IJCRR - 5(16), August, 2013
Pages: 27-30
Date of Publication: 28-Aug-2013
Print Article
Download XML Download PDF
DUPLEX APPENDIX: A MORPHOLOGICAL, EMBRYOLOGICAL AND APPLIED ASPECT
Author: Vandana Dave, Hitendra Kumar Loh, Avinash Thakur, Rajesh Kumar Suri
Category: Healthcare
Abstract:The vermiform appendix has been noted as a vestigial structure that has lost most of its original functions through the process of evolution. Duplication of appendix is extremely rare congenital entity which can be related with other anomalies of gastrointestinal tract. Double appendix represents a challenging clinical scenario in cases of right lower quadrant pain. In the present study we report a peculier case of double appendix. Understanding of appendiceal duplication is essential for clinicians to prevent acute and serious intestinal, genitourinary conditions; for surgeons performing surgeries and for medico legal connotations.
Keywords: vermiform appendix, vestigeal, appendicitis, double appendix.
Full Text:
INTRODUCTION
The vermiform appendix is positioned at the commencement of the large gut and has the same basic structure. It is an elongated tubular cul-desac connected to the caecum situated in the right iliac fossa of the abdomen. Though proposed as vestigeal in humans after losing its original functions during evolution, it still serves as a significant lymphoid organ. Large masses of confluent lymphatic nodules in the walls of appendix contain germinal centers for local defense against infection and make up a part of Gut Associated Lymphoid Tissue (GALT). It is presumed that these are homolog of the avian bursa of fabricus related to the acquisition of immunological competence by certain lymphocytes. In lower mammals particularly herbivores, the caecum and appendix are large and significant sites of digestion of cellulose by symbiotic bacteria1 . Though the length and position of the appendix exhibit normal anatomical variations, its duplication is a rare occurrence reported with an incidence of 0.004% 2 . The first case of appendix duplex was reported in a female patient who had associated anomalies of duplication of entire large bowel, two uteri with two vaginae, ectopia vesicae and exomphalos3 . Most anomalies of appendix have been observed in adults and most were noticed incidentally during surgery not primarily involving the appendix 4 . The complications that might arise from an unidentified duplicate appendix may have serious, life-threatening consequences for the patient.
Embryological Aspect:
Initially the appendix is a tiny diverticulum of the caecum. It increases rapidly in length. At birth it is relatively a long tube arising from the distal caecal end. After birth the right wall of the caecum grows excessively and pushes the appendix medially5 . The appendix is subject to considerable, positional variations. It may pass posterior to the caecum (retrocaecal appendix) or colon (retrocolic appendix) or it may descend on the pelvic brim (pelvic appendix). Although In majority of people (64%), it is retrocaecal in position5 .
CASE REPORT
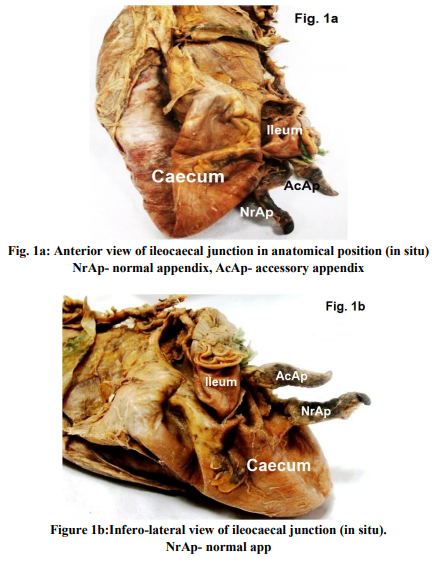
During routine dissection hall teaching curriculum of medical undergraduates, two appendices, normal and accessory were identified in a 56 years old male Indian cadaver. The normal appendix was subcaecal in position situated 2 cms below the ileocaecal junction and had a patent lumen. This appendix measured 3.1 cms in length from its base to the tip. The maximum outer diameter using vernier calipers was 0.9 cms. The accessory appendix was positioned at iliocaecal junction along the taenia line. It was smaller than the normal appendix and measured 2.6 cms in length from its base to the tip. The maximum outer diameter measured 0.4 cms. It was found in promonteric position. The lumen of this accessory appendix was obliterated. Both the appendices had mesoappendix containing appendicular artery at their free margin. The respective appendicular arteries were branches of iliocolic artery. Histologically, both appendices revealed normal mucosa, submucosa, muscularis externa and serosa.
DISCUSSION
Double appendix is usually asymptomatic. Accessory appendices are mostly diagnosed during abdominal surgeries, postmortem examination or on barium enema studies6 . Appendiceal duplication was first classified by Cave in 19367 . Wallbridge and Waugh in 1963 worked on the appendiceal duplication and divided these duplications into three groups as Type A, Type B and Type C8 . Type A consists of various degrees of partial duplication on a normally localized appendix with a single caecum. Type B consists of a single caecum with two completely separated appendices. Type B is divided further into two subgroups. B1 group includes two appendices localized symmetrically on either side of the ileo-cecal valve; this resembles the normal phylogenetical arrangement in birds, so this group was called the ‘bird-like or avian’ type. In B2 group (taenia-coli type) there is a normally localized appendix arising from the caecum at the usual site and a second, separate, rudimentary appendix localized along the taenia line. In type C there are two caeca, each bearing its own appendix8 . Some cases are difficult to categorize into a suitable type so the authors started to add additional types. Type D includes a horse-shoe appendix with two opening at the common caecum9 . The present case can be compared with type ‘B2’ variety, as one appendix arose from the normal site while the other accessory appendix which was smaller in size rather rudimentary, arose from the ileo-caecal junction. Most of the cases of double appendix studied by Wallbridge were of the ‘B’ type; out of the 50 reported cases, 30 were of this variety8 . Phylogenetically, the appendix is absent in several species like Felis (tiger, leopard, lion) and Canis (dog, wolf, fox) 10. Morphologically there is no reason why the human being might not have two appendices. Duplication is said to be possible in any part of gastrointestinal tract11. Aetiology of the double appendix has been explained by many workers. Environmental factors such as trauma or hypoxia during early fetal development have also been suggested to play a role11. Despite normal embryogenesis, the pathogenesis of appendiceal duplication is yet unclear. There are four theories to explain the embryology of gastrointestinal duplication namely the split notochord theory, the median septum formation, failure of the normal regression of embryonic diverticula and partially twinning procedure12. Embryogenesis of appendiceal duplication can be explained to some extent by the theory of ‘failure of the normal regression of embryonic diverticula’. Cave explained the embryological basis of its occurrence by referring to the work of Kelly and Hurden, Gladstone and Wakeley and emphasized that a transient appendix develops from the tip of the caecum at the beginning of the 5th week, atrophies at the 7th week and disappears soon after7 . The normal vermiform appendix differentiates later. The transient appendix may be substantiation of ancestral caecal duplicity in mammalia7 .
APPLIED ASPECT
The anomalies of appendix detected during childhood are always associated with severe intestinal, genitourinary or bony malformations, seen most often in conjunction with Type B1 and Type C duplication13. Carcinoma of the intestinal tract with coexistent duplication has also been reported. This condition is very rare and appears limited to a few number of cases14, 15 . In case of double appendix, the symptoms are usually the result of obstruction and inflammation of the bowel. In patients with appendiceal duplication, it has been reported that acute appendicitis occurs in one16 or both11 appendices and reoccurs six years after the first appendectomy17. In patient with appendicular duplication both appendices are removed whenever one is found inflamed. This is done to avoid diagnostic confusion that may arise on removal of a single appendix 11. The clinical presentation can vary according to the location of the appendices. Anomalies of the appendix such as duplication and malposition are of great practical importance and a surgeon must acknowledge this fact during operations.
CONCLUSION
A double appendix is rather rarest which accounts for surgical complications or may be associated with a carcinoma of gastrointestinal tract. Embryologically this duplication occurs due to the failure of normal regression of embryonic diverticula. Acknowledging such appendiceal duplications can circumvent diagnostic perplexity and help clinicians foresee acute or chronic intestinal or genitourinary conditions.
References:
1. Williums PL, Bannister LH. The anatomical basis of medicine and surgery. ELBS with Chrchil Livingstone Grays Anatomy.1995; 38th ed. pp 1775-76.
2. Kjossev KT, Losanoff JE. Duplicated vermiform appendix. Br J Surg. 1996; 83; pp 1259.
3. Picoli G. (Quoted by Gupta and Kak, 1964) Progresso Medico (Napoli). 1892; 6; pp 32.
4. Eroglu E, Erdogan E, Gundogdu G, Dervisoglu S, Yeker D. Duplication of appendix vermiformis : a case in a child. Tech Coloproctol. 2002; 6; pp 55-57.
5. K. L. Moore, T.V.N. Persaud. The developing human, clinically oriented embryology. 2009; 8 th ed. pp 227-229.
6. Mitchell IC, Nicholls JC. Duplication of the vermiform appendix. Report of a case: Review of classification and medico legal aspects. Medicine, Science, Law. 1990; 30(2); pp 124- 26.
7. Cave AJE. Appendix vermiformis duplex. J Anat. 1936; 70; pp 283-292.
8. Wallbridge PH. Double appendix. Br J Surg. 1963; 50(221); pp 346- 347.
9. Drino E, Radnic D, Kotjelnikov B, Aksamija G. Rare anomalies in the development of the appendix. Acta Chir Iugosl. 1991;38; pp 103- 11.
10. Chew DK, Borromeo JR, Gabriel YA, Holgersen LO. Duplication of the vermiform appendix. J Pediatr Surg. 2000; 35; pp 617- 618.
11. Bishop HC, Koop CE. Surgical management of duplications of the alimentary tract. Am J Surg. 1964; 107; pp 434-442.
12. Jimenez SG, Oliver MR, Stokes KB, Morreau PN, Chow CW. Case report: Colonic duplication: a rare cause of obstruction. J Gastroenterol Hepatol. 1999; 14; pp 889–892.
13. Tinckler LF. Triple appendix vermiformis: a unique case. Br J Surg. 1968;55; pp 79-8.
14. Holcomb GW 3rd, Gheissari A, O'neill JA Jr, Shorter NA, Bishop HC. Surgical management of alimentary tract duplications. Ann Surg. 1989; 209; pp 167-174
15. Chen CC, Yeh DC, Wu CC, Li MC, Kwan PC. Huge cystic duplication of the ascending colon in adult. Zhonghua Yixue Zazhi (Taipei). 2001; 64; pp 174-178
16. Griffiths EA, Jagadeesana J, Fasihe T, MercerJonesa M. Bifid vermiform appendix: a case report. Curr Surg. 2006; 63; pp 176-178.
17. Travis JR, Weppner JL, Paugh JC. Duplex vermiform appendix: case report of a ruptured second appendix. J Pediatr Surg. 2008; 43; pp 1726–1728.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





