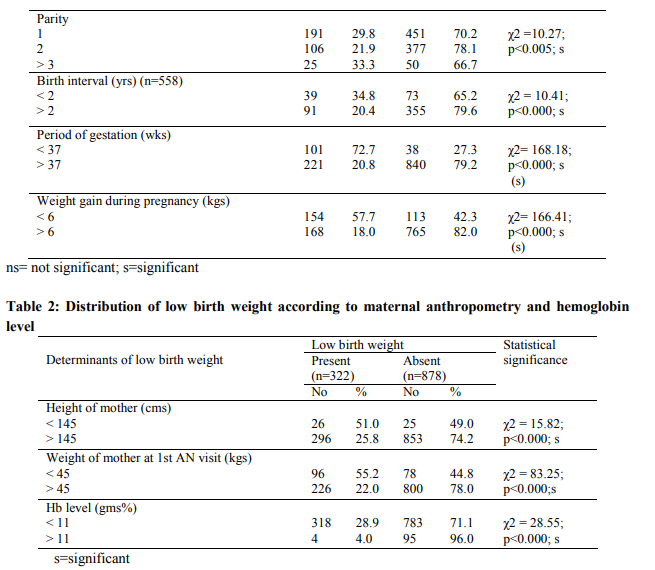
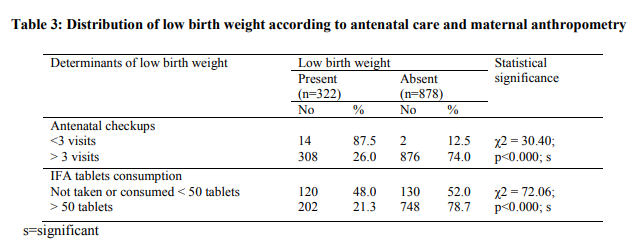
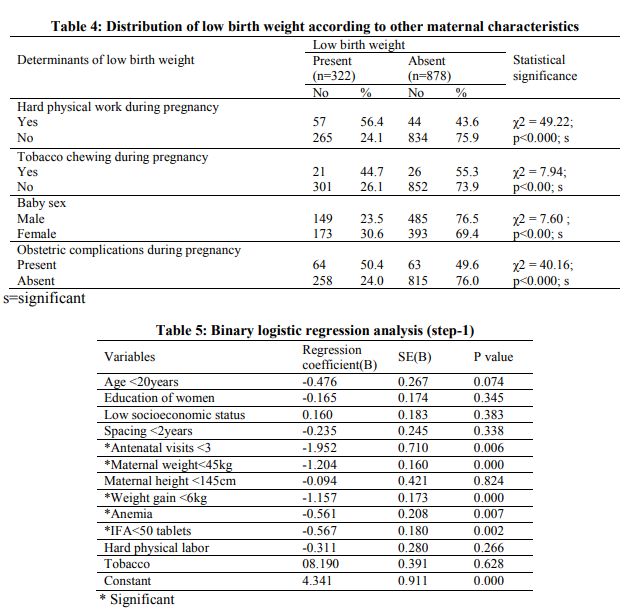
The proportion of Low birth weight in the present study was 26.8%. Table 1 summaries low birth weight according to some maternal variables. Significant association was found between Low birth weight and maternal age less than 20 years (χ2 = 11.19; p0.01), consanguinity history (χ2 = 33.27; p0.06) and occupation of the mother (χ2 = 3.10; p>0.039) has no significant association with low birth weight. Table 2 summarizes low birth weight according to maternal anthropometry and Hb% level. There was statistical significant association of low birth weight with maternal height less than 145cms (χ2 = 15.82; p<0.000), maternal weight less than 45kgs at first AN visit (χ2 = 83.25; p<0.000), and anemia (χ2 = 28.55; p<0.000). Table 3 summaries the effect of antenatal checkups and IFA tablets consumption on birth weight of new born. The birth weight of babies was influenced significantly by the number of antenatal checkups made by the mother and was significant (χ2 = 30.40; p<0.000). The statistical significant association was observed between LBW and IFA tablets consumption (χ2 = 72.06; p<0.000). Table 4 depicted low birth weight according to other maternal characteristics. LBW was highly significant among those mothers who were doing hard physical work during pregnancy (χ2 = 49.22; p<0.000), habit of chewing tobacco (χ2 = 7.94; p<0.00), female babies (χ2 = 7.60; p<0.00) and obstetric complications during pregnancy (χ2 = 40.16; p<0.000). Table 5 and 6 depicted that less than 3 antenatal checkups, maternal weight less than 45kg at first antenatal visit, less than 6 kgs weight gain during pregnancy, anemia and low IFA tablets consumption were the determinants of LBW.
DISCUSSION
The proportion of Low Birth Weight in the present study was 26.8 % while it was 21.5% from NFHS – 3[11] data. Higher proportion in our study could be due to the fact that high risk cases come for the delivery in hospital setting. A similar prevalence was found in Nasik study [12] and Chandigarh study [13]. The variation in the prevalence may be due to varying geographic and socioeconomic differences among the different communities. The study results establish that the prevalence of low birth weight is significantly associated with the mother’s age. The incidence of LBW was high among mothers less than 20 years of age (42.0%) which was statistically significant. Similar significant association was also reported by Velankar DH[8], Negi et al,[14] Kamaldoss et al,[15] and Anand et al,[16] in their respective studies. The birth weight improved with an increase in maternal age. Young age of mother and inadequate development of uterus can cause low birth weight babies. In current study, the proportion of low birth weight was high among those mothers residing in rural area (28.0%) and there was no statistical significant association of residential status of the mother and LBW. In present study, the proportion of low birth weight was found to be high among illiterate women (37.4%). The prevalence decreased with increasing the educational level of the women (23.5%). Sharma MK et al [13], Rizvi et al [17], Roudhari et al[18] and Mavalankar et al [19] showed significant association between maternal education and LBW. The high prevalence of low birth weight in relation to illiteracy may be linked to lower awareness levels regarding the need for antenatal care services and their utilization. The proportion of LBW was high in mothers who were laborers’ by occupation (27.4%) and it was not statistically significant. Same observation was documented in earlier studies. [16, 19, 20] High proportion of low birth weight was found in low income (28.5%). The proportion of LBW babies decreased with increase in the per-capita income of the family. There was statistical significance association between and LBW and family income. High prevalence of LBW in low socioeconomic status have also reported in other studies also. [8, 13, 19, 20] In current study the LBW prevalence was high among those mothers who gave history of consanguinity (38.7%) and it was statistically significant. In present study, it was observed that parity and low birth weight were co-related. Proportion of low birth weight increased with an increase in parity. This may be due to the fact that a large number of children are born without adequate spacing, leading to depletion in the woman’s nutritional status and health, leaving incapable of producing a healthy baby. In the current study, low birth weight was significantly found to be high in 3 or more than 3 para (33.3%). The studies in Dehradun, [14] Tamil Nadu, [15] and Karnataka [21] also found significant association of low birth weight with parity. The proportion of LBW was significantly high among those mothers with birth interval of less than 2 years (34.8%). Similar finding was revealed by the studies conducted in Mumbai [8] and Allahabad [22]. If women cannot recover from the effect of last pregnancy and period of breastfeeding before conceiving again, her nutritional status deteriorates with subsequent pregnancies. Hence, it is recommended to adopt birth spacing methods and widen the interpregnancy interval at least more than 2 years. This finding indicates the importance of birth spacing in preventing LBW babies. It was found that the period of gestation (<37 weeks) was statistically associated with LBW. Studies carried out in Lucknow [23] and Karnataka [24] have also found significant inverse association of low birth weight with gestational age. Though there is less scope to improve the gestational period through public health measures but improvement in other maternal factors like literacy, birth-spacing and reduced smoking level might improve the period of gestation and consequently improve the birth weight of the baby. Similar to present study significant relationship was found between maternal weight gain during pregnancy and the LBW in Nasik study[12] and other studies. [8, 15, 16, 24]
In the current study, the proportion of low birth weight was found to be high among those women with short stature (<145 cm) and it is statistically significant. Trivedi[5], Kramer[7] and Velankar DH[8] studies reported a significant association between maternal height and low birth weight. In the present study, the prevalence of the low birth weight was high among those women with weight less than 45kgs at first antenatal visit (55.2%) and it was statistically significant. Several studies [13,14,21,24] have also suggested that there was a significant association between maternal weight and LBW. Hence it is recommended to improve the nutritional status of a girl child throughout her life cycle as it will improve the nutritional status of women and will reduce the problem of LBW. In current study the prevalence of low birth weight was found to be significantly high in anemic women. Similarly other studies by Mavalankar et al. [19] and Joshi et al. [22] also reported significant relationship between mother’s hemoglobin concentration and the birth weight of the newborn. It is recommended that all efforts should be made to increase the Hb level by regular supplementation of iron and also by dietary modification. The proportion of LBW was high among mothers who had less than 3 required antenatal checkups indicating as a determinant of LBW. There was statistical significant association between antenatal checkups and LBW. Joshi et al.[22] and Idris et al.[23] also published the similar findings in their study. Association between irregular antenatal checkup and LBW may be due to noncompliance of advice/drugs during antenatal period. This emphasizes the need to improve both the coverage and quality of ante-natal care to reduce LBW which is the major cause of concern. The prevalence of low birth weight was found to be significantly high in women engaged in hard physical work in pregnancy (56.4%). Allahabad study [22] and Lucknow study [23] also reported statistical significant association between low birth weight and hard physical labor. A hard physical labor during pregnancy will upset the balance in women with marginal nutritional deficiencies and may also lead to early onset of labor causing prematurity. Due to the combined effects of vasoconstriction, myometrial contraction, reduced plasma volume, and diversion of blood flow away from the placental bed, there is diminution of utero-placental blood flow and resultant fetal hypoxia and result in fetal growth retardation. The prevalence of low birth weight was significantly high among tobacco users. The Nasik [12] study found significantly high proportion of low birth weight in relation to maternal tobacco exposure. Mehta et al. [25] also revealed that LBW proportion was high among tobacco users than among nonusers. It shows use of tobacco during antenatal period is associated with LBW. In the present study the proportion of low birth weight was significantly high in female babies and the same was also reported by Felke et al. study[26] and Allahabad study [22]. Mothers with bad obstetric history (BOH) delivered more number of LBW babies than mothers with no BOH and this accordance with other studies. [15, 16, 23] Binary logistic regression analysis has found out that the low birth weight is associated with risk factors like antenatal checkups, maternal weight less than 45kg, anemia, weight gain less than 6kg, low IFA tablets consumption during pregnancy. Various studies conducted in various parts of India after multivariate analysis or multi regression analysis was found that antenatal visits , age of the mother, socioeconomic status, maternal height less than 145cm, maternal weight less than 45kg, birth spacing less than 2years, weight gain during pregnancy, gestational age and anemia are the determinant factors for low birth weight.[8,21,23,24]
CONCLUSION
As there are several factors interacting in this phenomenon so it is not feasible to single out any particular factor affecting low birth weight. Among various epidemiological factors the maternal factors like maternal age, regular antenatal checkup, parity, birth interval, anemia, bad obstetric history, hard physical work, tobacco chewing during pregnancy were significant determinants of LBW. This study shows ineffectiveness of existing national programs for improving the antenatal care. Hence, it is the need of the hour to strengthen the existing maternal services at the basic level of community i.e., at door steps of the beneficiaries if possible. There is a need to promote right age at marriage (minimum 18 years). Inter pregnancy interval may be improved through different contraceptive methods of spacing. The study suggests focusing attention on health education of prospective mothers and discouraging teenage pregnancy.
ACKNOWLEDGEMENTS
The author extends the profound sense of gratitude to the study participants. Author acknowledges the immense help received from the scholars whose article cited and included in references for this manuscript. The author is also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript
References:
1. Wicox AJ, Skaeven R. Birth weight and perinatal mortality. The effect of gestational age. Am J Public Health 1992; 82:378-83.
2. Makhija K, Murthy GVS, Kapoor SK, Lobo J. Socio-biological determinants of birth weight. Ind J Paed 1989; 56:639-43.
3. Harfouche JK. WHO bulletin 1979:3; 387- 403.
4. UNICEF. Childinfo, Monitoring the situation of children and women, cited April 25, 2012 available at http://www.unicef.org/infobycountry/India_sta tistics.html.
5. Trivedi CR, Mavalankar DV. Epidemiology of low birth weight in Ahmedabad. Ind J Paed 1986; 53:795-800.
6. Lt.Col Singh G, Capt. Chouhan R and Major Sidhu K. Maternal factors for low birth weight babies. Medical journal Armed Forces India, 2009; 65(1):10-12.
7. Kramer MS. Determinants of low birth weight. Methodological assessment and metaanalysis. Bull of World Health Organization 1987; 65(5): 663-737.
8. Velankar DH. Maternal factors contributing to Low birth weight babies in an urban slum community of Greater Mumbai. Bombay Hospital Journal. 2009; 51(1):26-35.
9. Sachdev HP. Low birth weight in South Asia. Int J Diab Dev Ctries 2001; 21:13-33.
10. Pachauri S, Marvah SM. Socioeconomic factors in relation to birth weight. Indian Pediatr 1970; 7:462-8.
11. International Institute of Population Sciences, National Family Health Survey, India; 2005- 06 (NFHS-3, vol1) 2007; 223.
12. Sachin S Mumbare, Girish Maindarkar, Rajesh Darade, Surekha Yenges, Madhav kumar and Kiran Patole. Maternal Risk Factors Associated with Term Low Birth Weight Neonates: A Matched-Pair-Case Control Study. Indian Pediatrics. 2011; May 30.
13. Sharma MK., Kumar D, Huria A and Gupta P: Maternal risk factors of Low birth weight in Chandigarh India. The internet Journal of Health. 2009; 9(1):DOI:10.5580/10f1
14. Negi KS, Kandapal SD, Kukreti M. Epidemiological factors affecting low birth weight. J K Science, Journal of Medical Education and Research 2006; 8(1):31-34.
15. Kamaladoss T, Abel R, Sampathkumar V. Epidemiological correlates of low birth weight in rural Tamil Nadu. Ind J Pediatr 1992; 59(3):299-304.
16. Anand K, Garg BS. A study of factors affecting Low birth weight. Indian J Com Med 2000; 25(2): 57-62.
17. Rizvi SA, Hatcher J, Jehan I and Qureshi R. Maternal risk factors associated low birth weight in Karachi: A case control study. Eastern Mediterranean Health Journal 2007; 13(6): 1343-52.
18. Roudhari M, Yaghmaer M and Soheili M. Prevalence and risk factors of low birth weight infants in Zahedan, Islamic Republic of Iran. Eastern Mediteranean Health Journal 2007; 13(4); 838-45.
19. Mavalankar DV, Gray RH, Trivedi CR. Risk factors for preterm and term low birth weight in Ahmedabad. Indian Journal of Epidemiology 1992; 21(2):263-72.
20. Kiran A, Garg BS. A study of factors affecting LBW. Indian Journal of community medicine 2000;25:57-62
21. Acharya D, Nagraj K, Nair NS, Bhat HV. Determinants of Intrauterine Growth Retardation: A Case Control Study in Udupi District, Karnataka. Indian Journal of Community Medicine.2004; 29(4):181-82.
22. Joshi HS, Subba SH, Dabral SB, Dwivedi S, Kumar D, Singh S. Risk factors associated with Low birth weight in newborns. Indian Journal of Community Medicine. 2005; 30(4): 142-3.
23. Idris MZ, Gupta A, Mohan U, Srivastava AK, Das V. Maternal health and LBW among institutional deliveries. Indian J Community Med 2000; 25(4):156-60.
24. Phaneendra Rao RS, Prakash KP, Sreekumaran Nair N. Influence of PrePregnancy Weight, Maternal Height and Weight Gain During Pregnancy on Birth Weight. Bahrain Medical bulletin 2001; 23(1):1-8.
25. Mehta A, Shukla S. Tobacco and pregnancy. J Obstet Gynaecol India 1990; 40:1556-60.
26. Felke Y, Enquoseassie F. Maternal age, parity and gestational age on the size of newborn in Addis Abab. East Africa Medical journal 1999; 76(8):468-71.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





