IJCRR - 5(20), October, 2013
Pages: 81-88
Date of Publication: 02-Nov-2013
Print Article
Download XML Download PDF
UTILIZATION OF THE KISHORI SHAKTI YOJANA SERVICES BY THE ADOLESCENT GIRLS IN URBAN SLUM OF MUMBAI
Author: Shobha Kowli, Padmavathi Dyavarishetty
Category: Healthcare
Abstract:Objectives: Kishori Shakti Yojana, a programme under the Integrated Child Development Scheme aims to improve nutritional status of the girls and empower the adolescent girls through life skills education. The aim of the study was to assess the utilization of the Kishori Shakti Yojana by the adolescent girls and identify reasons for non-participation. Materials and Methods: A descriptive cross-sectional study in urban slum using a systematic random sampling method of households to obtain a sample size of 10% of adolescent girls (11-18 years). Results: The mean age of the 943 adolescent girls interviewed was 14.21 years. Eighty eight percent were currently studying. Around 52% girls were aware about ICDS but only 15% were registered. The ever utilisation of the services by the girls is extremely low at 8%. Reasons for poor utilisation of the services were lack of awareness about the services, community's perception that the services are not needed by them, and lack of suitable timings. Girls explicitly suggested Saturday and Sunday afternoons as being the most suitable time. Conclusions: The programme strategies should be designed taking into account the rural and urban difference for a succesful implementation. In the urban areas where majority girls are school going the programme could be well implemented by the educational institutes rather than the anganwadi centres.
Keywords: Adolescent Girls, Kishori Shakti Yojana, Integrated Child Development Scheme
Full Text:
INTRODUCTION
Studies across India have shown that health and nutritional status of adolescent girls (10-19 years of age) is poor. The girls also face greater social disadvantge and generally are lesser educated. Adolescent girls do not have adequate access to vital health and nutrition information or services; generally get married at an early age and are caught in the cycle of early pregnancy, childbearing and child rearing. Girls usually drop-out of school after completing primary education because of responsibility of household chores, to take care of younger siblings, distance from school, lack of female teachers and fear for safety. National Family Health Survey – 3 (NFHS-3) has found that 11.7% of the girls between 15-19 years are stunted, 47% are underweight and 56% are anaemic(1). Most girls have little knowledge of menstruation, sexuality and reproduction as shown by several studies (2-6).
A special intervention called as ‘Kishori Shakti Yojana’ (KSY)(7) was devised for adolescent girls using the ICDS (Integrated Child Development Scheme) infrastructure based on the experiences of empowerment programmes conducted by NGOs and researchers in India.
Kishori Shakti Yojana aims to improve the nutritional and health status of girls in the age group of 11-18 years and promote awareness of health, hygiene, nutrition and family welfare, home management and child care through the nutrition health education programme and administration of iron folic acid tablets as supplement(7). Life Skills education programme is another important component of the KSY(7). Non-formal Education of adolescent girls with particular attention to school dropouts and ensuring functional literacy among illiterate adolescent girls is another major component of KSY(7). Vocational training activities are undertaken for adolescent girls for their economic empowerment through this scheme. A large number of adolescent girls have utilised the various components of the Kishori Shakti Yojana as evident from the last three years performance report of the Kishori Shakti Yojana programme(8).
However it was observed that the girls in the community were not consuming Iron Folic Acid (IFA) tablets. Those who received the IFA tablets would just discard it. Knowledge about nutrition and health was also poor. The proposed study therefore aims to assess the utilization of the Kishori Shakti Yojana by the adolescent girls and identify reasons for non-participation of the adolescent girls in the Programme.
MATERIALA AND METHODS
The present study conducted in an urban slum of Mumbai in the F/N ward with the help of ICDS supervisors and the health post staff comprised of 1,07,817 population; 25309 households and 7297 adolescent girls. A descriptive cross-sectional study design was adopted. The study participants were the adolescent girls aged between 11-18 years old. A written informed consent was obtained either from the girl or from their mother/ guardian in cases of girls below 18 years of age.
Sample size was calculated as 10% of the adolescent girls population in the study area which worked out to be 880 adolescent girls assuming a non-response rate of 20%. It was estimated that 3052 houses would need to be visited in the study area so as to meet the target of 880 adolescent girls. Sampling technique was the Systematic Random Sampling with household as the unit of sampling. If a particular household had more than one girl then the youngest adolescent girl was interviewed. The study was conducted over a period of one year between 2011-2012.
The survey was carried out as per ICDS supervisor’s area. The first household was selected by randomly picking a ten rupee currency note and noting its last digit number to select the first household for survey. All the subsequent households were selected as the eighth household from the last enumerated. If any eighth household was locked then the next eighth household was selected and the procedure repeated. The total respondents for the survey were 943 adolescent girls. A pre-tested structured questionnaire with open and closed type of questions in Hindi language was used for interviewing the adolescent girls. Questionnaire explored aspects regarding participation, knowledge, and suggestions for improving the Kishori Shakti Yojana.
RESULTS
Demographic and Social characteristics of study group
A total of 943 adolescent girls were interviewed amongst the 3082 households visited. The mean age of the girls was 14.21 years. Majority of the girls belonged to the age group of 11-14 years (55.8%) and were predominantly Hindus (74.4%).
Almost 88% girls (829) were currently studying. Of the 114 girls not currently studying, almost all perceived education as important, however only 43.9% girls desired to continue their studies. Majority of the 104 girls, who had received 10 or less than 10 years of schooling, discontinued their education primarily due to poor scholastic performance (25%) and family reasons (21%). Family reasons included poor economic status of the family, responsibility of house hold chores and siblings, death of parent etc. Almost 8% of the girls cited health reasons like suffering from TB as a reason for discontinuing their education. A substantial number of girls (12%) were not interested in studies. Only three girls were married; one was married at the age of 12 years and the other two at the age of 17 years. None of them had children.
Awareness about Anganwadi centre and its services
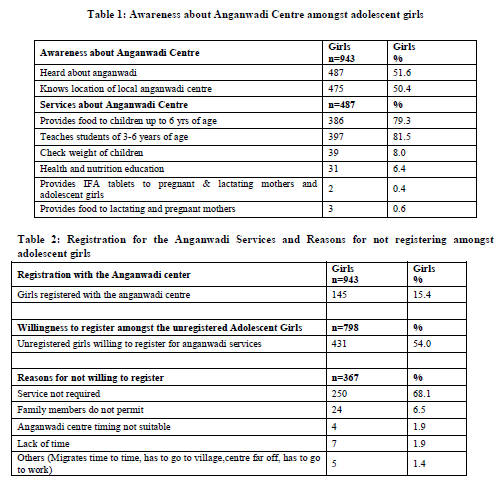
Only 2 adolescent girls were aware about the Kishori Shakti Yojana who had obtained the information from the school. It is seen from Table 1 that Anganwadi centre and its location was known only to 50% girls. Anganwadi centres are synonymous with the Balwadis and are known for its preschool education and food supplementation programme for the underfive children. Awareness about services for the pregnant and lactating mothers was very low.
Table 2 shows that only 15% girls have registered with anganwadi centre. Most of them had received information from the anganwadi worker (96%). Of the unregistered 798 girls, only half of the girls were willing to register their names with the anganwadi centre. The reason given by majority of the girls who were not willing to register in anganwadi was the belief that the services of anganwadi were not required by them. Other reasons included reluctance from the family to send them to the anganwadi centre, lack of time and unsuitable timings.
Utilisation of Anganwadi services
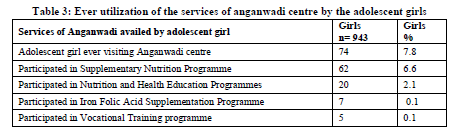
The ever utilization of the anganwadi services was only 7.8%. Thirty Five adolescent girls were currently visiting anganwadi and 49 had visited the centre in the past. From table 3, it is seen that the most commonly utilised services were supplementary nutrition programme and health education programmes/meetings.
Supplementary nutrition programme
Only 7% (62) of the adolescent girls were availing supplementary food services provided by anganwadi. About 70% of these 62 girls utilized the services in the last six months. A majority of the girls (53) were satisfied with the services.
Iron Folic Acid (IFA) Supplementation Programme
The percentage of adolescent girls consuming IFA tablets from anganwadi was very low. Only 7 girls said that they were consuming IFA tablets. All the adolescent girls were consuming these tablets for less than 6 months on the advice of the Anganwadi worker. The pattern of consumption was mostly daily. None complained about side-effects.
Health Education Programmes/Meetings
The topics on which health education was imparted were nutrition, menstrual hygiene and personal hygiene. Sixteen of the twenty girls attending health education programmes reported satisfaction with the programmes conducted for them.
Vocational Training
Vocational skills training programmes such as computer training, mehendi and English speaking courses were organised through ICDS and were attended by only 5 girls. Out of them, 3 were satisfied with the training. The suggestions from the girls regarding vocational training were that classes should be conducted on beautician course (37%), tailoring (17%) and computer classs (10%).
Reasons for not participating in the various service components
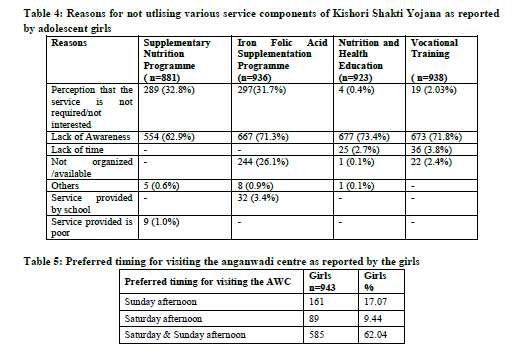
It is seen from table 4 that lack of awareness is the predominant reason for the non-utilisation of the services. Around 63%-73% girls cited lack of awareness for non-utilisation of supplementary nutrition, iron folic acid supplementation, nutrition and health education and vocational training programmes.
Nutrition and Iron Folic Acid supplementation was perceived as not required by 32%-33% of the girls. Another 244 girls reported that the iron folic acid (IFA) tablets were not available at the anganwadi centre. Thirty two girls reported receiving IFA tablets from schools and therefore did not require to take it from anganwadi. Other reasons for not consuming IFA were side-effects, lack of time and discouragement from family members for consuming IFA tablets.
Suggestions for improving the ICDS/KSY
A few important suggestions for improving the anganwadi services were; to use television to publicise anganwadi; anganwadi should have its own premises; facility should be clean, bigger and open on time. Medicines should be provided. No concrete suggestions were given by girls for supplementary nutrition, except one girl who said quality of food in terms of cleanliness and taste should improve.
Suitable Timing for Girls to attend Anganwadi Centre
It is seen from Table 5, that the majority of the respondents felt that Saturday and Sunday afternoon was the most convenient time to visit the AWC.
DISCUSSION
The study aimed at finding out utilization of services of Kishori Shakti Yojana (KSY) specially designed to serve the prospective mothers of the society. The adolescent girls in the age group 11 – 18 years contributed to about 10% of urban population which matches with Indian average figure of 10%(9.10).The predominant religion in this area is Hindus followed by Muslims. Only three girls are found to be married but none of them had children. Thus the age of marriage atleast in the urban slums is above 18 years of age.
The present study found that 88% girls are studying currently as compared to the findings of the evaluation of KSY programme in Uttar Pradesh and Rajasthan(11) where almost 65% girls were not studying. The educational status of urban girls is thus better compared to their rural counterparts in northern India. Those girls who had discontinued their studies before or after 10th standard had given reasons like poor scholastic performance or disinterest in the studies. Economic reasons and family responsibilities were the reasons for discontinuation of studies in about one-fifth of the girls. Partnerships with Non-Governmental Organizations to support educational coaching classes will probably be able to reduce school drop-out.
The girls were not aware about Kishori Shakti Yojana in the present study. This is in contrast to the awareness about the scheme in Uttar Pradesh and Rajasthan where more than 50% were aware about the scheme(11). Even though the awareness about KSY is poor a large number of girls knew about anganwadi centre and its location. Anganwadi is however more known for its nutrition supplementation and non-formal education to children below 6 years of age. Growth monitoring, Nutrition and health education programmes were known only to few girls.
Only 15% girls were registered with local anganwadi in contrast to 90% observed in Uttar Pradesh and Rajasthan(11). However almost half of the unregistered girls showed their willingness to get registered. Amongst the registered girls, only a few were currently visiting the anganwadi either for food supplementation or meetings. Majority of these girls were satisfied with the work of anganwadi. Thus in urban area if adolescent services are desired to be delivered properly, ICDS will have to market them through social media.
The few who were attending were satisfied with the services and could be used as motivators to get their peers to anganwadi. Ignorance about Nutrition Health Education sessions, IFA supplementation programme, food supplementation and vocational training provided by anganwadi was the major contributory factor for poor utilisation.
About one-third girls also felt that services of anganwadi were not needed. There were many complaints like lack of information regarding services available, unclean surroundings, centre not opening on time, medicines not being available, lack of space etc. Lack of time was the reason given by hardly a few beneficiaries.
Thus it is seen that inadequate propaganda is the main reason behind non-utilization of the services. Nutrition and health education sessions if promoted in the community will sensitize the mothers and girls about the need of IFA and food supplementation. Advertising about Anganwadi centre and its services on television was one of the suggestions given by the girls. Mass media and community mobilization efforts that engage influential adults such as parents, teachers, community and religious leaders, as well as pop stars and sports stars can positively affect the norms of behavior of the adolescents and youth (12).
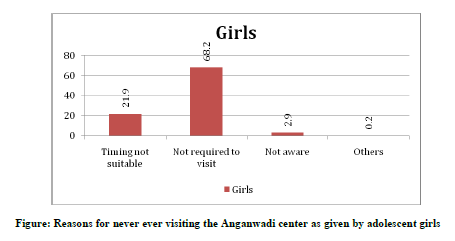
One-fourth of the girls who had availed the services in the past said that the reason for discontinuation was lack of suitable timings. A similar proportion of girls who had never visited the anganwadi cited the same reason. Anganwadis function only in the morning time when majority of girls(88%) go to schools or colleges. So it is obvious that anganwadi timings were not suitable to them. Many of the girls suggested saturday and sunday afternoons as more suitable timing. Logistics of this arrangement will have to be seen by ICDS scheme. But certainly community based organization and local NGOs can join hands.
The consumption of IFA tablets by the girls is extremely low. As large number of girls are attending either school or colleges, colloboration between the health departmental and educational institutes would be a cost-effective intervention. The education department could make it mandatory for all the public and private institutes to implement the IFA supplementation programme. This colloboration will take care of a large proportion of adolescents who are still studying and only a few adolescents girls who are not attending school will need to be covered by the health department.
As far as Food supplementation is concerned, the girls have expressed concern about cleanliness and quality of food. They suggested that milk, eggs, fruits, and rawa should be given. More number of Nutrition and Health education programmmes should be conducted in the community so as to improve their participation in the IFA supplementation, supplementary nutrition and vocational skills training programmes.
The girls are interested in vocational skill development services. Suggested courses like beautician course, tailoring and computer training reflects the girls preference for self employment or work from home opportunities. Thus providing them with much needed vocational training programme, the utilization of other service components will increase.
Kishori Shakti Yojana is now converted to the more ambitious SABALA yojana which also involves field visits of the girls to different institutions like banks and post office etc. The idea is indeed very praiseworthy but blind duplication of rural setting in urban slums will be very dangerous and futile. The urban areas need a different approach. There is multiplicity of services for primary health and empowerment of girls through local health and education agencies. However the coordination between these agencies is unfortunately lacking. The problem is complicated by private health and education service providers in urban areas. Thus in an urban area, with a political will, the education and the health departments could make more relevant and coordinated efforts to empower the women of India and make them SABALA in true sense.
CONCLUSIONS
The services of ICDS for the adolescent girls namely the Kishori Shakti Yojana is poorly utilised by the girls in urban slums of Mumbai. The three common reasons for poor utilisation were lack of awareness about the services; perception that the services are not required by them and lack of suitable timings. In urban areas, where majority of the adolescent girls are studying, Kishori Shakti Yojana/SABALA, could be implemented in colloboration with the education department in the schools and colleges, which is a feasible option. The Anganwadi Centres could focus only on the small segment of non-school/non-college going adolescent girls. The participation of these girls could be improved by active propoganda of the ICDS services, creating a demand for the services and organizing the services at a time that is suitable and convenient for the girls. Vocational skills training can be augmented by linking with other community based NGOs with special emphasis on beautician`s training, tailoring and computer training. Thus a strategic plan to complement the availability of services and increase demand of the services can improve utilization of services.
ACKNOWLEDGEMENT
We are thankful to Indian Council of Medical Research for financial support to conduct the research (ICMR File No. 5/11/17/2010-SBR).
References:
- NFHS-3 Final Report, http://www.rchiips.org/nfhs/nfhs3.shtml, accessed on 24-08-2013
- Rama Rao A.(1963). A study on menstruation in adolescents. Journal of Indian Medical Association, 40 (1): 15-19.
- Khanna A., Goyal R.S. , Bhawsar R.(2005). Menstrual practices and reproductive problem. A study of girls in Rajasthan. Journal of health management, Vol: 7 (1) pg 91-107.
- Deo D.S., and Ghattargi C.H. (2005). Perceptions and Practices Regarding Menstruation: A Comparative Study in Urban and Rural Adolescent Girls. Indian Journal of Community Medicine, Vol. 30, No. 1, January-March, 2005
- Quazi S.Z., Gaidhane A., and Singh D. (2006). Believes and Practices regarding menstruation among adolescent girls of high school and Junior college of rural areas of Thane district. . Journal of DMIMSU, Dec 2006, Vol 2, Page 67-71.
- Dasgupta A and Sarkar M (2008). Menstrual hygiene among adolescent girls. Indian Journal of Community Medicine, Vol. 33, Issue 2. Page 77-80
- Guidelines for Implementation of Adolescent Girls Scheme as a component under centrally sponsored ICDS (general) scheme, F.no.5-5/2000-CD-I, Government of India, Ministry of Human Resource Development, Department of Women and Child Development, New Delhi
- http://wcd.nic.in/projsanc/ksy06-09.htm, accessed on 24-08-2013
- http://censusindia.gov.in/2011census/censusinfodashboard/stock/profiles/en/ ND_India.pdf, accessed on 24-08-2013
- http://www.censusindia.gov.in/Census_Data_2001/India_at_glance/popu1.aspx, accessed on 24-08-2013
- Kishori Shakti Yojana (KSY), Under the ambit of ICDS,In Uttar Pradesh and Rajasthan,2006 , Ministry of Women and Child Development, Government of India, Formative Research and Development Services, New Delhi
- http://siteresources.worldbank.org/HEALTHNUTRITIONANDPOPULATION/Resources/281627-1095698140167/Rosen-AHDFinal.pdf, accessed on 24-08-2013
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





